
Remember me

In the United States, racialized minority groups, such as Black and Asian people, experience a greater severity of and disability from chronic pain.2,3,5,13,35,37 Interestingly, enhanced pain perception in minoritized groups appears to precede development of chronic pain. This enhanced sensitivity is possibly a result of the persistent stress caused by structural racism and systemic discrimination.8 Although racism against Black Americans is endemic and well recognized, the association of enhanced pain sensitivity in racially minoritized groups exists in other groups subject to racial discrimination. For example, the association of enhanced pain sensitivity in an ethnically minoritized group exists in China where people from the Uygur minority demonstrate enhanced pain sensitivity compared with the Han Chinese majority.63 Previous research indicates that Hispanic, Asian, and Black people have greater pain sensitivity, and above threshold painful stimuli is rated as more painful in these minoritized groups compared with White people. In addition, individuals from these minoritized racial or ethnic groups demonstrate lower tolerance, especially to stressful and thermal stimuli.12,31,36,38,39,43,50,51,53 Sex differences are well known in pain. Women tend to be more sensitive to pain, report higher pain intensity to fixed painful stimuli, and demonstrate lower tolerance compared with men.16–18,20,34,50 Minoritized group differences in pain sensitivity may limit patient-reported effectiveness of multidimensional pain treatment.23,33
Previous mixed reports of minoritized group differences in pain-related psychological traits (eg, depression, anxiety, pain catastrophizing) may indicate greater depression, anxiety, and pain catastrophizing in racialized minorities compared with White people.4,10,36,60 Differences in somatization across racialized groups were also reported, indicating that Black people and women with temporomandibular disorders had higher level of somatization compared with White people and men.19
The pain sensitivity questionnaire (PSQ) has been used to measure self-rated pain sensitivity, predominantly in populations predominantly composed of European sociocultural background.54–56 Studies have shown that the PSQ detects minoritized group differences in between Black and White people in pain sensitivity and clinical pain for both healthy participants and patients with chronic pain.5,40 The original validation study found no sex difference in PSQ, while finding differences in experimental pain sensitivity between men and women.54 Currently, limited information regarding validity of the PSQ is available in Asian and Black people.
