This retrospective, cohort study included IVF PGT-M cycles evaluated by the Genetics Laboratory in Assuta Tel Aviv Medical Center from 2018 to 2022. The study group included PGT-M cycles performed for male and female patients diagnosed with BRCA 1/2 mutations (cases). Cases were compared to PGT-M cycles tested for other mutations with dominant inheritance (MD or PKD) from either the male or female partner (controls).
Ethics
The study was approved by the Ethics Committee of Assuta Tel Aviv Medical Center (approval number 0092 − 21 ASMC). All patients a genetic consultation prior to a PGT cycle and therefore all patients who were eventually included in this study expressed their wish to perform an IVF PGT-M cycle for this indication. Written informed consent was not required for this retrospective study.
Pre-implantation genetic testing
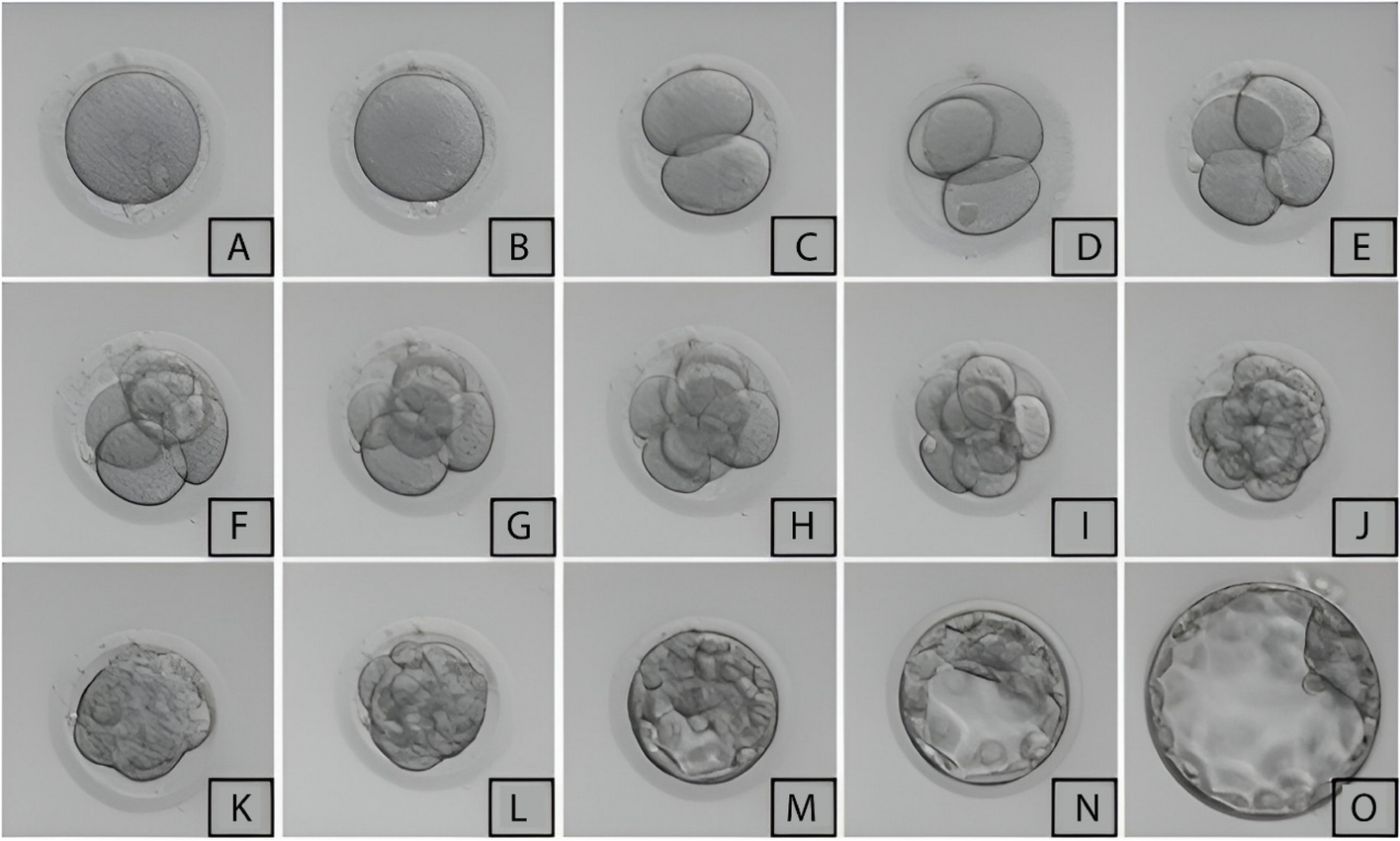
The oocytes destined for ICSI or for standard insemination were checked for fertilization 16 to 18 h after the procedure. The zygotes were then transferred into individual wells with 25 µl of pre-equilibrated single medium (SAGE 1-STEP, Origio, Trumbull, CT, USA or GLOBAL TOTAL, LifeGlobal, Paramus, NJ, USA) under mineral oil and cultured until day5 or 6 in a time-lapse system incubator (EmbryoScope, Vitrolife, Sweden), under standard incubation conditions (37 °C, 6% CO2 and 5% O2). Embryos were evaluated for cleavage stage (day 2/3) based on recording the number and symmetry of blastomeres, and the percentage of fragmentation. Blastocysts (day 5/6) were evaluated using a previously described scoring system [9]. Briefly, the blastocysts were classified as early (1–2 Gardner scale) or expanding (3–6 Gardner scale). For blastocysts graded as 3–6, the development of the inner cell mass and the trophectoderm were assessed. The inner cell mass was designated as: (A) tightly packed, many cells, (B) loosely grouped, several cells, or (C) very few cells. The trophectoderm was described as: (a) many cells forming a cohesive epithelium, (b) few cells forming a loose epithelium, or (c) very few, large cells. Only embryos of good morphology were biopsied (grade A or B). Biopsies were performed on day 5 or on the morning of day 6 depending on the grade of the expanded blastocyst (3–6, i.e., full blastocysts onward). Biopsies conducted on day 3 were performed at the 6–8 cell stage. Before biopsy, the cleavage stage embryos were pre-incubated for 10–15 min in Ca+ 2/Mg+ 2 free bicarbonate-buffered medium (Vitrolife, Sweden) to loosen cell-to-cell adhesions. Biopsies were undertaken using an inverted microscope (Diaphot 300, Nikon, Japan) equipped with a warming stage and micromanipulation system (Narashige, Japan). Laser technology (ZILOS-tk, Hamilton Thorne, Beverly, MA, USA) was used to dissect the zona pellucida, and one blastomere or 5 to 6 trophectoderm cells were pulled gently away from cleavage stage embryos/blastocysts. Before biopsy, the blastomeres were checked for the presence of nuclei. Each