
Remember me


What is known about the topic?
Aged care is a dynamic sector experiencing rapid change. Implementation of innovations is complex and the context is important. Lessons from implementation in health care cannot necessarily be applied to aged care.What does this paper add?
A comprehensive review that identifies five key categories of factors that influence implementation in the aged care context, especially resourcing. Identifies rapid, recent growth in the field of aged care implementation research. Identifies the need for greater attention to community-based aged care services, use of implementation science theory, and inclusion of consumers in aged care implementation research. INTRODUCTIONAged care is a dynamic sector experiencing rapid and significant change due to various socio-demographic and policy drivers.1 In Australia, this includes major policy reforms2; a greater proportion of services provided in the community as opposed to residential facilities3; and an increased proportion of private, for-profit providers in the aged care market.4
Implementing something new—an innovation—is complex, and context matters. An implementation that works in one context may not necessarily work in another. Identifying the factors that influence the implementation of innovation for a particular context helps to ensure that implementation strategies are contextually appropriate so that implementation is successful. In this paper, we broadly define an innovation as something new in a given service setting—it could be a technological device, equipment, a model of care, an evidence-based guideline, infrastructure, or anything that differs from the status quo.
Much research has explored implementation in health care, but considerably less so in aged care. While there are many parallels between the aged care and health care sectors, there are some key differences, particularly in the scope and frequency of care and structural aspects of the systems, such as funding and regulation. The scope of aged care services is broader than health care, incorporating support for activities of daily living, meals and nutrition, social and emotional support, and the physical environment. Aged care also differs in terms of being long-term, high-frequency (daily) care relationships, whereas health care tends to be more episodic, with less frequent engagement between service providers and recipients. The goals of care also differ, particularly between acute care, which has curative objectives, and aged care, which is more holistic and focused on quality of life. Findings from health care implementation research cannot necessarily be applied to contemporary aged care. While aged care implementation research is less well-progressed than that of health care, there appears to be a growing body of literature. Several reviews have examined factors that influence implementation in aged care settings. Masso and McCarthy5 reviewed factors that support the implementation of evidence-based practice in residential aged care. Focusing on clinical care, they identified the importance of the evidence itself, the implementation process, available resources, and the impact of the context. Their subsequent review6 examined the mechanisms that influence implementation of evidence-based practice in residential aged care facilities, identifying the importance of the human dimension of change. More recently, McArthur et al.7 reviewed studies of long-term care staff perspectives on barriers and facilitators to implementing evidence-based practice guidelines. They highlighted leadership, strategic use of resources, and organizational support for change. Our review adds to this previous work in several ways: we include community-based aged care services as well as residential care; we adopt a broad definition of aged care that extends beyond clinical care; we adopt a broad definition of innovation that includes, but is not limited to, guidelines, and we adopt a broad frame of analysis in considering contextual factors as well as those relating to individuals, innovations, and mechanisms. Furthermore, our review is informed and supported by an advisory group comprising aged care consumers, staff, and researchers.
Our review aimed to identify a broad range of factors from studies of various designs, and explored the nature and extent of the literature. It did not, however, critique the quality of included papers. We determined that a scoping review would be best suited to our objectives.8
OBJECTIVESThe objectives of this scoping review were to:
identify the factors that influence the implementation of innovations in aged care; and explore the scope and limitations of the aged care implementation research literature. REVIEW QUESTIONS 1. What factors influence the implementation of innovations in aged care? 2. What does the aged care implementation research literature look like in terms of the characteristics and focus of research, and what are the patterns and shortcomings in this literature? INCLUSION CRITERIA ParticipantsAs the study context was aged care, the participants in the included studies were people working in or receiving care from an aged care organization. External service providers who deliver services within the aged care setting (e.g., general practitioners) as well as people who support the implementation of innovations (e.g., researchers) were also included.
ConceptTo be included, studies must have identified factors that influenced implementation based on the real-world implementation of an innovation. Factors influencing implementation had to be “measured” (or identified qualitatively) and reported in the findings for the paper to be included, rather than simply surmising in the discussion. Intervention studies whose primary aim was to test the effectiveness of an innovation that also examined implementation, could be included (e.g., a quasi-experimental study5 of a “reablement” program that examined clinical outcomes and identified organizational barriers to the program's feasibility). Studies that were a “pre-implementation” assessment of potential barriers/enablers were not included. Similarly, studies that were an assessment of hypothetical perceptions of an innovation were also excluded.
The scope of innovations was broad—including but not limited to evidence-based practice—defined as new products, services, programs, models, and technology. Papers in which the practice implemented was not new were excluded (e.g., a study examining barriers to routine oral care that did not involve a change in practice).
ContextTo be included, studies had to be conducted in aged care settings or organizations. We define “aged care” as formalized care provided primarily to older people (usually aged 65+ but could be younger in particular populations), including residential facilities, community settings, “seniors’ centers,” or “day centers.” Studies were excluded if they were about informal or unpaid care for older people, such as that provided by a relative or friend.
