
Remember me


The study was performed between 12 November 2020 and 3 March 2023. Participants received oral semaglutide for a median (range) of 36.1 (0.1–87.7) weeks; the corresponding in-study and on-treatment median observation periods were 40.7 (3.7–87.9) and 36.3 (0.1–87.7) weeks, respectively.
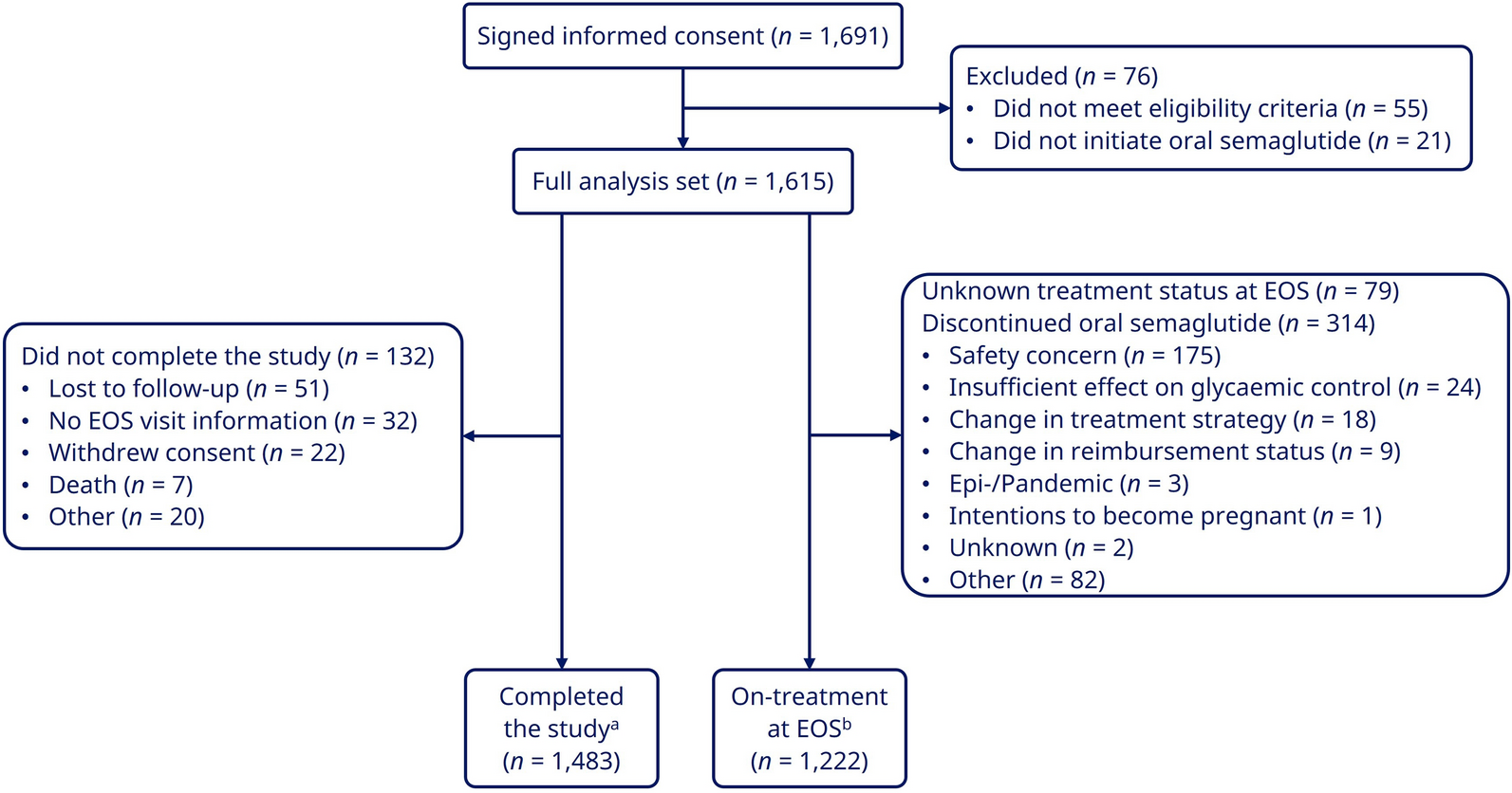
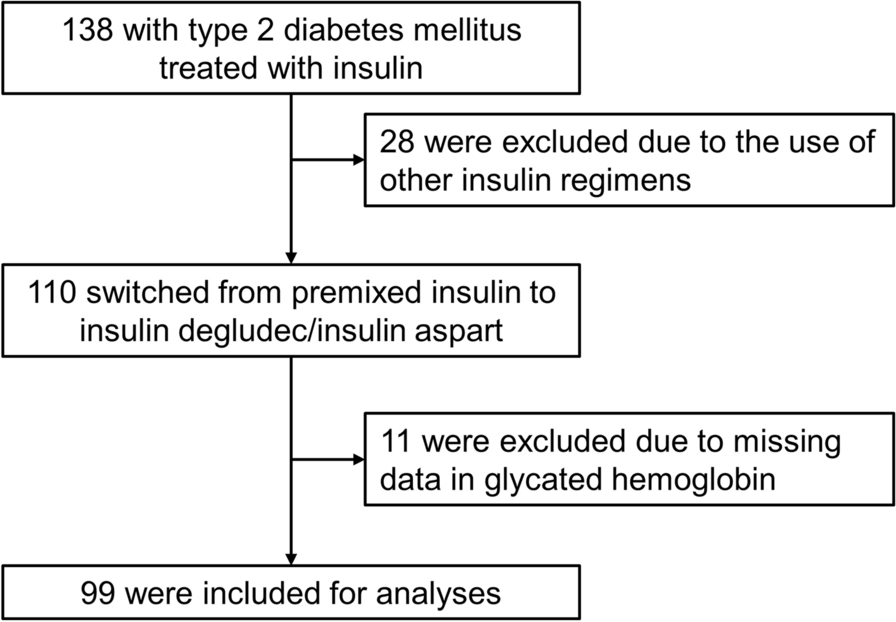
Overall, 187 participants were enrolled and received oral semaglutide (the FAS); 141 were still on oral semaglutide treatment at the EOS visit (Fig. 1).
Fig. 1
Participant disposition. Abbreviations: EOS end of study, n number of participants. †Participants who initiated oral semaglutide and attended the EOS visit. ‡Participants who were taking oral semaglutide and attended the EOS visit
A total of 178 participants attended visit 2, nine participants had no intermediate visit between visits 2 and 3, 68 participants had one intermediate visit, 49 participants had two intermediate visits, 31 participants had three intermediate visits and 30 participants had four or more intermediate visits. As a result of the COVID-19 pandemic, 31 (17.4%) participants attended visit 3 at 45–52 weeks and eight (4.5%) participants attended visit 3 after 52 weeks.
Participant characteristics are summarised in Table 1. Most participants were aged 45–65 years, and 17.1% were ≥ 75 years old. Participants had a mean (SD) T2D duration of 6.8 years (5.7) at baseline. Mean (SD) HbA1c was 7.7% (1.2) and 72.2% of participants had an HbA1c level of ≥ 7% at baseline.
Table 1 Participant demographics, baseline characteristics and initiation of oral semaglutide (FAS)The most common concomitant medications for the treatment of diabetes among participants were metformin (78.6%) and SGLT2 inhibitors (21.4%). Of participants with available data, 78 (41.7%) were current or past smokers, 54 (50%) stated that their highest level of education was high school or equivalent and 60 (42.6%) were retired.
