
Remember me


Multiple hereditary exostoses (MHE) are an inherited condition affecting approximately 1 in 50,000 individuals and is characterized by benign, cartilage-capped osseous growths1. There are multiple musculoskeletal manifestations including injury to neurovascular structures2. Compression of the peripheral nerves by osteochondromas has been described3–9 (Fig. 1).
 Fig. 1:
Fig. 1: Fig. 1-A Clinical picture of a patient with MHE, a posterolateral prominence, paresthesias, and weakness of the extensor hallucis longus. Fig. 1-B Preoperative, coronal radiograph of the involved tibia and fibula. Fig. 1-C Axial, proton density with fat saturation magnetic resonance imaging scan of the proximal tibia and fibula. Fig. 1-D Postoperative, coronal radiograph of the involved tibia and fibula.
The common peroneal nerve and its branches are at risk for compression as it courses around the fibular head/neck10. One indication to decompress the peroneal nerve and excise proximal fibular osteochondromas is the presence of foot drop (0/5 on manual strength testing of the tibialis anterior); equally important is weakness (≥1 and ≤4/5 on manual strength testing) of the tibialis anterior, peroneus brevis and longus, and extensor hallucis longus11. Other indications have not been adequately defined in the literature. Decompression of the peroneal nerve and excision of osteochondromas is not a benign procedure, with a postoperative foot drop rate between 22.7% and 33%3,12.
To our knowledge, no previous study has focused on the decompression of the peroneal nerve and the excision of proximal fibular osteochondromas exclusively in patients with MHE. The purpose of this study was to report our experience treating this cohort, including approach, indications, complications (all untoward events), and rate of recurrence (return of symptoms and signs of peroneal nerve compression or painful osteochondromas on the proximal fibula after an interval of symptom improvement lasting a minimum of 1 year after the surgical procedure; patients undergoing a revision surgical procedure for prophylaxis [e.g., acute deformity correction] were not considered to have had a recurrence). We hypothesized that most patients’ symptoms would improve with decompression and osteochondroma excision.
Materials and MethodsInstitutional review board approval was obtained for this study. A retrospective review of the records dating from June 1, 2009, to October 31, 2023, was performed to identify Current Procedural Terminology code 64708 (neuroplasty of a major peripheral nerve of the arm or leg). Radiographs and charts were reviewed to identify patients with a diagnosis of MHE. Patients were excluded from analysis if the nerves being decompressed were not the common, superficial, and deep peroneal nerves at the knee.
The records of the patients meeting the inclusion and exclusion criteria were further reviewed to identify indications, approach, complications, location of osteochondroma excision (lateral, posterior, anterior, and/or medial), proximal fibular excision, recurrence, skeletal maturity (no open physes at the distal femur, proximal tibia, or proximal fibula were considered skeletally mature), and need for revision (repeat peroneal nerve decompression at any time after the index decompression). Operative reports were also reviewed for concomitant excision of ischial, posterior proximal femoral, posterior and/or posterolateral distal femoral, and lateral proximal tibial osteochondromas.
Surgical TechniqueThe patient is placed supine with the contralateral knee slightly flexed to take tension off the contralateral nerve. After tourniquet application, an incision is made either laterally in line with the proximal fibula or following the course of the peroneal nerve as it crosses the fibular neck10. Blunt dissection is performed in line with the common peroneal nerve posterior to the biceps femoris attachment.
All patients underwent the initial part of the decompression (i.e., a soft-tissue release, which has been previously described10). In brief, the fascia overlying the nerve is incised both proximally and distally, and a transverse fasciotomy of the anterior and lateral compartments is performed. All vertical septa are transected in the anterior and lateral compartments following the fasciotomy. The nerve is mobilized by releasing the soft-tissue attachments proximal to the lateral compartment.
The second part of the decompression is excision of osteochondromas. The goal of this portion is to remove all osteochondromas surrounding the nerve. For posterior osteochondromas, the interval between the peroneus longus and the soleus is utilized. For lateral osteochondromas, the nerve is gently retracted and the peroneus longus muscle belly is retracted anteriorly. Occasionally, the peroneus longus may need to be detached from its origin and to be reflected distally (Fig. 2).