Types of sourcesThis scoping review considered quantitative, qualitative, and mixed methods study designs for inclusion. Knowledge synthesis reviews that met the inclusion criteria were also eligible. Opinion papers were not eligible for inclusion. Protocols or conference abstracts for which a full-text article was not available were also excluded.
METHODSThis review was conducted in accordance with the JBI methodology for scoping reviews9 and reported according to PRISMA-ScR guidelines (see Appendix I, https://links.lww.com/IJEBH/A159). The objectives, inclusion criteria, and methods for this scoping review were specified a priori in a protocol.10 Variations from the protocol are explained at the end of the Methods section.
Search strategyThe search strategy aimed to locate published studies, and a test search of MEDLINE was undertaken to identify relevant articles on the topic. Text words contained in the titles and abstracts of relevant articles, along with the index terms used to describe the articles, were used to develop a final search strategy, which was adapted and translated across nine databases, including MEDLINE, CINAHL, AgeLine, and ProQuest Social Sciences Premium Collection (see Appendix II, https://links.lww.com/IJEBH/A160). The keywords were developed by a librarian and searches combined four groupings: (1) knowledge terms (knowledge, evidence, or research); (2) setting terms (nursing homes, home care, aged care, long-term care, etc.); (3) age terms (aged, older people, senior, etc.); and (4) implementation terms (barriers or facilitators to implementation, implementation, change, etc.). The initial searches were conducted on August 23, 2022 and were limited by a date range from January 1, 2012 (as our preliminary searches indicated that most relevant papers were published since this date). Only English language papers were included as we did not have capacity for translation. The search strategy was later repeated to capture additional studies published between August 1 and December 31, 2022.
Study/source of evidence selectionFollowing the search, all identified citations were collated and uploaded into EndNote v.20 (Clarivate Analytics, PA, USA) and duplicates removed. The remaining citations were then uploaded into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) for screening. Following a pilot test and minor revisions to clarify the inclusion criteria, titles and abstracts were screened by two independent reviewers. Any disagreements that arose between reviewers were resolved through discussion or by a third reviewer. Potentially relevant sources were retrieved in full and assessed in detail against the inclusion criteria by one reviewer. Where there was uncertainty, papers were discussed with another reviewer before deciding whether to include. Reasons for exclusion of papers at full text were recorded and are reported below.
Data extractionA data extraction tool was developed and piloted by the reviewers for use in Covidence; however, after testing it on 15 papers, we found this software did not allow for inductively coding or grouping the often quite large extracted segments of text where implementation factors were identified. The data extraction tool was adapted for use in NVivo and piloted (see Appendix III, https://links.lww.com/IJEBH/A161), and the included studies were uploaded to NVivo. Data were extracted using the case classification and coding functions of NVivo. The five reviewers each worked on a random selection of papers in separate NVivo files. The data extracted included specific details about the participants, concept, context, study methods, and key findings relevant to the review questions. Text segments that indicated factors influencing the implementation of an innovation were inductively coded.
Data analysis and synthesis of resultsWe employed an inductive descriptive qualitative content analysis approach. Identified factors were discussed among the review team over a series of four workshops to develop categories and sub-categories of factors that influence implementation. Each reviewer then organized their data according to the agreed categories, and NVivo files were merged for further frequency analysis of identified factors and attributes of included studies.
Engagement with knowledge usersThis review was overseen by our Research Advisory Group, comprising aged care consumers and family members, aged care staff from diverse settings, a representative from the Australian Aged Care Quality and Safety Commission, a representative from Dementia Training Australia, representatives from Primary Health Networks and South Australian Virtual Care Service, and aged care researchers. This group met quarterly in a hybrid online/face-to-face format for approximately 1.5–2 hours. Participants were provided with documents and verbal descriptions summarizing the review methods and preliminary findings. They were consulted on the research design, validation of identified factors and categories, and interpretation and contextualization of the findings.
Variation from the review protocolOur protocol included a secondary review objective, to identify how implementation outcomes are defined in aged care implementation research. These outcomes will be examined and reported separately in a forthcoming paper.
Although published guidance suggests including a targeted search for gray literature and screening reference lists of included papers for additional studies, our high yield of included studies meant that we were confident that we would obtain valid findings from the included studies.
We approached the issue of reliability checking data extraction by conducting several workshops to interpret and group our data, which gave us confidence in the consistency of our interpretation and eliminated the need for cross-checking.