Most of the participants had a physician in primary care (n = 184; 98.4%) and 149 (79.7%) participants had a physician with previous experience with prescribing GLP-1RAs. Nearly all physicians prescribed a starting oral semaglutide dose of 3 mg. Oral semaglutide was primarily prescribed to improve glycaemic control and/or reduce body weight (Table 1).
Approximately two thirds of participants had a CV-related medical history and nearly three quarters of participants met an expanded definition of CV disease, including CKD, haemoglobinopathy, dyslipidaemia and microalbuminuria (Table 1).
Glycaemic and Weight Changes Over TimeThere was a significant reduction from baseline to EOS in HbA1c, assessed in 177 participants, as shown by an estimated mean (95% CI) change of − 0.88%-points (− 1.01 to − 0.75; P < 0.0001) or − 9.64 mmol/mol (− 11.05 to − 8.22; P < 0.0001; Fig. 2A). The estimated mean decreases in HbA1c occurred primarily within the first 28 weeks of treatment (Fig. 2B).
Fig. 2
Estimated change from baseline to week 38 in HbA1c and body weight, for A HbA1c (N = 177), B HbA1c over time (N = 177), and C body weight (N = 165) (FAS); D Proportion of participants achieving HbA1c < 7%, and composite endpoints of HbA1c and body weight reduction. Figure 2B At week 0, observed mean at baseline for participants having at least one post-baseline assessment is plotted. The outer lines of the band represent 95% CI. Abbreviations: CI confidence interval, FAS full analysis set, HbA1c glycated haemoglobin, N number of participants included in the analyses
Secondary and sensitivity analyses of the primary endpoint yielded comparable results. The secondary analysis of the primary endpoint revealed little difference between the ‘in-study’ and ‘on-treatment’ periods. The additional sensitivity analysis showed that the COVID-19-related amendment to extend visit 3 to outside the 34–44-week window had very little impact on the primary endpoint (Fig. S1).