 Fig. 2:
Fig. 2: Intraoperative photograph of a patient with MHE demonstrating a lateral osteochondroma (purple arrow) distalizing the deep peroneal nerve (green arrow). The peroneus longus has been reflected distally (black arrow).
For anterior osteochondromas and medial osteochondromas, the origin of the peroneus longus is reflected distally to allow for the visualization of the motor branch to the tibialis anterior. The lateral and proximal origin of the extensor digitorum longus and tibialis anterior may also require release to allow for mobilization of the compartment (Fig. 3). It is important to identify the motor branch to the tibialis anterior as osteochondromas can cause displacement of the nerve. For large medial osteochondromas, proximal fibular excision is recommended with preservation of the epiphysis, ligamentous attachments, and joint capsule13.
 Fig. 3:
Fig. 3: Intraoperative photograph of a patient with MHE demonstrating a mobilized extensor digitorum longus (blue arrow) and an anterior osteochondroma (yellow arrow). The previous lateral osteochondroma (purple arrow), deep peroneal nerve (green arrow), and reflected peroneus longus (black arrow) can also be seen.
Following osteochondroma excision, the edges are smoothed, and the knee is taken through a range of motion to ensure that the nerve is uninhibited.
Statistical AnalysisDescriptive statistics were calculated. The Fisher exact test was performed to assess the association of categorical variables. Multivariable, binomial, logistic regression was used to develop a model for predicting complications. Variables used in the model included the location of osteochondromas, previous decompression, age at the time of the surgical procedure, follow-up duration (the time from the surgical procedure to the last follow-up or the time from the surgical procedure to the time of a revision operation), fibular excision, and concomitant excisions. A backward deletion method was used to eliminate variables until the most accurate model was found. Analysis of variance compared the logistic regression model to the null model. An omnibus test was used to assess the goodness of fit. Odds ratios (ORs) were calculated for significant independent variables in the logistic regression model. The Kaplan-Meier method with right censoring was performed for a survival analysis of the recurrence cohort. Significance was set at p < 0.05. All data were analyzed using R (The R Foundation; https://www.R-project.org/).
ResultsThere were 126 surgical cases (86 patients) that met the inclusion and exclusion criteria (Table I). Of the 126 operations, 72 (57.1%) were performed on skeletally immature patients. Thirty (34.9%) of 86 patients had bilateral nerve decompressions and osteochondroma excisions. The median follow-up was 2.0 years (interquartile range [IQR] width, 3.1 years).
TABLE I - Patient Demographic Characteristics Characteristic Value Sex* Female 36 (41.9%) Male 50 (58.1%) Age at index surgery (yr) Median 14.7 Minimum 3.6 Maximum 69.2 IQR width 12.8*The values are given as the number of patients, with the percentage in parentheses.
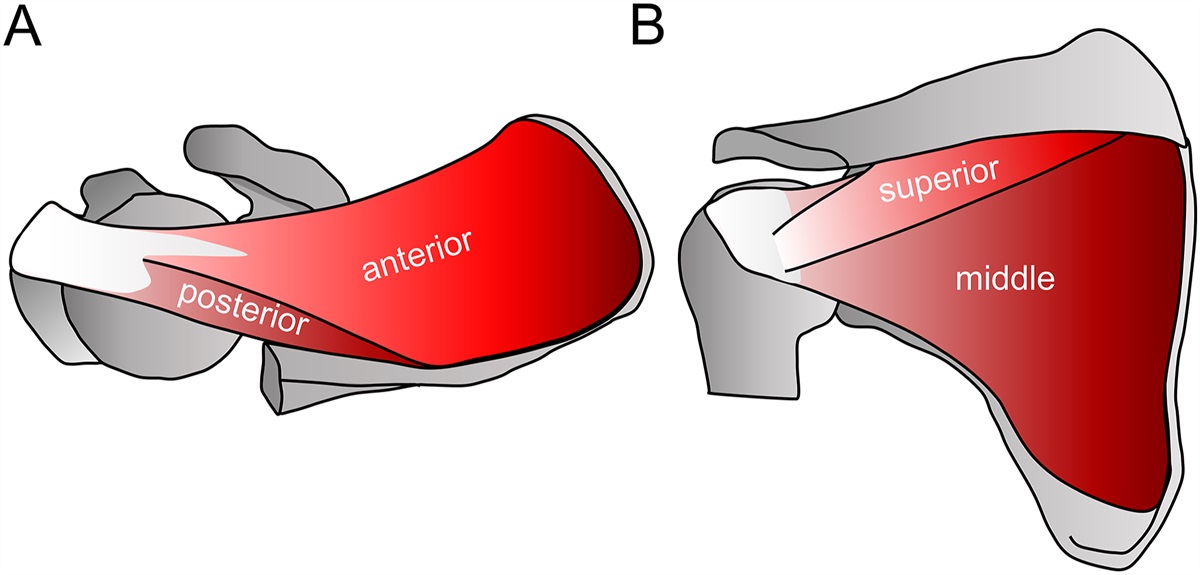