blastomere and trophectoderm cell was routinely washed prior to their transfer to the PCR tube, to ensure a pure sample. Moreover, a sample from the last drop of the washing medium was also collected in a different PCR tube and transferred for molecular analysis as a control, to detect contamination. After the procedure, the biopsied embryos were placed in separate numbered dishes with pre-equilibrated single medium to ensure easy identification of embryos post-diagnosis.
Molecular diagnosis
Establishing the haplotype was a necessary step in the preparation for PGT. Several informative microsatellite markers were selected for each patient in preparation for PGT. At least two informative polymorphic short tandem repeats were linked for each family on either side of the mutant allele. Primers suitable for multiplex PCR were carefully designed for each marker, and the diagnostic protocol was examined using DNA samples of appropriate family members who were carriers or non-carriers of the specific familial mutant allele. Each case was pre-validated in a model specifically designed for each family. Validation was achieved by employing genomic DNA samples for haplotyping and highly diluted DNA samples for pre-PGT validation, mimicking single-cell molecular testing.
Maternal and paternal DNA samples were always included in each case; therefore, these informative markers could differentiate the maternal and paternal contribution of alleles to all normal or abnormal embryos. The genetic constitution of each normal embryo is composed of one maternal and one paternal allele. An embryo with unequal parental contribution is easily detectable, while the origin of the extra allele is straightforwardly diagnosed by the pre-validated markers. Using multiple informative markers in all cases allows us to diagnose all embryos with uniparental disomy [10].
Data analysis
All data were analyzed using SPSS for Windows, version 24.0 (IBM Corp., Armonk, NY, USA). As the continuous variables were not normally distributed, we used descriptive statistics including the median values and non-parametric tests for the comparison of continuous variables among independent groups (Mann-Whitney U test). Chi-square test or Fisher’s exact test was used to compare rates and proportions, each when appropriate. The BRCA PGT cycles were compared to non-BRCA cycles (MD and PKD). Since some of the patients had more than one cycle, we also accounted for the total contribution of each patient and performed a generalized linear model analysis with a log link function, utilizing the natural logarithm (Ln) with the mathematical base e :When analyzing the oocyte yield, the model used the number of cycles (Ln cycles) as the offset variable. In the analysis of zygotes and biopsied embryos (representing the blastulation potential), the oocytes (Ln-oocytes) and zygotes (Ln-zygotes) were defined as the offset variables. All P values were two-tailed and considered significant at less than 0.05.





Comments (0)