Overall enhanced pain sensitivity is often present in minoritized groups that experience discrimination. This led us to the hypothesis that no matter the identity of the group, anxiety experienced by racialized minority groups and women would lead to enhanced pain sensitivity. Based on prior research, we predicted that enhanced pain sensitivity in minoritized groups would be mediated by greater anxiety, which is often the result of the experience of stress and discrimination.9,40,48 The primary predictions of this secondary analysis study were as follows: (1) people from racialized minority groups would be more sensitive to painful stimuli and rate painful stimuli greater than White people, and this enhanced sensitivity would be mediated by anxiety or pain catastrophizing11,12,38,50; (2) women would be more sensitive to painful stimuli and rate painful stimuli greater than men, and this enhanced sensitivity would be mediated by anxiety or pain catastrophizing50; (3) there would be a positive correlation between PSQ scores and pain intensity ratings to suprathreshold painful mechanical stimuli54; (4) there would be an effect of racialized minority group on self-report pain sensitivity in terms of the PSQ score and somatization in terms of the Pennebaker Inventory of Limbic Languidness (PILL) score.5 Finally, considering the Eurocentric sociocultural development of the pain sensitivity questionnaire, we predicted that racially minoritized individuals’ lack of experience with some of the items on the PSQ would lead to a different estimation of PSQ item rating compared with those items that had been experienced.54
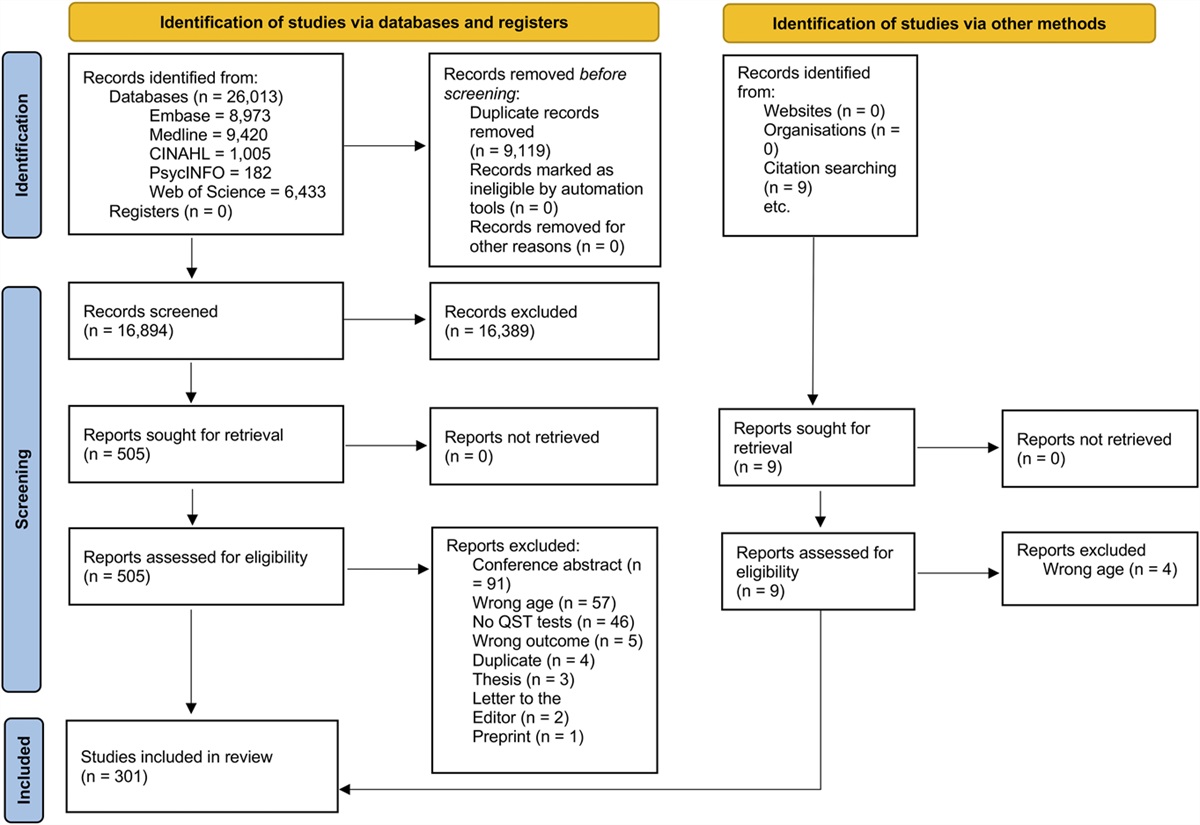
2. Methods 2.1. OverviewWe report results of a secondary analysis of data from 3 studies conducted at the University of Maryland Baltimore (UMB) from October 2011 to December 2015. In accordance with the secondary analysis, we did not conduct an a priori sample size calculation. Study participants were recruited by advertisement in and around the UMB community. All participants provided written informed consent, and procedures were approved by the UMB Institutional Review Board for the Protection of Human Subjects. Results of these studies have been previously reported in different contexts.44–46
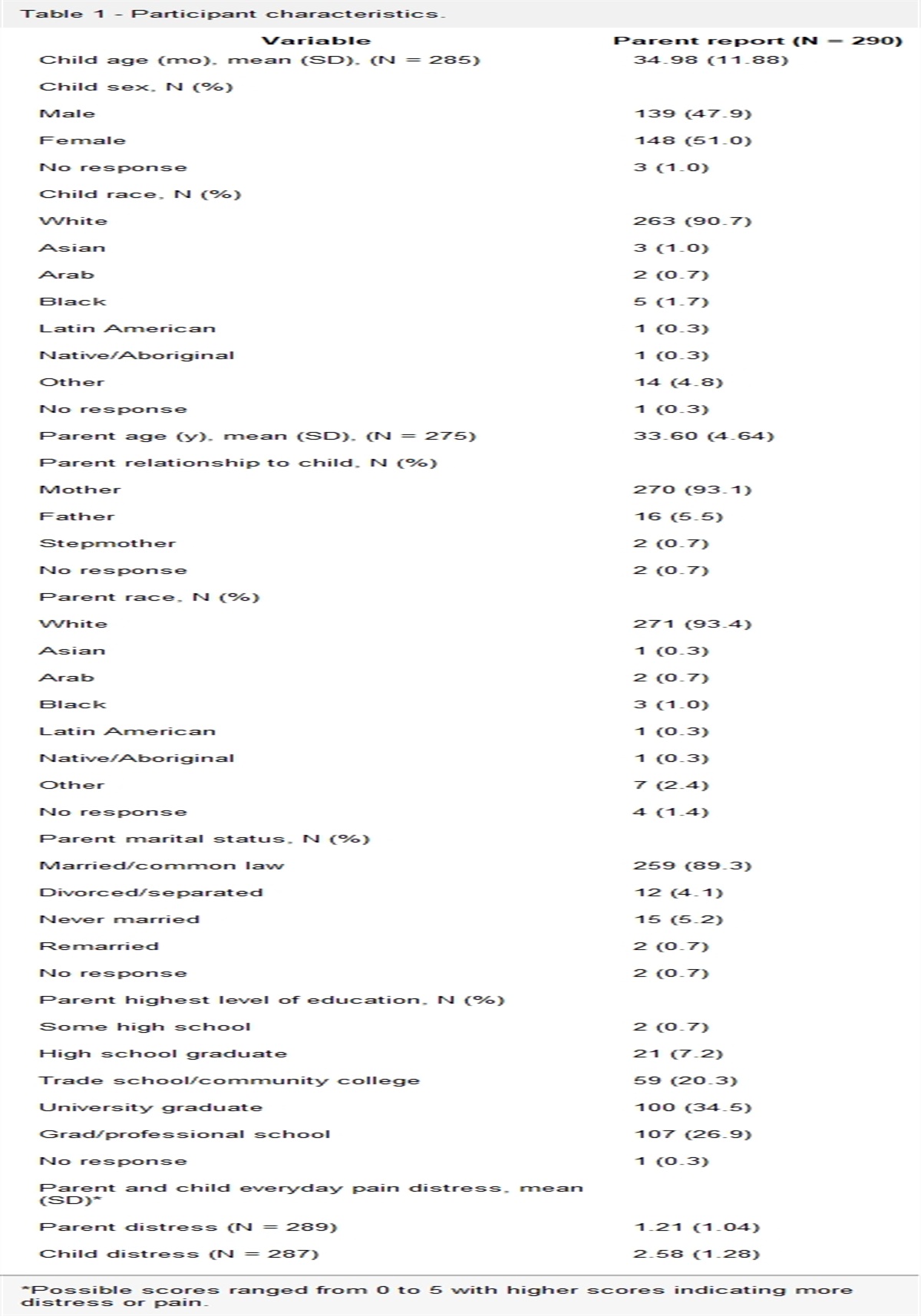