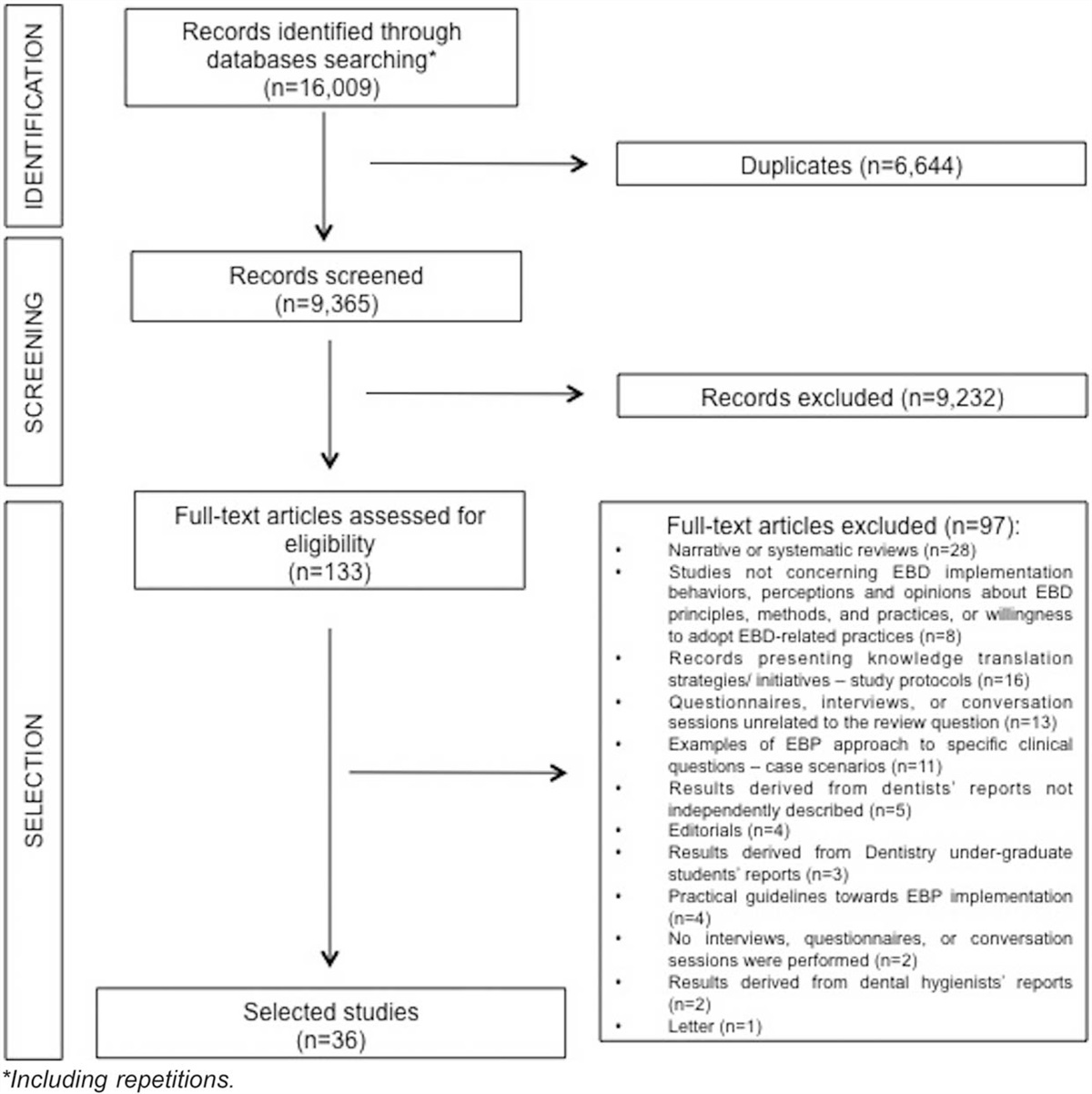
FINDINGS Search and selection of included studiesOf the 2530 retrieved studies, 193 were ultimately included.6,7,11–201 The PRISMA-ScR diagram (Figure 1) shows the study selection process and reasons for full-text exclusion. Details of excluded studies are in Appendix IV, https://links.lww.com/IJEBH/A162.
 Figure 1:
Figure 1: PRISMA-ScR diagram of study selection process.
Attributes of included studiesAppendix V, https://links.lww.com/IJEBH/A163 summarizes the number and proportion of included studies according to their various attributes. The attributes of each included paper are reported in Appendix VI, https://links.lww.com/IJEBH/A164. Of note are the findings regarding the aged care context, consumer involvement, and use of a theory or framework. As detailed in Appendix V, https://links.lww.com/IJEBH/A163, the majority of papers (n = 142, 74%) reported on studies conducted in the residential facility context. Very few studies (n = 28, 15%) involved consumers and/or their families in any stage of the study, and only 28% of the papers (n = 54) used an implementation theory or framework. The most commonly used theories or frameworks were the Normalization Process Theory (n = 9), Integrated/Promoting Action on Research Implementation in Health Services (iPARIHS) (n = 8), and the Consolidated Framework for Implementation Research (CFIR) (n = 5).
The rate of publication of relevant studies grew over the period of investigation, as shown in Figure 2. The most common study countries were the United States (n = 37, 19%), Australia (n = 32, 17%), and the United Kingdom (n = 28, 15%). The focus of the innovations reported was mostly clinical care (n = 94, 49%), followed by personal care (n = 30, 16%).
 Figure 2:
Figure 2: Number of included studies published per year.