Surgical indications for peroneal nerve decompression and proximal fibular osteochondroma resection are seen in Table II. There were 170 proximal fibular osteochondromas excised (1.3 osteochondromas per case). Figures 4 and 5 illustrate the locations and number of osteochondromas excised. Eleven cases did not have any proximal fibular osteochondromas excised: 4 had posterior distal femoral osteochondromas, 1 had a proximal lateral tibial osteochondroma, and 6 had only the soft-tissue decompression.
TABLE II - Indications for Peroneal Nerve Decompression and Proximal Fibular Osteochondroma Excision Indications No. (%) of Cases Dysesthesias or neuropathic pain 35 (27.8%) Weakness (tibialis anterior or extensor hallucis longus) 23 (18.3%) Pain over the proximal fibula 29 (23.0%) Prominence 3 (2.4%) Foot drop 4 (3.2%) Prophylaxis for acute correction 11 (8.7%) Paresthesias 12 (9.5%) Not documented 9 (7.1%) Fig. 4:
Fig. 4: Locations of the osteochondromas that were excised from the proximal fibula.
 Fig. 5:
Fig. 5: Location of osteochondromas that were excised from locations other than the proximal fibula. These include the posterior proximal femur, posterior/posterolateral distal femur, and lateral proximal tibia.
Six limbs underwent proximal fibular excision; there was concern about instability intraoperatively in 2 cases. In 1 of these cases, the proximal tibiofibular joint was stabilized with a screw, and 1 case had a lateral collateral ligament reconstruction.
Of 126 limbs, 100 improved after the surgical procedure. Improvement could not be ascertained from the charts on 23 limbs: 13 in which the surgical procedure was indicated for prophylaxis, 9 with an unknown indication, and 1 that was lost to follow-up. Three limbs did not improve after the surgical procedure. Two of them had incompletely resected osteochondromas, underwent revision excision, and improved. The third patient, who had weakness for >1 year prior to intervention, still had weakness of the tibialis anterior at 3.3 years.
Twenty complications (15.9%) occurred in this series. They included foot drop (7 cases [5.6%]), neuropathic pain (6 cases [4.8%]), wound breakdown and/or infection (2 cases [1.6%]), implant failure with instability (1 broken screw [0.8%]), and tibialis anterior/extensor hallucis longus weakness (4 cases [3.2%]). Two complications had not completely resolved at the most recent follow-up. One patient still has weakness of the tibialis anterior (follow-up, 1.4 years) following proximal fibular excision. The other had a revision decompression with proximal fibular excision and developed a foot drop and wound breakdown following the surgical procedure. The wound healed and the foot drop showed improvement to a 4/5 tibialis anterior and 4/5 extensor hallucis longus at 5 months postoperatively. All complications were treated with observation except for 3: 2 neuropathic pain complications due to incomplete resection of osteochondromas required revision excision, and a patient with a broken proximal tibial/fibular screw underwent removal and had varus instability at the time of follow-up. There was no association between the indication for the index operation and the occurrence of a complication (p = 0.8937).
A logistic regression model was developed for complications (Table III). Figure 6 is a nomogram for the complication model. The specificity was 0.98, the sensitivity was 0.26, the positive predictive value was 0.71, and the negative predictive value was 0.88. The overall accuracy of the model was 86.9%. There was no difference between the no information rate and the complication model (p = 0.2722).