2.2. ParticipantsIn study 1, we screened 31 potential participants and include data from 26 participants. We excluded 3 participants because they did not fulfill eligibility criteria (Supplemental Table 1, https://links.lww.com/PR9/A218). We used self-reported race according to US Census guidelines specifically “Asian or Asian American,” “Black or African American,” “White, Caucasian, or European,” “Native American,” “Hawaiian Native or Pacific Islander” and “Other,” which was a write-in. In this report, we use the terms Asian, Black, or White people to refer to these racialized groups. No persons self-reported “Native American” or “Hawaiian Native or Pacific Islander.” We excluded a further 2 participants who self-reported mixed race. Of the 26 participants (17 women) in study 1, 6 self-identified as Asian, 2 as Black, and 18 as White with a median age of 30 years (range: 22–61 years). In study 2, we screened 50 potential participants and include data from 42 participants in the present report. We excluded 8 participants because they did not fulfill eligibility criteria (Supplemental Table 2, https://links.lww.com/PR9/A218). The 42 participants (18 women) in study 2 included 9 Asian, 5 Black, and 28 White people with a median age of 25.5 years (range: 20–38 years). In study 3, we screened 91 potential participants and include data from 66 participants in the present report. We excluded 24 participants because they did not fulfill eligibility criteria (Supplemental Table 3 and Supplemental Table 4, https://links.lww.com/PR9/A218). We excluded a further single participant who self-reported mixed race. Data from participants who self-identified as “mixed race” is reported in supplemental material (Supplemental Table 5, https://links.lww.com/PR9/A218). The 66 participants (38 women) in study 3 included 19 Asian, 18 Black, and 29 White people with a median age of 25 years (range: 18–43 years). Data were included from 134 participants (73 women), composed of 34 (18 women) Asian, 25 (13 women) Black, and 75 (41 women) White people with a median age of 26 years (range: 18–61 years) (Table 1).
Table 1 - Demographics by racialized group. Measure Asian people (Percent/SD) Black people (Percent/SD) White people (Percent/SD) χ2 or ANOVA Female 18 (53%) 14 (56%) 41 (55%) Χ2 = 0.057*These demographic variables were not collected for 7 Asian, 3 Black, and 23 White people.
†These demographic variables were not collected for 6 Asian, 2 Black, and 18 White people.