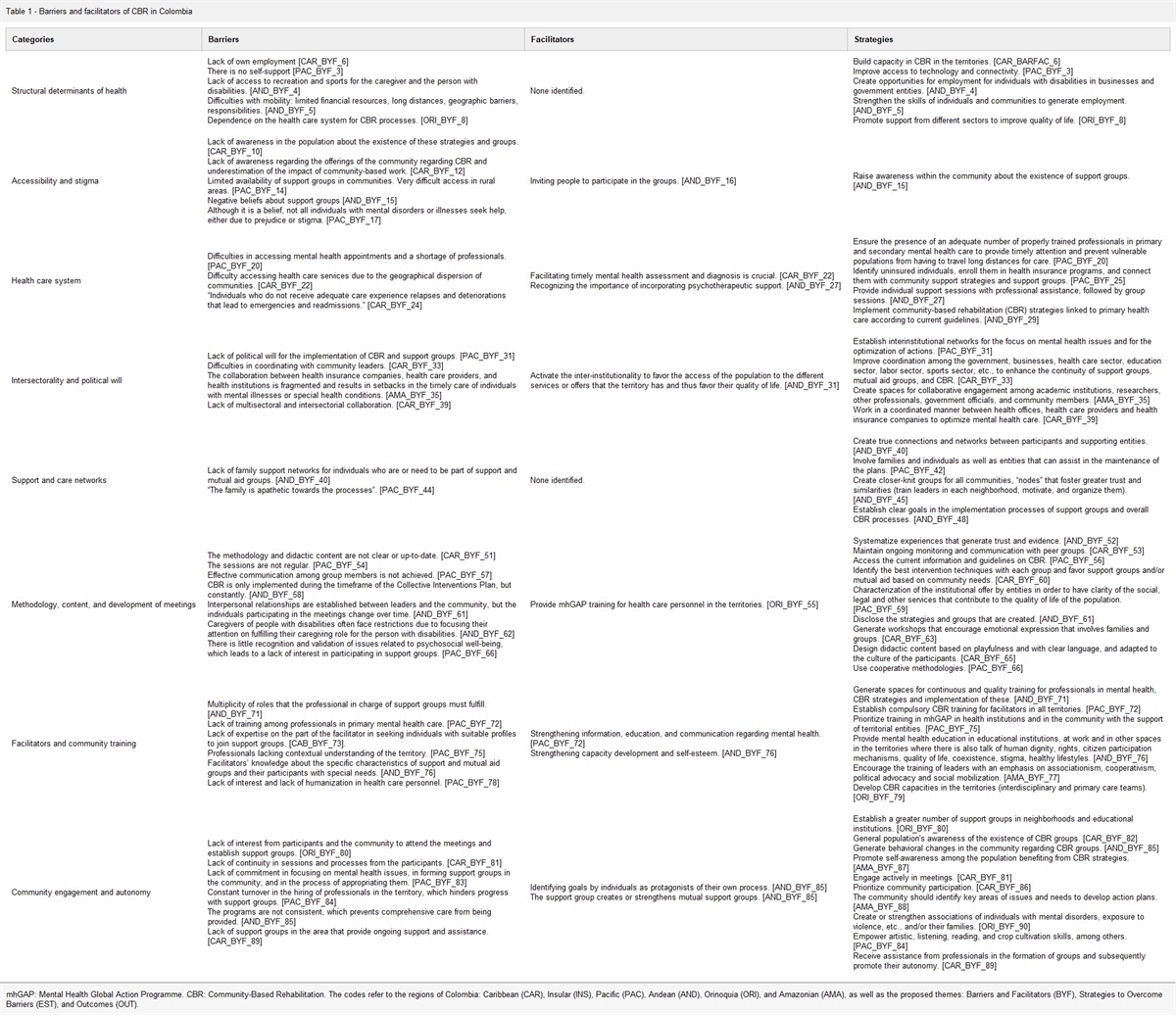
Factors that influence implementation in aged careWe identified five main categories of factors that influence implementation in aged care. Table 1 shows these categories as well as the number and proportion of papers that reported factors in each category.
Table 1 - Main categories of factors that influence implementation Category Papers (n) Papers (%) Organizational context factors 175 91 People factors 162 84 Relational factors 142 74 Innovation factors 129 67 Implementation process actions 128 66Appendix VI, https://links.lww.com/IJEBH/A164 shows which factors were identified in each included paper. Factors relating to the organizational context were prominent in the included studies. Chief among these was the importance of resources, primarily in terms of staffing, workload and time, as well as financial resources, the physical environment and technology infrastructure. Organizational culture was also a prominent sub-category within the organizational context. Particular culture factors we identified included leadership style, staff autonomy, and organizational focus and priorities.
People factors were also a frequently identified category. These related to older people, aged care staff, and/or other stakeholders. There were two main categories of people factors. Firstly, the beliefs and attitudes that people hold in relation to the problem, the innovation, or the change. Secondly, individual capabilities, including individuals’ skills, competencies, knowledge, and understanding regarding the innovation and/or the change process, or background knowledge/skills.
Many relational factors were identified as influencing implementation. We defined these as being about the quality of interactions between stakeholders (aged care staff, consumers, external service providers, plus others) both before and in the process of implementation, noting that they were partly about the existing context, and partly about the implementation process. Most prominent among these was the importance of leaders’ support and backing for the implementation. Collaboration and communication were also important relational factors.