TABLE III - Multivariable Logistic Regression Model for Complications* Predictor Variables Beta Coefficient OR (95% CI)† P Value Constant −2.39 Excision of anterior osteochondroma 1.65 5.21 (1.60 to 17.02) 0.0062† Proximal fibular excision 2.69 14.73 (2.24 to 96.69) 0.0051† Previous decompression 1.75 5.77 (1.46 to 22.78) 0.0124† Excision of posterior osteochondroma −1.16 0.31 (0.09 to 1.09) 0.0677*All of the osteochondroma locations reference the proximal fibula. Dependent variable = complication (1 = yes or 0 = no). Deviance = 23.21 (p = 0.0001). Goodness of fit: p = 0.0799. CI = confidence interval.
†Significant independent variables.
 Fig. 6:
Fig. 6: Nomogram for the complications logistic regression model.
A total of 11 revision operations (8.7%) were performed: 2 for incomplete resection of osteochondromas, 1 for a second acute deformity correction on the ipsilateral side, and 8 for recurrence of symptoms.
Ninety-one cases met the minimum 1-year follow-up criterion and were included in the recurrence analysis. There were 8 recurrences, which occurred at a mean (and standard deviation) of 4.81 ± 2.55 years after the index operation. The mean age of the patients who experienced recurrence was 9.13 ± 4.57 years at the time of the index procedure. All patients who had recurrence underwent revision decompression and osteochondroma excision. In all except 2 patients with recurrences, the indications for the revision were the same as those for the index procedure. Table IV lists the osteochondroma locations in the patients who had recurrences. There was no association between the initial indication and recurrence (p = 0.1935). There was an association between skeletal immaturity and recurrence (p = 0.0241); all cases of recurrence occurred in skeletally immature patients. A Kaplan-Meier curve and median survival probabilities for skeletally mature and immature patients are seen in Figure 7 and Table V. There were no recurrences in patients who had excision of anterior fibular osteochondromas or lateral proximal tibial osteochondromas. The rate of recurrence for all limbs was 8.8% (8 of 91); however, if the skeletally mature limbs are excluded, then the rate would be 13.8% (8 of 58).
TABLE IV - Osteochondroma Locations for Recurrence Cases* Patient At Initial Surgery Initial Osteochondroma Location Revision Osteochondroma Location Time from Initial Surgery to Revision (yr) Age (yr) Sex 1 3.7 Female Distal femur Distal femur 2.3 2 8.3 Female Posterior fibula Anterior fibula, lateral fibula 2.7 3 13.2 Female Posterior fibula, distal femur Posterior fibula, lateral fibula, distal femur 3.0 4 13.3 Female Posterior fibula Posterior fibula, lateral fibula, anterior fibula 3.0 5 15.4 Male Lateral fibula, distal femur Distal femur 5.7 6 9.5 Female Lateral fibula, distal femur Anterior fibula, posterior fibula, distal femur 6.0 7 4.8 Male Lateral fibula, distal femur Lateral fibula, anterior fibula, posterior fibula, distal femur 6.0 8 4.4 Male Lateral fibula, distal femur Lateral fibula, anterior fibula, posterior fibula, distal femur 9.7 Fig. 7:
Fig. 7: Kaplan-Meier curve for recurrence of symptoms in patients with a minimum 1-year follow-up. The blue line denotes patients who were skeletally mature and the red line denotes patients who were skeletally immature at the time of peroneal nerve decompression. The shading represents the 95% confidence intervals.
TABLE V - Median Survival Probability at 3 and 6 Years 3-Year Probability* 6-Year Probability* Probability of no recurrence Skeletally immature 88% (78% to 100%) 73% (55% to 98%) Skeletally mature 100% (100% to 100%) 100% (100% to 100%)*The values are given as the median, with the 95% confidence interval in parentheses.
To our knowledge, this is the first study to review peroneal nerve decompression and proximal fibular osteochondroma excision exclusively in patients with MHE. Additionally, this is the largest, single-center study to examine peroneal nerve decompression in the setting of osteochondroma(s), whether multiple or solitary3,12.
