The current study investigated the differences in clinical, radiological, and histological features of nasal polyps between HIV-positive and HIV-negative patients and found that there was no statistical difference between these patients.
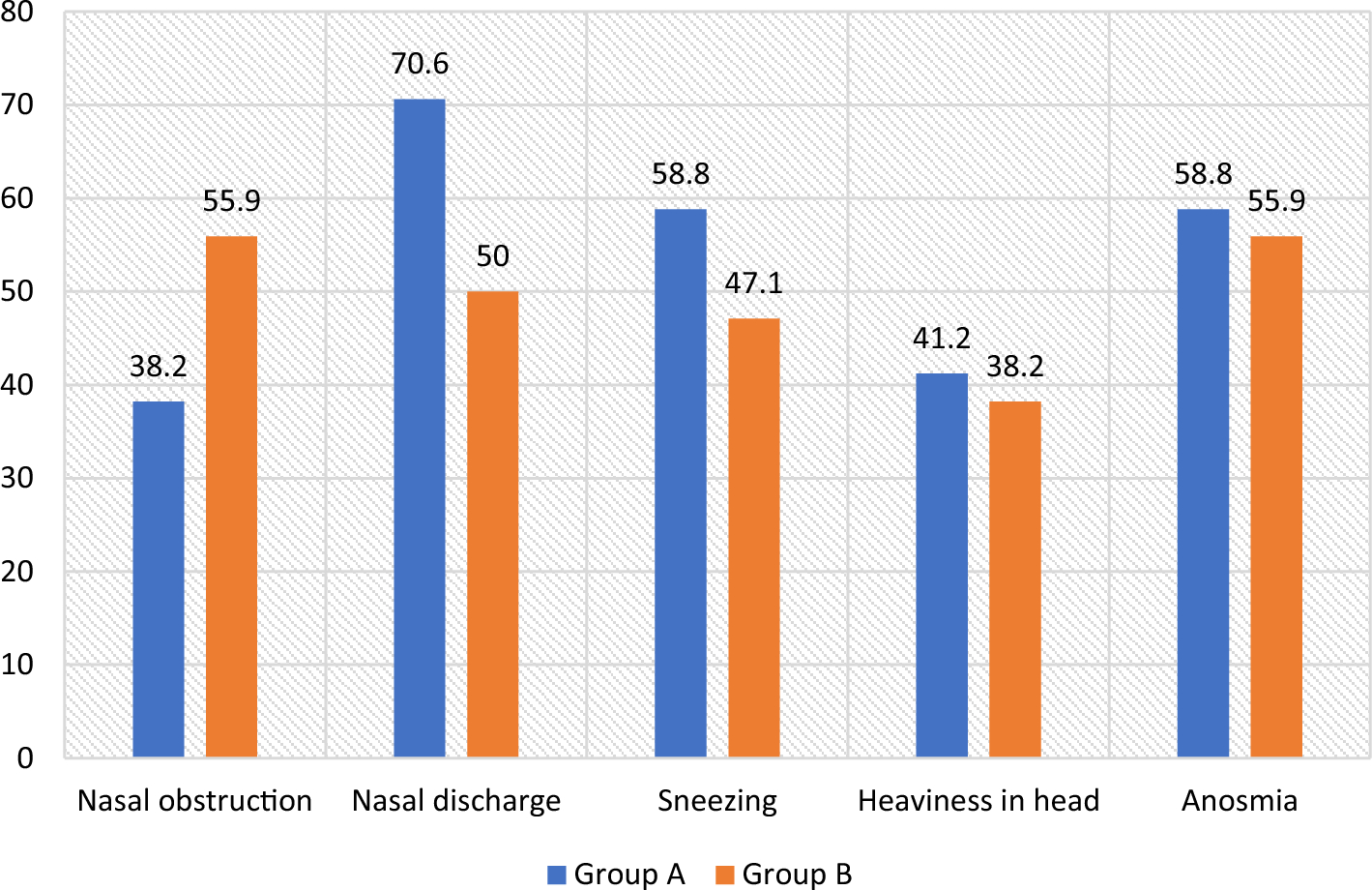
Interestingly, the prevalence of nasal discharge, nasal congestion, anosmia, facial pressure, postnasal drip, and aspirin sensitivity were comparable between both HIV-positive and HIV-negative patients. There was no significant difference in the prevalence of these clinical symptoms between the two groups. There are no studies that point to marked differences between the groups regarding these symptoms. That is because most studies on nasal polyps have been conducted in low HIV prevalence regions and thus, have not considered it in the process [1, 11, 13].