In studies 2 and 3, before any thermal assessments, we evaluated suprathreshold mechanical pain ratings by having participants rate pain intensity to 4 different weighted mechanical probes (64, 128, 256, and 512 mN force with a flat circular tip of 0.2-mm diameter).27,29,30,46 Stimuli were applied 1 cm outside the area of subsequent thermode placement on the lower leg. Each probe force was applied in a random order, 3 times each, moving clockwise around the area of thermode placement. Each probe was placed for 1 second, then the participant provided a rating of pain intensity on a 0 to 100 scale, with “0” indicating no pain at all and “100” indicating the most intense pain imaginable. A 15-second interval separated each trial. Participants rated their pain intensity on a numerical rating scale (NRS) with verbal anchors and numbers ranging from 0 to 100 by 10s.28
2.3.2. Warmth detection thresholdWarmth detection threshold was measured using a Pathway (MEDOC Inc; Ramat Yishai, Israel) thermal sensory testing device with a thermode of Peltier elements (3 × 3-cm2 thermoconducting surface; maximum temperature of 50°C). The thermode was placed on the participant's left leg over the thickest part of the tibialis anterior muscle. The thermode was held at a 32°C, and then, the temperature was increased at 0.5°C/second. Participants were instructed to click a computer mouse when they first felt a change in temperature. This sequence was repeated 4 times. The average of these 4 measurements was taken as the WDT.
2.3.3. Heat pain thresholdFollowing WDT determination, heat pain threshold (HPT) was measured in a similar manner. The baseline temperature was 32°C in studies 1 and 2, whereas baseline temperature was 30°C in study 3. In all studies, the temperature was increased at 0.5°C/second. Participants were instructed to click the computer mouse when the warmth becomes painful. This sequence was repeated 4 times. The mean of the final 3 of 4 measurements taken as the HPT.
2.4. Self-report questionnaires 2.4.1. Pain sensitivity questionnaireWe used the PSQ to assess each participant's self-report pain sensitivity by rating how painful specific experiences would be for the participant.54 The 17-item survey can be separated into 2 subscales—minor and moderate—reflecting the general level of expected pain for each item, along with 3 normally nonpainful items. We used the sum of the score for minor and moderate items and discarded the 3 normally nonpainful items. Test–retest reliability for the PSQ has been reported as adequate with intraclass correlations (ICCs) of 0.83 over intervals of 1 to 3 weeks. Internal consistency for the PSQ is high, with Cronbach alphas > 0.90. Cronbach alpha of the PSQ data analyzed in this study was 0.93 (95% CI, 0.91–0.95). Preliminary studies indicated that although many people had experienced the items described, many situations may be influenced by racial, ethnic, or cultural associations. Therefore, we included the following phrase after each question: “Also, indicate if this has ever happened to you.”
2.4.2. Pain catastrophizing scaleIn studies 2 and 3 and in 6 participants in study 1, we used the pain catastrophizing scale (PCS), which comprises 13 self-reported items to describe the thoughts and feelings of an individual when experiencing pain.58 Previously reported test–retest reliability for the PCS has indicated a high degree of stability across 6 weeks with an r = 0.75. Cronbach alpha of the PCS data analyzed in this study was 0.91 (95% CI, 0.88–0.93).
2.4.3. State-trait anxiety inventoryIn studies 2 and 3, we used state-trait anxiety inventory (STAI), which comprises 40 self-reported items.57 Items 1 to 20 evaluate state anxiety (STAI-S), whereas items 21 to 40 assess trait anxiety (STAI-T). STAI state scale uses a 4-point scale for each item, ranging from “1” (not at all) to “4” (very much so), whereas items in the STAI trait are rated from “1” (almost never) to “4” (almost always). The STAI state and trait subscales were scored as sum scores. Test–retest reliability for the trait anxiety scale has been reported as adequate, ranging from 0.73 to 0.86 over intervals of 20 to 104 days. Cronbach alpha, indicating internal consistency, of the STAI state data analyzed in this study was 0.92 (95% CI, 0.89–0.94), whereas that for the STAI trait was 0.92 (95% CI, 0.90–0.94).
2.4.4. Pennebaker Inventory of Limbic LanguidnessIn studies 2 and 3 and in 6 participants in study 1, we used the PILL as an indicator of somatic awareness.52 It comprises 54 self-reported items, which assess the self-reported frequency of common physical symptoms and sensations, such as racing heart, headaches, and coughing. It uses a 5-point scale for each item, from “0” (have never or almost never experienced the symptom) to “4” (more than once every week). The PILL has adequate test–retest reliability (0.70 over 2 months). Cronbach alpha of the PILL data analyzed in this study was 0.92 (95% CI 0.90–0.94).