Numerous factors were identified relating to the innovation and its compatibility with the organizational context or appropriateness for the stakeholders concerned. The characteristics and design of the innovation were frequently identified as key to successful implementation. The adaptability or flexibility of the innovation, alignment with existing systems, and acceptability and appropriateness to the target stakeholders were also prominent factors in this category.
A range of factors relating to actions of the implementation process were also identified. These fell into two main sub-categories: (i) stakeholder engagement and involvement and (ii) implementation mechanisms. We defined stakeholder engagement and involvement as the nature and extent of the engagement, involvement, inclusion, and participation of stakeholders in the development of the innovation or its implementation. This sub-category included several factors to do with “bringing people along” during implementation, such as feedback, experience of “early wins” to reinforce the benefit of the innovation, and participation and inclusion. Implementation mechanisms were defined as activities/actions that are done to drive change, to implement the innovation. These included training, champions, facilitation, and knowledge sharing, among others.
Figure 3 shows the five main categories of factors and sub-categories.
 Figure 3:
Figure 3: Main categories and sub-categories of factors that influence implementation in aged care.
DISCUSSIONIn this section, we will first discuss our findings regarding the many factors that influence implementation in aged care before commenting on the shortcomings in the field of aged care implementation research that we have identified, and then noting some limitations of our study, before concluding.
Factors that influence implementationOur review has identified five main categories of factors that influence implementation in aged care: the beliefs, attitudes, and capabilities of people/stakeholders; contextual factors such as resourcing and culture; the fit between the innovation and the context or stakeholders; relational factors in terms of the interactions between stakeholders; and the activities of implementation, including implementation strategies and stakeholder engagement. These categories inherently make sense. If people are not in favor or do not have the skills or knowledge for the change, it will be much harder to implement. If the innovation is just not appropriate, it will not get taken up. If people do not work well together, it is hard to make change. If leaders are not behind it, it is hard to implement anything new. Involving people and using appropriate mechanisms to promote change are important. And perhaps most critically, it is difficult to implement anything new in a resource-constrained environment.
Earlier reviews have examined selected aspects of factors that influence implementation in aged care, focusing on implementation mechanisms in residential settings,6 behavioral influences on implementation of guidelines,7 and clinical care in residential settings.5 They identified many factors similar to those we identified: time, staffing, resources, leadership, champions, strategies,7 receptive context, model of change, resources, staff skills, stakeholder engagement, nature of the change, supportive systems, demonstrable benefits,5 common ground for change, learning by connecting, reconciling competing priorities, and exercising agency.6 Our review provides a more comprehensive analysis than previous reviews in that it examines the whole gamut of influences, including contextual factors, rather than just focusing on individual behavioral factors or implementation mechanisms; it includes a broad scope of innovations that extend beyond a purely clinical focus or implementation of guidelines; and it includes community-based as well as residential care. Our review builds on comparable reviews and generates a comprehensive knowledge base from which to develop resources that provide holistic, contextually appropriate support for implementation efforts.
The factors we have identified as influencing aged care implementation are analogous to the well-established determinants of implementation in health care. The CFIR,202 which is a synthesis of existing implementation theories, comprises five major domains of implementation constructs (the intervention, inner and outer setting, the individuals involved, and the process by which implementation is accomplished). There is much overlap between the CFIR and the categories identified in our review; however, there are two key differences. Our review did not identify the outer setting as a key influence on implementation of innovations within an aged care setting. We did, however, identify the category of “relational factors,” which spans the “setting” (our organizational context) and the “individuals” (our “people factors”). Our findings therefore indicate that implementation in aged care is not dissimilar to implementation in health care. The same sorts of things matter, although how they operate will likely differ between aged care and health care, given key differences in organizational structures and hierarchies, staff capacity, and resourcing. A key implication of our study is that it shows that implementation in aged care is highly complex, and there are many factors across several main categories/domains that can help or hinder change. Implementing innovation in aged care requires a strategic approach, with knowledge of and attention to the stakeholders, the context and the innovation, and the way in which these elements intersect, including interaction between stakeholders. Simplistic approaches and attempts at implementation that do not account for this complexity will rarely succeed.
We have identified resourcing as a prominent category among factors that influence implementation in aged care. The need for reliable resourcing was also a key recommendation of Australia's Aged Care Royal Commission203 in terms of impacting the quality and safety of services provided. Our analysis shows that resourcing is also critical for being able to improve. Where aged care organizations are working with the bare minimum to “keep their heads above water” and provide the basics of care (or not even that, as the Royal Commission showed), their ability to implement improvements is constrained. There needs to be some “fat” or resourcing “slack” so that organizations can implement change well for sustainable improvement. This is recognized in the Alberta Context Tool, where “organizational slack” is defined as “the cushion of actual or potential resources which allows an organization (unit) to adapt successfully to internal pressures for adjustments or to external pressures for changes” and comprises staff, space, and time.204 Appropriate resourcing is of paramount importance and fundamental to having staff, space, and time, and so should be the primary priority for improving aged care. Without adequate resourcing, any efforts at innovation and improvement will be challenged if people and organizations are not afforded the space and opportunity to give suitable attention to it and by necessity, are restricted to the day-to-day, routine work of aged care, with no “slack” for innovation.