Body weight decrease from baseline to EOS was assessed in 165 participants. Body weight significantly decreased, as shown by estimated mean (95% CI) relative and absolute changes of − 4.72% (− 5.58 to − 3.86; P < 0.0001) and − 4.62 kg (− 5.46 to − 3.79; P < 0.0001), respectively (Fig. 2C). The percentage of participants who had a body weight reduction ≥ 10% from baseline to EOS was 13.7%.
Glycaemic and Weight ThresholdsOverall, 64.6% of participants had a HbA1c < 7% by EOS, compared with 27.8% at baseline; among the 72.2% of participants with a baseline HbA1c of ≥ 7%, over half achieved HbA1c < 7% (Fig. 2D). In addition, 28.5% and 22.9% of participants achieved the composite endpoints of a reduction in HbA1c of ≥ 1%-point with body weight reduction of ≥ 3% and ≥ 5% by EOS, respectively (Fig. 2D). Furthermore, the estimated mean change from baseline in waist circumference (cm) was − 4.15 (SD [95% CI], 0.64 [− 5.44 to − 2.87]; P < 0.0001).
Participant- and Physician-Reported OutcomesParticipants reported a significant increase in their treatment satisfaction with oral semaglutide compared with treatment before initiating oral semaglutide (Fig. 3A, B). The dosing conditions questionnaire revealed that most participants found oral semaglutide very easy to consume (Fig. 3C); further details on dosing conditions are in Table S1.
Fig. 3
Participant-reported satisfaction and ease of treatment to consume: A absolute treatment satisfaction measured with DTSQs, B relative treatment satisfaction measured by DTSQc, and C ease of consumption for oral semaglutide, measured by the dosing conditions questionnaire. Abbreviations: CI confidence interval, DTSQc Diabetes Treatment Satisfaction Questionnaire change, DTSQs Diabetes Treatment Satisfaction Questionnaire status, EOS end of study, N number of participants in the analysis, SD standard deviation. †Observed change was also 12.3 (SD 6.98)
Overall, when judged against their reason for initiating oral semaglutide (Table 1), physicians considered treatment a clinical success in 130 (73.9%) cases. More specifically, physicians reported that glycaemic control was improved in 72.9% of participants, body weight was reduced in 71.6% of participants and convenience was achieved for 60.0% of participants. In addition, there were no issues with hypoglycaemia in 95.7% of participants while they were receiving oral semaglutide. Almost half (46.2%) of participants achieved clinical success in relation to addressing CV risk as reported by their physicians and 40.2% in relation to simplifying the current treatment regimen for participants (Table S2).
In the dosing conditions questionnaire, 60.0% of participants who responded rated oral semaglutide as 6 on the easy to consume scale (0 being very difficult and 6 being very easy) and 86.4% of participants gave a 4, 5 or 6 for this response (Table S1).
Treatment PatternsAt EOS, among 141 participants still taking oral semaglutide, only nine (6.4%) remained on semaglutide 3 mg, whereas 56 (39.7%) participants were taking semaglutide 7 mg at EOS. Additionally, 75 participants (53.2%) had increased to the maximum 14 mg dose and one participant had temporarily discontinued oral semaglutide at EOS.
Twenty-four participants (12.8%) had a new glucose-lowering medication added, or increased the baseline glucose-lowering medication dose, during the study period. Conversely, 13 participants (7.0%) had a glucose-lowering medication removed or the dose reduced during the study period.
SafetyOverall in the in-study observation period, 48 participants (25.7%) experienced a total of 68 AEs; most were mild or moderate in severity and nine participants (4.8%) experienced serious AEs. Most AEs were considered probably related to study drug (Table 2). AEs that led to study-drug withdrawal were reported in 25 participants. The most common AEs occurred in the system organ class of gastrointestinal disorders. One case of severe hypoglycaemia was reported by one participant (0.5%); this participant was not receiving insulin or sulfonylurea. The participant also had known hypertension and was receiving treatment with empagliflozin, metformin and enalapril in addition to oral semaglutide. The blood glucose levels of this participant are unavailable, and the severe hypoglycaemia was classified according to the criteria stated in the endpoints safety section.
Table 2 Summary of AEs over the in-study period (FAS)One fatal AE was reported in a 77-year-old woman who died as a result of disseminated uterine cancer 250 days after treatment initiation; the death was deemed unlikely to be related to study drug.
Comments (0)