2.5. Statistical analysisEffects of sex and racialized minority group on questionnaire, QST, and demographic outcomes were evaluated using simple general linear models in R version 4.2.2. Assessment of statistical significance was performed with the “anova” function, whereas post hoc testing was performed using the general linear hypothesis test command in the multcomp package in R with Holm–Sidak correction. Effect size measures from contrasts are reported as Cohen d. Cronbach alphas were calculated on raw item-level data using R version 4.2.2's “alpha” function from the psych package. Summary of total data per measure is presented in Supplemental Table 4, https://links.lww.com/PR9/A218.
For suprathreshold mechanical pain (STMP) ratings, we used linear mixed models taking into account force as a repeated-measures factor to evaluate effects of racialized minority group and sex on pain intensity ratings.24 Assessment of statistical significance was performed with the anova command, whereas post hoc testing was performed using the general linear hypothesis test command in the multcomp package in R. For post hoc significance calculations, we used the false discovery rate (FDR) correction for multiple comparisons. We used Pearson correlation to calculate correlation coefficients from normally distributed data. Significance of P values are reported in terms of unadjusted significance levels at P < 0.05 and after FDR or Holm–Sidak correction depending on the number of hypothesis tests with post hoc tests requiring 6 or more comparisons corrected with FDR.6,32
To test the mediation effects of anxiety and pain catastrophizing on differences in pain sensitivity, we used the structural equation model module “sem” in STATA version 18.
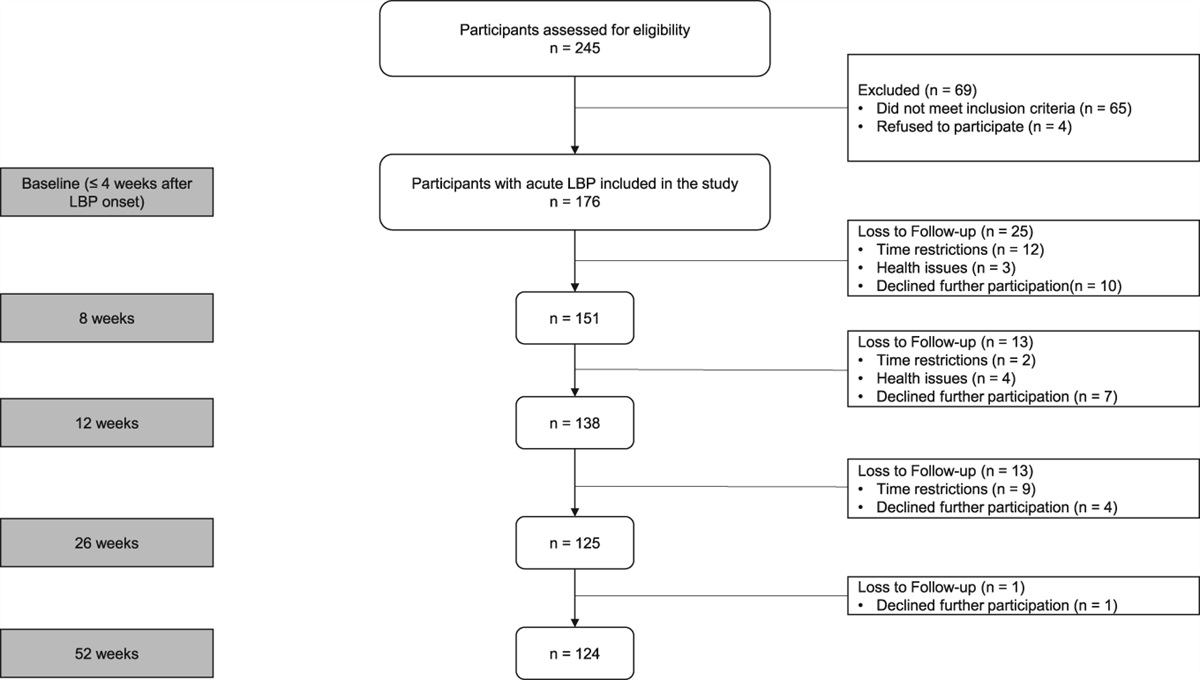
3. Results 3.1. Demographic factors potentially associated with minoritized racial differences in pain sensitivity were similar across racialized groups and biological sexGeneral linear models (GLMs) evaluating proportion of women in each group, age, marital status, proportion of students in each group, and proportion smoking tobacco found that racialized minority group was not associated with these factors (Table 1). Although education was greater and status of drinking alcohol was less frequent in Asian people, there was no difference in these factors between Black and White people (Table 1). GLMs evaluating age, marital status, education level, proportion of students in each group, proportion drinking alcohol, or proportion smoking tobacco found that female sex was not associated with these factors (Table 2).