Despite this, this study found asthma was more prevalent in HIV-positive patients than HIV-negative patients, although the difference was not statistically significant. This finding aligns with literature, studies have found asthma to be highly prevalent in people living with HIV [15, 17, 27] Respiratory diseases are common in people with HIV resulting from severe immune dysregulation from the infection. It is still unclear how asthma and HIV relate however, the IgE and cytokine network are implicated [17].
Moreover, no patient presented with either cough or ageusia. These findings suggest that the presence of nasal polyps may not be significantly affected by HIV status.
Additionally, the Lund McKay Score was assessed in both HIV-positive and HIV-negative patients, and it was found that HIV-negative patients had a slightly higher score on average compared to HIV-positive patients. Although this difference was not statistically significant, it indicates that HIV status may not affect the severity of nasal polyps. Again, no studies exist that indicate differences in scores.
Genetic factors associated with nasal polyps are important to consider, especially in patients living with HIV. In this study, none of the patients had ciliary dyskinesia, cystic fibrosis or Kartegener syndrome, which are known genetic factors associated with nasal polyps. However, atopy was reported in 20% of the sample. Although there was no statistically significant difference in atopy between HIV-negative and HIV-positive patients, it is still an important factor to consider in patients with nasal polyps. Atopy has been previously associated with the development of nasal polyps, and it is believed to be a risk factor for the recurrence of nasal polyps after surgical treatment [25]. It is apparently common in South Africa due to environmental factors [20]. Therefore, its prevalence may be indicative of what is happening at the population level in the country. However, a study on rhinosinusitis and atopy among people living with HIV reported atopy being present in 18% of patients similar to what this study found [9]. However, the study in question was a case series and such studies generally rank low on the hierarchy of evidence due to their high susceptibility to bias. As such, it may be prudent to suggest that the result was only a fluke, especially in the absence of any more genetic evidence about HIV infection and atopy.
Furthermore, sneezing and itchy nose were reported in a small percentage of the total patients, with only HIV-negative patients reporting sneezing and no HIV-positive patients reporting itchy nose. These clinical symptoms could be associated with allergic rhinitis, which is a common comorbidity of nasal polyps. In patients living with HIV, the immune system is compromised, and this could affect their response to allergens and the development of allergic rhinitis [2, 3].
Additionally, results of this study provide insight into the histological factors associated with nasal polyps in HIV-positive and HIV-negative patients. The presence of respiratory mucosa was more common in patients living with HIV. This finding can be corroborated by a study by Sellers and colleagues [30] which found that the respiratory mucosa of HIV-infected patients showed decreased pro-inflammatory cytokine levels.
Basement membrane thickening was higher in the HIV-positive group, with a marginal difference noted. Particular cases of basement membrane disease in people living with HIV due to elevated levels of antibodies have been noted [22, 33]. This could explain the higher prevalence. Similarly, fibrosis and pseudostratified ciliated columnar were more prevalent in patients living with HIV. That is because immune activation and persistent inflammation are likely to contribute to collagen deposition and lymphoid tissue fibrosis in HIV-infected people [7].
Bone overall degree of inflammation was observed only in patients living with HIV. This result is in line with other research that suggested a link between HIV infection and bone inflammation. It has been hypothesized that HIV infection can result in chronic inflammation that causes bone loss, which may help persons living with HIV develop osteoporosis and increase their risk of fracture [16, 24]. It has been suggested that HIV-associated chronic inflammation may cause an increase in bone resorption and a decrease in bone formation, albeit the precise mechanism underlying this link is not entirely known. It is important to bear in mind that bone inflammation is a complex process, with HIV infection being only one of the numerous variables that might play a role in the development of this condition [4, 16, 24].






Comments (0)