The most common indications for peroneal nerve decompression and osteochondroma excision were neuropathic pain and/or dysesthesias (pain in the superficial or deep peroneal nerve dermatomes), weakness of the tibialis anterior and/or extensor hallucis longus, and/or pain over the proximal fibula/osteochondromas. In the study by Birch et al., 29% of their patients had neurologic findings and 71% had pain3. In the current study, if all neurologic indications were combined, 59% of patients had a neurologic symptom and 23% had pain. Painful osteochondromas should be elicited by history prior to palpation.
Foot drop is a sequela of peroneal nerve compression and/or entrapment11. A preoperative foot drop was the indication for a surgical procedure in 4 limbs (3.2%), all of which completely recovered during the postoperative period. Birch et al. found that 8 of 9 patients recovered and did not require orthotics following decompression3. The return of tibialis anterior function is unpredictable; it is recommended that nerve decompression and osteochondroma excision be performed prior to foot drop14.
Prophylactic peroneal nerve decompression is recommended when performing osteotomies of the proximal tibia from valgus to varus, especially when there is radiographic evidence of osteochondromas on the anterior and lateral proximal fibula10. A notable indication that is missing from this series is concern about possible malignancy15.
Most patients improved following the surgical procedure. Two patients, both pediatric, underwent a revision surgical procedure within 1 year due to incomplete resection. Both improved following their revisions. An adult patient had long-standing weakness of the tibialis anterior and extensor hallucis longus prior to decompression, and the weakness persisted at the most recent follow-up (3.3 years).
It is important to assess patients with MHE for multiple sites of compression and not just the proximal fibula. This includes the spine, ischium, proximal femur, distal femur, and proximal tibia5,6. Sixty percent of cases in this series also had an osteochondroma removed from a location other than the proximal fibula, which might have compressed the nerve (Fig. 5). Full-length coronal and sagittal views of the lower extremities are routinely ordered prior to the surgical procedure. If the diagnosis is unclear, additional advanced imaging is warranted.
In this study, electromyography (EMG) and nerve conduction studies (NCS) were not routinely obtained prior to decompression and excision. In a study by Cardelia et al., EMG and NCS were performed on all patients preoperatively16. Interestingly, EMG and NCS revealed changes in the peroneal nerve in all of these patients, even though one-half of the patients had little or no neurologic deficit preoperatively16. EMG and NCS are recommended if there is a question regarding the location of nerve compression or if quantitative findings are desired.
This study showed a 16% complication rate following peroneal nerve decompression and fibular osteochondroma excision. The most common complication was foot drop, which occurred after 7 operations (5.6%). Table VI lists foot drop rates from this current study and previous studies for comparison. Six of the 7 cases completely resolved, and the remaining foot drop improved to 4/5 muscle strength of the tibialis anterior and extensor hallucis longus at 5 months postoperatively. All were managed with orthotics until the patient was able to actively dorsiflex. The potential reasons for injury were excessive perineural dissection or overzealous retraction and/or manipulation3.
TABLE VI - Comparison of Rates of Iatrogenic Foot Drop Across Different Studies Study Total Cases Iatrogenic Foot Drop* Present study 126 7 (5.6%) Birch et al.3 (2021) 22 5 (22.7%) Wirganowicz and Watts12 (1997) 10 3 (30.0%)*The values are given as the number of patients, with the percentage in parentheses.
The complication regression model was significantly different from the null model and fit the data well. The nomogram (Fig. 6) is useful for surgeons counseling patients who have had previous decompression (OR, 5.77) or require excision of an anterior proximal fibular osteochondroma (OR, 5.21). Reflecting the origins of the peroneus longus and extensor digitorum longus to mobilize the compartment and visualize and protect the nerve prior to osteochondroma excision may help to minimize this risk. The origins were repaired and protected with a CAM walking boot for 4 weeks.
Proximal fibular excision was reserved for cases with large medial osteochondromas. Proximal fibular excision (OR, 14.73) also increased the odds of a complication. Medial osteochondromas may elicit pain by lateralizing the fibular head and tensioning the peroneal nerve. Another possibility is that a medial osteochondroma can compress the anterior tibial artery as it crosses the interosseous membrane and cause claudication. In such cases, contrast-enhanced advanced imaging is recommended.