Table 2 - Demographics by biological sex. Measure Female people (Percent/SD) Male people (Percent/SD) χ2 or ANOVA Age (median/range) 26 (18–56) 26 (20–61) Χ2 = 0.72*These demographic variables were not collected for 19 female and 13 (marital status or education) or 14 (occupation) male people.
†These demographic variables were not collected for 17 female and 9 (smoking) or 10 (drinking) male people.
GLMs evaluating the effect of racialized group and biological sex on warmth and heat pain sensitivity found significant effects of racialized group (F2,128 = 7.63; P = 0.00074) and sex (F1,128 = 4.90; P = 0.029) on heat pain sensitivity and significant effects of sex (F1,128 = 10.84; P = 0.0013) on warmth sensitivity (Fig. 1). There were no significant interaction effects (HPT: F2,128 = 0.29; P = 0.75; WDT: F2,128 = 0.31; P = 0.73). Post hoc comparisons found that Asian (t-stat = 3.70; P = 0.0094; Cohen d = 0.73; mean difference (MD) = 2.3°C; 95% confidence interval (CI) = 1.1–3.5°C) and Black people (t-stat = 2.34; P = 0.042; d = 0.55; MD = 1.6°C; 95% CI = 0.3–2.9°C) were more sensitive to heat pain, having lower HPTs than White people (Fig. 1A). Post hoc comparisons of the sex main effect found that women were more sensitive to heat pain (t-stat = 2.23; P = 0.028; d = 0.38; MD = 1.2°C; 95% CI = 0.2–2.2°C) and warmth (t-stat = 3.31; P = 0.0012; d = 0.57; MD = 1.7°C; 95% CI = 0.7–2.7°C) compared with men (Figs. 1B and D).There was no significant effect of racialized group on warmth sensitivity (F2,128 = 0.73; P = 0.49) (Fig. 1C). There were no significant mediation effects of either PCS or state or trait anxiety on significant differences in heat pain sensitivity among racialized groups or between sexes (Supplemental Table 6, https://links.lww.com/PR9/A218). There were no significant effects of sex or racialized group on STMP, but effects of probe force were significant (Supplemental Results and Supplemental Figure 1, https://links.lww.com/PR9/A218).
 Figure 1.:
Figure 1.: (A) Heat pain sensitivity, assessed by heat pain thresholds assorted by racialized group. (B) Heat pain sensitivity, assessed by heat pain thresholds assorted by biological sex. (C) Warmth sensitivity, assessed by warmth detection thresholds assorted by racialized group. (D) Warmth sensitivity, assessed by warmth detection thresholds assorted by sex. *P < 0.05; **P < 0.01; ***P < 0.001.
3.3. Self-report pain sensitivity is greater in Asian and Black people compared with white peopleGLMs evaluating the effect of racialized group and sex on self-report pain sensitivity, pain catastrophizing, and a measure of somatization found significant effects of racialized group on self-report pain sensitivity (F2,127 = 15.45; P = 9.84 × 10−7) but not on pain catastrophizing (F2,107 = 1.023; P = 0.36) or somatization (F2,107 = 2.22; P = 0.11) (Fig. 2A). We found significant effects of sex on somatization (F1,107 = 4.14; P = 0.044) and self-report pain sensitivity (F1,127 = 9.50; P = 0.0025) but not on pain catastrophizing (F1,107 = 0.044; P = 0.83). There were no significant interaction effects (PCS: F2,107 = 2.35; P = 0.10; PILL: F2,107 = 0.48; P = 0.62; PSQ: F2,127 = 1.81; P = 0.17). There were no significant mediation effects of PCS or state or trait anxiety on significant differences in self-report pain sensitivity among racialized groups or between sexes (Supplemental Table 6, https://links.lww.com/PR9/A218).
 Figure 2.:
Figure 2.: (A) Somatization, measured by Pennebaker Inventory of Limbic Languidness (PILL) sum score, assorted by racialized group. (B) Somatization, measured by PILL sum score assorted by sex. (C) Self-report pain sensitivity, measured by pain sensitivity questionnaire (PSQ) score, assorted by racialized group. (D) Self-report pain sensitivity, measured by PSQ score assorted by sex. *P < 0.05; **P < 0.01; ***P < 0.001.