Implementation in community-based aged careThe studies in our review predominantly focused on residential aged care with very little research regarding implementation in the context of community-based aged care services. This part of the aged care sector in Australia has grown considerably in recent years, with the number of community-based care consumers more than doubling from around 60,000 in 2015 to over 140,000 in 2020, and provider numbers growing from 504 to 920 in the same period.3 This part of the sector is expected to grow even further, with government policy initiatives and consumer preferences driving significant growth.205
There are significant government reforms to community-based aged care in development as well as many new market entrants offering innovative technology solutions and operating models.205 Understanding how to successfully implement and sustain change with this part of the aged care sector will be increasingly important as growth continues. The lack of contextually relevant research evidence to inform effective implementation, change, and improvement may hinder efforts to improve the quality and safety of community-based aged care services and respond to policy reforms. Our review is the first to examine implementation in community-based aged care as well as residential aged care, and thus offers important findings about the need for more research related to this context.
Consumer involvement in aged care implementation researchOur review made the novel finding that very few aged care implementation studies involved consumers of aged care services; that is, older people and their representatives. Underpinned by the principle of “nothing about us without us,” there is a growing recognition of the importance of involving people in research to ensure that research questions and outcomes are relevant and generate evidence that better reflects the needs of specific groups. The concept of consumer participation and involvement also features prominently in both the current and revised Australian Aged Care Quality and Safety Standards: “meaningful and active partnerships with older people inform organizational priorities and improvements to care and services.”206 Elaborating on this principle, research into the implementation of innovation in aged care should also involve meaningful and active partnerships with older people. Meaningful involvement of consumers, incorporating collaboration and shared leadership, will optimize the real-world applicability of research findings and care interventions. Stakeholders’ “ownership” of a “problem” and involvement in associated research is recognized as a key factor in ensuring that the research has meaningful impact.207
Bodison et al.208 identified four key barriers to community participation in dissemination, implementation, and improvement science from the perspectives of researchers and service providers: (1) communities have historically had little influence over the “problems” to be investigated and setting the research agenda in the first place; (2) key stakeholders are often left out during the development of research projects; (3) people in communities who experience disadvantage and marginalization do not trust researchers and/or large institutions, or their scarce resources and time are put to personal priorities rather than research participation; and (4) research findings are seldom meaningfully communicated to the communities of study, partly because researchers prioritize academic outputs rather than community feedback. Bodison et al. proposed various practical approaches to overcoming these barriers, such as ongoing forums, resources, training, specific funding mechanisms, networking opportunities, and online directories.208
Slattery et al.209 recommend that co-designed research incorporate numerous elements to promote participation of research end-users. Their INVVOLVE framework advises researchers to Invest in co-design; assess Needs; enVision roles, responsibilities, and rewards; Validate participants; Organize interaction carefully; Lead the engagement; Value participant time and input; and Evaluate and report on engagement processes.209 More specifically, Goodwin et al.210 identified a range of factors that affect the inclusion of older people in research (both as subjects and as collaborators)—individual, interpersonal, organizational, community, and policy. They developed a framework of 14 recommendations to promote the inclusion of older people in research to ensure its relevance.
To improve the value and impact of aged care implementation research, ideally, studies would be instigated by consumer and service provider “end users” to address the real-world, priority problems they identify. While there are challenges to involving consumers in implementation research, the benefits to the relevance and applicability of the research warrant the additional effort. We echo recommendations208–210 that “end users” should be actively involved in genuine participatory, power-sharing research to generate meaningful outcomes to inform real, sustainable improvement.
Theoretically-informed implementation research is uncommonOur analysis found that relatively few studies drew on an implementation science framework in either the design or conduct of their implementation efforts or analysis. Implementation frameworks enable implementation practitioners and researchers to describe or guide efforts to translate evidence into practice; analyze and identify the mechanisms by which implementation strategies have effect; and evaluate implementation efforts.211 The application of a framework aids the communication, synthesis, and generalizability of findings. Where an implementation science framework has not been used, it can compromise the viability and success of the implementation efforts. In a practical sense, without the appropriate use of an implementation framework, stakeholders may inaccurately assess the context or develop inappropriate implementation strategies. The translation of implementation research findings into practice may also be compromised by poor use of frameworks, thereby constraining the public health impact of the research. The poor use of frameworks can also slow or misguide the progress of implementation science as a field.212 While we did not assess the appropriateness or quality of the use of implementation frameworks, the finding that some 70% of papers in our study made no mention of any implementation framework is a clear indication that framework use is lacking in the field of aged care implementation research.
Our findings are consistent with those of Sullivan et al.,213 whose citation review identified low but increasing use of implementation theories, models, and frameworks in aging research (not necessarily in the aged care setting) in the USA. Our study builds on this work by examining the aged care context specifically, and including studies from any country. As we have shown, aged care implementation research is produced in various countries, so a broad geographic scope is important for gaining an accurate picture of low theory use internationally.