Patients undergoing proximal fibular excision have a risk of varus laxity17. It is routine practice to assess stability intraoperatively after proximal fibular excision. In 4 of 6 patients, the proximal fibular epiphysis, joint capsule, and lateral collateral ligament were not disturbed, and the knee was stable. One patient had the entire proximal fibula excised including the epiphysis, and a previously described technique was utilized to secure the lateral collateral ligament to the tibia18. Another patient had a screw placed to secure the proximal fibula to the tibia19. This screw broke and the patient developed pain; an operation was required for removal. The patient has varus instability awaiting reconstruction.
No studies have specifically addressed recurrence in the MHE population to our knowledge. Recurrence, for purposes of this study, was defined as a return of symptoms following at least 1 asymptomatic year. All limbs that experienced recurrence had a new osteochondroma that was detected at least 2 years after the initial surgical procedure (Table IV). Additionally, 7 of 8 cases had an osteochondroma excised at the time of revision from a location that was similar to that treated during the index procedure.
All recurrences happened in patients who were skeletally immature. Osteochondromas are benign tumors20; however, the physes of skeletally immature patients with MHE are affected by genetic mutations (EXT1, EXT2) and additional osteochondromas can grow after previous ones have been resected21.
A previous study of 114 osteochondromas documented a recurrence rate of 2% at a minimum 2-year follow-up22. Our study found a 9% recurrence rate at a minimum 1-year follow-up. If all skeletally mature patients were excluded, the recurrence rate would be 14% at a minimum 1-year follow-up and 18% at a minimum 2-year follow-up. The location and diagnosis (MHE compared with solitary) were not discussed in the former study and may contribute to the differences between that study and ours. Birch et al. reported no recurrences following surgical excision of a proximal fibular osteochondroma in 31 limbs, but they did not document the duration of follow up in their study3.
The Kaplan-Meier curve (Fig. 7) and median survival probabilities (Table V) demonstrate the probability of remaining asymptomatic after the surgical procedure. In skeletally immature patients, it may be prudent to decompress the peroneal nerve only when neurologic symptoms are present to avoid the increased odds of complications that come with a reoperation. If the nerve requires decompression, the excision of all surrounding osteochondromas should be performed.
There were limitations to this study. As a retrospective study, the data were based on what was recorded in the medical record. Additionally, this study did not show electrophysiologic findings, which could quantitatively define the presence of peroneal nerve compression. This study did not quantify or qualify the amount of scarring, adhesion, or the size of osteochondromas, which may also play a role in recurrence. Lastly, due to the high number of cases without complications compared with those with the complication, the regression model was not different from the no information rate, suggesting similar accuracy and its imperfection as a model. Despite such limitations, this study provides valuable information for any surgeon performing these procedures.
In conclusion, neuropathic pain or dysesthesia, weakness, and pain from osteochondromas are the 3 most common indications for peroneal nerve decompression or osteochondroma excision in patients with MHE. The excision of anterior osteochondromas, proximal fibular excision, and previous decompression significantly increase the odds of a complication, but the majority of complications resolve without intervention. The recurrence of symptoms was found only in skeletally immature patients. The nomogram for complications and the Kaplan-Meier curve for recurrences are valuable tools that assist surgeons in counseling their patients.
Note: The authors thank the tireless efforts of the MHE Research Foundation, Brooklyn, NY (mherf.org) for their support of families and patients with MHE, advocating public awareness and spearheading the efforts of biomedical and clinical research on this rare disease.