Post hoc comparisons of the sex association found that women report greater somatization compared with men (t-stat = 2.05; P = 0.043; d = 0.38; MD = 6.5; 95%CI = 0.3–12.7) (Fig. 2B). Post hoc comparisons found Asian (t-stat = 4.53; P = 4.1 × 10−5; d = 1.03; MD = 1.14; 95% CI = 0.64–1.64) and Black people (t-stat = 4.32; P = 6.1 × 10−5; d = 0.99; MD = 1.21; 95% CI = 0.66–1.76) reported greater self-report pain sensitivity compared with White people (Fig. 2C). Further post hoc comparisons found that men reported greater self-report pain sensitivity compared with women (t-stat = 3.06; P = 0.0027; d = 0.47; MD = 0.65; 95% CI = 0.24–1.06) (Fig. 2D). Finally, somatization, pain catastrophizing, state/trait anxiety, and self-reported pain sensitivity were significantly positively associated in our sample (Supplemental Figure 2, https://links.lww.com/PR9/A218).
3.4. Pain sensitivity questionnaire items have not been experienced equally across racialized groupsTo evaluate the validity of the PSQ in a racially diverse population, we used an ANOVA for the effects of racialized group and sex on the percent of questions participants positively endorsed “indicate if this has ever happened to you” (PSQ%Y). There was a significant association of racialized group on PSQ%Y (F2,124 = 19.87; P = 3.28 × 10−8), but the effect of sex (F1,124 = 0.30; P = 0.59) and interaction of racialized group and sex (F2,124 = 1.25; P = 0.29) were not significant. Post hoc comparisons found that Asian (t-stat = 3.35; P = 0.0022; d = 0.87; MD = 6.4%; 95% CI = 2.7–10.1%) and Black people (t-stat = 6.05; P = 4.63 × 10−8; d = 1.64; MD = 12.6%; 95% CI = 8.5–16.7%) reported experiencing PSQ items at lower rates than White people (Fig. 3A). Although the sample size was sufficient to assume a Gaussian distribution of residuals, we used a Kruskal–Wallis test to verify that racialized group was significant (Χ2 = 39.0; P = 3.4 × 10−9), whereas sex was not (Χ2 = 0.00052; P = 0.98) (Fig. 3B). Black people reported a significantly lower rate of experiencing PSQ items compared with Asian people (t-stat = 2.59; P = 0.11; d = 0.52; MD = 6.2%; 95% CI = 1.5–10.9%). Further interrogating the validity of the PSQ, we found a negative correlation of PSQ score vs PSQ%Y (Spearman R = −0.30; P = 0.00045) (Fig. 3C).
 Figure 3.:
Figure 3.: (A) Percent of pain sensitivity questionnaire (PSQ) items experienced assorted by racialized group. (B) Percent of PSQ items experienced assorted by sex. (C) Correlation of percent of PSQ items experienced vs PSQ score. In (C), gray area denotes 95% confidence interval of linear fit. *P < 0.05; **P < 0.01; ***P < 0.001.
We used a LMM to analyze the association of racialized group with PSQ rating for each individual item of the PSQ including only those 14 items in the total score. Importantly, the overall association of racialized group on PSQ rating remained significant (F2,482 = 6.05; P = 0.0025) and the interaction of racialized group and PSQ question number was significant (F26,1651 = 2.50; P = 4.42 × 10−5). After Bonferroni correction for the number of statistical hypothesis tests (n = 42; P < 0.0012), one item (Q3) showed significantly higher scores for Asian and Black people compared with White people, 2 items (Q7 and Q8) showed significantly higher scores for Black people compared with White people, and 4 items (Q4, Q10, Q11, and Q12) showed significantly higher scores for Asian people compared with White people (Table 3). Fewer than 70% of Black participants reported having experienced 3 of the PSQ items (Q6, Q10, and Q11) (Table 3). When a participant reported having not experienced a PSQ item, the participant would rate the item as less painful compared with when they had experienced the item (Z = 1.97; P = 0.049).