We identified that the CFIR202 and iPARIHS214 were among the most used frameworks. This was also consistent with the findings of Sullivan et al.213 However, these authors also identified another commonly used framework (Greenhalgh's Diffusion of Innovation in Service Organizations215) that we did not. We also identified Normalization Process Theory216 among the most common, which Sullivan et al. also did not. Moreover, their analysis identified that only 41% of citations meaningfully applied theories, models, or frameworks and only 23% used them throughout the research, further indicating inadequate use.
There are several possible explanations for the limited use of frameworks. The ability to follow clear steps in the implementation process rather than adapting and applying broader concepts has been posited as a reason that some frameworks are applied more than others.213 This is consistent with input from our advisory group, suggesting that a clear, simple, step-by-step process would be more likely to be used. Why such a high proportion of implementation research fails to employ any implementation framework or theory is perhaps harder to explain. It may be that there is limited capacity and capability to find, interpret, and apply implementation frameworks, given the personnel shortages across the aged care workforce. Where there are limited personnel and time for an implementation project, time to engage with implementation science theory may be considered a “luxury.” Training in implementation science also tends to be at postgraduate level, and course options are few. The dauntingly rapid proliferation of frameworks, unfamiliarity of language and inconsistent terminology have also been suggested as contributing to the limited use of implementation frameworks.217 Health care practitioners, including nurses, tend to be pragmatic and action-oriented,217,218 and may not appreciate or may downplay the potential value of a theory-informed approach to implementation efforts. The development of practical tools, underpinned by robust theory, will help to optimize implementation efforts while overcoming the barriers to accessing and applying theory in the resource-constrained environment of aged care.
LimitationsOur review only included papers published since 2012, so may not capture earlier studies. However, we did identify a trend in the growth of aged care implementation research over the last 10 years. In addition, as we included other reviews, it is likely that earlier published findings will have been captured.
We did not undertake formal cross-coder reliability checking in relation to data extraction; however, given our in-depth and robust discussion of data and its interpretation, we are confident that data has been reliably interpreted.
As a scoping review, our study did not formally assess the quality of the included papers, and there was considerable heterogeneity among them. A systematic review that formally assesses the quality of research may be warranted, given the concerns about the lack of theoretical underpinning and consumer involvement we have identified, and impressions of varying research and reporting quality.
We note that there are likely relationships and connections between the categories of factors that we have not explored in this paper; however, we intend to further analyze these in depth in forthcoming papers.
CONCLUSIONSThis review aimed to identify factors that influence the implementation of innovations in aged care. We have identified a complex array of key factors: organizational context factors, people factors, relational factors, factors relating to the innovation, and factors associated with the actions of implementation. We also sought to examine the aged care implementation research literature in terms of the characteristics and focus of research, and the patterns and shortcomings of this literature. We have identified recent growth in aged care implementation research, and a predominant focus on clinical care. Our novel findings highlight important shortcomings in this growing field in terms of the limited use of theory to underpin research, infrequent involvement of consumers to ensure the relevance and value of work, and little attention to community-based services. With the global population aging, and imminent major policy initiatives in numerous countries, aged care is a dynamic sector. Effective implementation of innovative practices and models is needed to ensure continuous improvement.
Implications for researchOur study highlights the need for greater research focus on the growing community-based component of the sector, the need to build capacity to appropriately use implementation theory, and to meaningfully involve consumers to promote robust, useful implementation outcomes. This will also contribute to strengthening the field of implementation science in aged care, building a solid evidence-base to inform future efforts and research.
Implications for practiceOur identification of factors that influence implementation highlights the vital need for adequate resourcing to enable improvement in the sector and provides a rich knowledge base to inform the development of practical tools and resources to support effective, contextually appropriate implementation of evidence-based practice and innovation in aged care.
AVAILABILITY OF DATA AND MATERIALSThe authors are willing to provide access to the data and materials from the studies, if requested.
AUTHOR CONTRIBUTIONSAW wrote the first and subsequent drafts of the manuscript, with comments and revision from AM, CD, LdlP, SC, PR, and GH. AW, CD, PR, AM, LdlP, and SC designed the study, with input from GH. AW, AM, CD, LdlP, and SC conducted study screening and data extraction. AW, AM, CD, LdlP, and SC conducted analysis and interpretation in consultation with GH. CD conceptualized and oversaw all aspects of the project.
ACKNOWLEDGMENTSThe authors wish to acknowledge the members of our Research Advisory Group and greatly appreciate their feedback and contributions throughout this scoping review: Bronwyn Arthur, Nicky Baker, John Cates, Betty Fry, Sandra Glaister, Michelle Hogan, Judith Leeson AM, Alan Patching, Emma Story, Jennifer Thompson, and Christine While.
FUNDINGARIIA is funded by the Australian Government Department of Health and Aged Care. The funders took no part in the review process.