References 1. Shapiro F, Simon S, Glimcher MJ. Hereditary multiple exostoses. Anthropometric, roentgenographic, and clinical aspects. J Bone Joint Surg Am. 1979 Sep;61(6A):815-24. 2. Schmale GA, Conrad EU 3rd, Raskind WH. The natural history of hereditary multiple exostoses. J Bone Joint Surg Am. 1994 Jul;76(7):986-92. 3. Birch CM, Smit KM, Sucato DJ. Peroneal nerve function before and following surgical excision of a proximal fibular osteochondroma. J Pediatr Orthop. 2021 Jan;41(1):61-6. 4. Demiroğlu M, Özkan K, Kılıç B, Akçal A, Akkaya M, Özkan FÜ. Deep peroneal nerve palsy due to osteochondroma arising from fibular head and proximal lateral tibia. Int J Surg Case Rep. 2017;31:200-2. 5. Aldashash F, Elraie M. Solitary osteochondroma of the proximal femur causing sciatic nerve compression. Ann Saudi Med. 2017 Mar-Apr;37(2):166-9. 6. Trager RJ, Prosak SE, Getty PJ, Barger RL, Saab ST, Dusek JA. Ischial osteochondroma as an unusual source of pregnancy-related sciatic pain: a case report. Chiropr Man Therap. 2022 Oct 17;30(1):45. 7. Kale SY, Gunjotikar AR, Sane RM, Singh S, Dhar SB, Patil RL. Osteochondroma presenting clinically with carpal tunnel syndrome in a 12-year-old boy. J Orthop Case Rep. 2021 May;11(5):109-12. 8. Yamamoto T, Tanaka K, Nagira K, Marui T, Akisue T, Kurosaka M, Mizuno K. Intermittent radial nerve palsy caused by a humeral osteochondroma: a case report. J Shoulder Elbow Surg. 2002 Jan-Feb;11(1):92-4. 9. Karakurt L, Yilmaz E, Varol T, Ozdemir H, Serin E. [Solitary osteochondroma of the elbow causing ulnar nerve compression: a case report]. Acta Orthop Traumatol Turc. 2004;38(4):291-4. Turkish. 10. Nogueira MP, Paley D. Prophylactic and therapeutic peroneal nerve decompression for deformity correction and Lengthening. Oper Tech Orthop. 2011;21(2):180-3. 11. Abdel MP, Papagelopoulos PJ, Morrey ME, Wenger DE, Rose PS, Sim FH. Surgical management of 121 benign proximal fibula tumors. Clin Orthop Relat Res. 2010 Nov;468(11):3056-62. 12. Wirganowicz PZ, Watts HG. Surgical risk for elective excision of benign exostoses. J Pediatr Orthop. 1997 Jul-Aug;17(4):455-9. 13. Mootha AK, Saini R, Dhillon M, Bali K, Dhatt SS, Kumar V. Modified resection technique for proximal fibular osteochondromas. Orthop Traumatol Surg Res. 2011 Sep;97(5):569-73. 14. Lu JCY, Dengler J, Poppler LH, Van Handel A, Linkugel A, Jacobson L, Mackinnon SE. Identifying common peroneal neuropathy before foot drop. Plast Reconstr Surg. 2020 Sep;146(3):664-75. 15. Bovée JVMG. Multiple osteochondromas. Orphanet J Rare Dis. 2008 Feb 13;3:3. 16. Cardelia JM, Dormans JP, Drummond DS, Davidson RS, Duhaime C, Sutton L. Proximal fibular osteochondroma with associated peroneal nerve palsy: a review of six cases. J Pediatr Orthop. 1995 Sep-Oct;15(5):574-7. 17. Agarwal DK, Saseendar S, Patro DK, Menon J. Outcomes and complications of fibular head resection. Strategies Trauma Limb Reconstr. 2012 Apr;7(1):27-32. 18. Bickels J, Kollender Y, Pritsch T, Meller I, Malawer MM. Knee stability after resection of the proximal fibula. Clin Orthop Relat Res. 2007 Jan;454(454):198-201. 19. van den Bekerom MPJ, Weir A, van der Flier RE. Surgical stabilisation of the proximal tibiofibular joint using temporary fixation: a technical note. Acta Orthop Belg. 2004 Dec;70(6):604-8. 20. Zak BM, Crawford BE, Esko JD. Hereditary multiple exostoses and heparan sulfate polymerization. Biochim Biophys Acta. 2002 Dec 19;1573(3):346-55. 21. Pacifici M. The pathogenic roles of heparan sulfate deficiency in hereditary multiple exostoses. Matrix Biol. 2018 Oct;71-72:28-39. 22. Humbert ET, Mehlman C, Crawford AH. Two cases of osteochondroma recurrence after surgical resection. Am J Orthop (Belle Mead NJ). 2001 Jan;30(1):62-4.
Comments (0)