Table 3 - Racial differences in PSQ items from the moderate and minor subscales. Asians > Whites AAs > Whites Percent yes (%) PSQ item t-stat P t-stat P Asians AAs Whites 1. Bump shin on table 2.13 0.084 3.24 0.0037 87.5 88 95.9 2. Burn your tongue 3.41 0.0020 3.31 0.0029 100 92 100 3. Muscles slightly sore 4.17 0.00015 4.34 <0.0001 100 96 100 4. Trap finger in drawer 4.53 <0.0001 3.10 0.0057 93.7 84 97.3 6. Mild sunburn 3.49 0.0015 1.84 0.156 75 32 100 7. Graze knee 3.40 0.0021 3.86 0.00037 87.5 92 97.3 8. Bite your tongue 3.08 0.0063 3.56 0.0011 100 100 98.6 10. Lemon juice in cut 5.53 <0.0001 1.53 0.276 84.4 56 90.4 11. Prick finger on thorn 3.98 <0.001 2.58 0.027 84.4 60 91.8 12. Bare hands in snow 4.60 <0.0001 3.40 0.002 84.4 88 100 14. Handshake with strong grip 0.95 0.61 2.46 0.037 93.7 92 97.3 15. Pick up hot pot 1.17 0.47 2.45 0.039 96.9 92 98.6 16. Heavy boot on bare foot 1.89 0.14 3.42 0.0019 91.6 84 86.3 17. Bump “funny bone” 1.76 0.18 2.60 0.026 100 92 100Items in bold are statistically significant after Bonferroni correction for 28 hypothesis tests.
PSQ, pain sensitivity questionnaire.
Pain sensitivity questionnaire scores positively correlated with suprathreshold mechanical pain ratings for the 64 mN, 128 mN, 256 mN, and 512 mN probes with R = 0.30–0.41; P < 0.0024 (Supplemental Figure 3, https://links.lww.com/PR9/A218). However, neither warmth (R = 0.071; t = 0.803; P = 0.423) nor heat pain thresholds (R = −0.135; t = −1.55; P = 0.123) significantly correlated with self-report pain sensitivity.
The GLM showed that neither sex (state: F1,104 = 0.0034; P = 0.95; trait: F1,107 = 0.04; P = 0.84) nor racialized group (state: F2,104 = 0.099; P = 0.91; trait: F2,107 = 0.64; P = 0.53) or their interaction (state: F2,104 = 1.14; P = 0.33; trait: F2,107 = 0.98; P = 0.38) had significant effects on state or trait anxiety.
4. DiscussionThis study examined biological sex and racialized group differences in pain sensitivity using both QST and PSQ, and associations among somatization and psychological traits, including state and trait anxiety and pain catastrophizing with pain sensitivity. We found that men reported greater pain in response to common painful experiences compared with women, whereas women reported greater warmth and heat pain sensitivity but not suprathreshold ratings to painful mechanical stimuli compared with men. We found Asian and Black people reported greater pain responses to common painful experiences and were more sensitive to heat pain compared with White people, but no racialized group difference was found for warmth sensitivity or suprathreshold mechanical pain. The overall pattern of sex and racialized minority group associations with enhanced pain sensitivity support our overall hypothesis that no matter the identity of the group, the stress of systemic discrimination and adverse life experiences of structural minoritization leads to enhanced pain sensitivity. However, in contrast to our predictions and previous findings, we found no mediating effect of anxiety or pain catastrophizing on this enhanced pain sensitivity.20,47 It should be stressed that we found enhanced pain sensitivity in racially minoritized individuals despite the presence of similar or greater protective demographic factors such as education and less alcohol and tobacco use.
Sex differences in pain sensitivity are well known, and this study adds to the literature by providing specific information on diverse modalities of pain sensitivity among young healthy participants.18 Each modality of pain is associated with different contributions of peripheral nerve fibers signaling of pain conditions and subsequent perception.1,61 Similarly, men and women may respond differently to heat pain stimuli, and the modulatory function of other psychological traits, such as anxiety, have been shown to play a role sex differences.14,22,59 Greater female sensitivity to warmth and painful heat may imply enhanced peripheral nervous system activity in response thermal stimuli in women compared with men.
Previously, a systematic review and meta-analysis revealed the differences in racialized group differences by the type of experimental pain modality; racialized minorities had higher pain sensitivity mainly on suprathreshold pain responses but not in thresholds on various modalities of pain stimuli.38 This study reinforces the notion that minoritized racial groups experience greater pain in response to noxious thermal stimuli compared with White people. We found significant increases in thermal sensitivity as measured by lower thresholds in Asian and Black people compared with White people. Although lowered heat pain thresholds (ie, greater heat pain sensitivity) in minority groups compared with majority White people has been reported previously, other studies have found no difference between White people and others in this measure.12,15,62,64
Higher psychological traits related to pain among women and racialized minorities have been reported previously2,7,26,37; therefore, including these factors in understanding pain disparities is necessary. In contrast to previous studies, we found no racial
Comments (0)