REFERENCES 1. Organisation for Economic Co-operation and Development. Ageing and long-term care [internet]. OECD [cited 2023 Jul 13]. Available from: https://www.oecd.org/els/health-systems/long-term-care.htm 2. Moore CB. Consumer directed care aged care reforms in Australia since 2009: a retrospective policy analysis. Health Policy 2021; 125 (5):577–581. 3. Department of Health and Aged Care Aged Care Financing Authority. Ninth Report on the Funding and Financing of the Aged Care Industry – July 2021 [internet]. Commonwealth of Australia; 2021 [cited 2023 Jun 16). Available from: https://www.health.gov.au/resources/publications/ninth-report-on-the-funding-and-financing-of-the-aged-care-industry-july-2021 4. Henderson J, Willis E. The marketisation of aged care: the impact of aged care reform in Australia. In: Collyer F, Willis K, editors. Navigating private and public health care: experiences of patients, doctors and policy-makers. Palgrave Macmillan; 2019. 249 p. 5. Masso M, McCarthy G. Literature review to identify factors that support implementation of evidence-based practice in residential aged care. Int J Evid-Based Healthc 2009; 7 (2):145–156. 6. Masso M, McCarthy G, Kitson A. Mechanisms which help explain implementation of evidence-based practice in residential aged care facilities: a grounded theory study. Int J Nurs Stud 2014; 51 (7):1014–1026. 7. McArthur C, Bai Y, Hewston P, Giangregorio L, Straus S, Papaioannou A. Barriers and facilitators to implementing evidence-based guidelines in long-term care: a qualitative evidence synthesis. Implement Sci 2021; 16 (1):70. 8. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 2018; 18 (1):143. 9. Peters MDJ, Godfrey CM, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: Scoping reviews (2020 version) [internet]. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. JBI; 2020. Available from: https://synthesismanual.jbi.global 10. Windle A, Champion S, Davy C, de la Perrelle L, Marshall A, Ross P, et al. Factors that influence the implementation of evidence-based practice and innovation in aged care: protocol for a scoping review [internet]. 2022. Available from: https://osf.io/5tzn7 11. Aagaard K, Melendez-Torres GJ, Overgaard C. Improving oral health in nursing home residents: a process evaluation of a shared oral care intervention. J Clin Nurs 2020; 29 (17–18):3392–3402. 12. Abrahamson K, Davila H, Mueller C, Inui T, Arling G. Examining the lived experience of nursing home quality improvement. J Gerontol Nurs 2013; 39 (9):24–30. 13. Abrahamson K, Mueller C, Davila HW, Arling G. Nurses as boundary-spanners in reducing avoidable hospitalizations among nursing home residents. Res Gerontol Nurs 2014; 7 (5):235–243. 14. Ahluwalia SC, Friedman E, Siconolfi D, Saliba D, Phillips J, Shih R. Promises and pitfalls of health information technology for home- and community-based services. J Appl Gerontol 2021; 40 (5):558–565. 15. van den Akker LE, de Waal MWM, Geels PJEM, Poot E, Achterberg WP. Implementation of the multidisciplinary guideline on chronic pain in vulnerable nursing home residents to improve recognition and treatment: a qualitative process evaluation. Healthc 2021; 9 (7): 16. Alamri SH, Kennedy CC, Marr S, Lohfeld L, Skidmore CJ, Papaioannou A. Strategies to overcome barriers to implementing osteoporosis and fracture prevention guidelines in long-term care: a qualitative analysis of action plans suggested by front line staff in Ontario, Canada. BMC Geriatr 2015; 15:94. 17. André B, Grønning K, Jacobsen FF, Haugan G. Joy of life in nursing homes. Health care personnel experiences of the implementation of the national strategy: a qualitative study with content analysis of interviews. BMC Health Serv Res 2021; 21 (1):1–8. 18. Assander S, Bergstrom A, Eriksson C, Meijer S, Guidetti S. ASSIST: a reablement program for older adults in Sweden: a feasibility study. BMC Geriatr 2022; 22 (1):618. 19. Augustsson H, Tornquist A, Hasson H. Challenges in transferring individual learning to organizational learning in the residential care of older people. J Health Organiz Manag 2013; 27 (3):390–408. 20. Badger F, Plumridge G, Hewison A, Shaw KL, Thomas K, Clifford C. An evaluation of the impact of the Gold Standards Framework on collaboration in end-of-life care in nursing homes. A qualitative and quantitative evaluation. Int J Nurs Stud 2012; 49 (5):586–595. 21. Baier RR, McCreedy E, Uth R, Gifford DR, Wetle T. Nursing home leaders’ perceptions of a research partnership. Aging Clin Experiment Res 2021; 33 (12):3371–3377. 22. Bamford C, Heaven B, May C, Moynihan P. Implementing nutrition guidelines for older people in residential care homes: a qualitative study using Normalization Process Theory. Implement Sci 2012; 7 (1):106. 23. Banerjee A, Taylor D, Stranz A, Wahl A. Facilitated reflection meetings as a relational approach to problem-solving within long-term care facilities. J Aging Stud 2021; 59:100965. 24. Bardo AR, Applebaum RA, Kunkel SR, Carpio EA. Everyone's talking about it, but does it work? Nursing home diversion and transition. J Appl Gerontol 2014; 33 (2):207–226. 25. Bartholomeyczik S, Quasdorf T. Influence of leadership on implementing Dementia Care Mapping: a multiple case study. Dementia 2019; 18 (6):1976–1993. 26. Batchelor F, Hwang K, Haralambous B, Fearn M, Mackell P, Nolte L, et al. Facilitators and barriers to advance ca
Comments (0)