
Remember me


Fibromyalgia syndrome (FMS) is a form of chronic widespread pain in the classification of chronic primary pain by the International Classification of Diseases 11th revision (ICD-11). This syndrome is defined as diffuse musculoskeletal pain in at least four of five body regions and in at least three or more body quadrants (as defined by the upper–lower/left–right parts of the body) and axial skeleton (neck, back, chest, and abdomen) [1]. It is associated with sleep disorders, cognitive dysfunction, and somatic symptoms. A diagnosis of FMS is established if the pain is not directly attributable to a nociceptive process in these regions and if there are features consistent with nociplastic pain [1].
Patients with FMS present a lower pain threshold, which generates a condition of diffuse hyperalgesia and/or allodynia. This indicates that there may be a problem with the amplification of pain or with sensory processing in the central nervous system (CNS) [2]. Pharmacological treatment alone is inadequate for most patients who suffer from FMS. Considering the different mechanisms of pain sensitivity, multidisciplinary treatment programs are recommended to target the peripheral, central, cognitive–emotional, and interpersonal causes of chronic pain [2].
Spinal cord stimulation (SCS) has been reported to be effective for neuropathic and ischemic pain, as well as central pain [3]; however, few studies have addressed the effectiveness of SCS for FMS pain [4]. Patients with FMS suffer from refractory chronic pain and limited daily activity. As we supposed that SCS might be an option to improve the refractory pain that accompanies FMS, we conducted a 1-week, temporary SCS trial. The pain was alleviated after 1000-Hz stimulation, without irritation; therefore, leads and an internal pulse generator (IPG) were implanted in the patients. We report two cases in which SCS at 1000 Hz was effective against chronic lower-limb pain in patients with FMS.
The authors obtained written informed consent from the patients regarding the publication of this case report and the use of related data.
Case presentationCase 1A 57-year-old woman who began to feel weakness in her lower legs around the age of 46 and gradually developed generalized pain was diagnosed with FMS by her previous physician. In our hospital, the diagnosis was confirmed by the American College of Rheumatology 1990 Criteria. She was treated with oral medication and physiotherapy, but had difficulty in controlling her pain; thus, she was referred to our department at age 51. The oral administration of pregabalin, duloxetine, neurotropin®, tramadol, and clonazepam helped ameliorate the pain, and the patient was able to continue with her daily life. However, from age 53, the pain in her lower limbs worsened, and she had difficulty in walking. Lumbar spine magnetic resonance imaging revealed a bulge in the lower lumbar spine disks and mild dural sac exclusion, but no significant spinal canal stenosis (Fig. 1A). After providing the patient with sufficient explanation, a 1-week SCS trial for the management of pain in the lower limbs was conducted. During the trial, the patient complained of discomfort from the SCS (10 Hz). However, the pain in the lower limbs was reduced (numerical rating scale [NRS] 6–7 to 1), and the gait difficulty was improved after 1000-Hz stimulation, without irritation. Therefore, SCS implantation (Medtronic® 1000 Hz) was performed (Fig. 1B), after which the patient felt almost no pain in the lower limbs, the dose of oral medication was reduced to only tramadol and duloxetine and could return to her daily life (The final setting: amplitude 3.0 mA, pulse width 60 μs, frequency 1000 Hz).
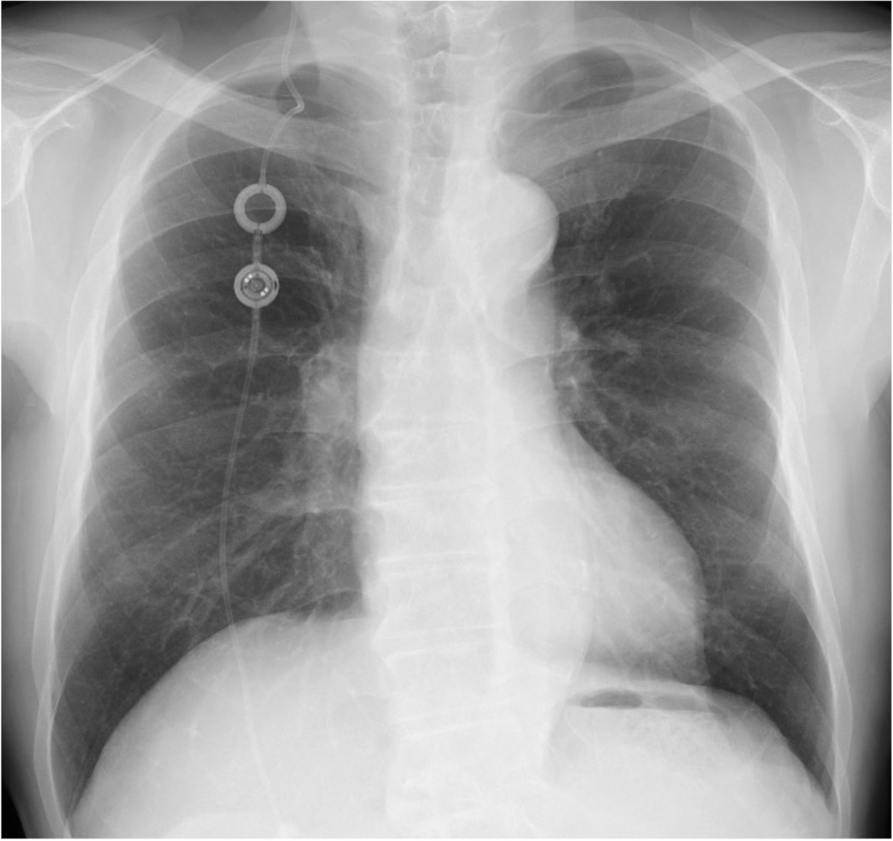
Fig. 1
Preoperative and postoperative photographic images of Case 1. A Preoperative magnetic resonance image of the lower spine. Spinal canal stenosis was not observed. B Abdominal radiograph after SCS placement
Case 2The patient was a 64-year-old woman. After a traffic accident at the age of 47, there was an onset of pain in the area from the left cervical region to the arm, as well as discomfort in the lower legs. Radiographic findings revealed a suspected bone injury in the uncinate process of the seventh cervical vertebra. Therefore, a traumatic cervical syndrome was diagnosed, and the patient underwent drug and block therapies such as facet joint block. From around age 49, the pain spread throughout her body, and the patient was diagnosed with FMS by the American College of Rheumatology 1990 Criteria. Treatment with oral medication (gabapentin, tramadol, and pregabalin) and physiotherapy were initiated, and a posterior cervical medial branch block was performed. However, from the age of around 60 years, the pain in the lower limbs worsened, and she had difficulty walking. Because her tolerance toward the oral medication was low and it was challenging to increase the dose so controlling pain could be controlled, a 1-week SCS trial was conducted for the management of pain in the upper and lower limbs. During the trial, 1000-Hz stimulation was attempted because the patient complained that the stimulation (10 Hz) was unpleasant; after SCS, the patient found that the pain in the upper and lower limbs was ameliorated (NRS 6 to 4) and that it became easier to move up and down stairs. Furthermore, the stiffness of the patient’s hands was reduced. At the age of 61 years, SCS implantation was performed for pain relief in the upper and lower limbs (Medtronic® 1000 Hz) (Fig. 2A, B). After implantation, the dose of oral medication was reduced to tramadol taken only once and her gait difficulty was ameliorated (The final setting: amplitude 4.5 mA, pulse width 90 μs, frequency 1000 Hz for both electrodes in the cervical spine and in the lower thoracic spine).
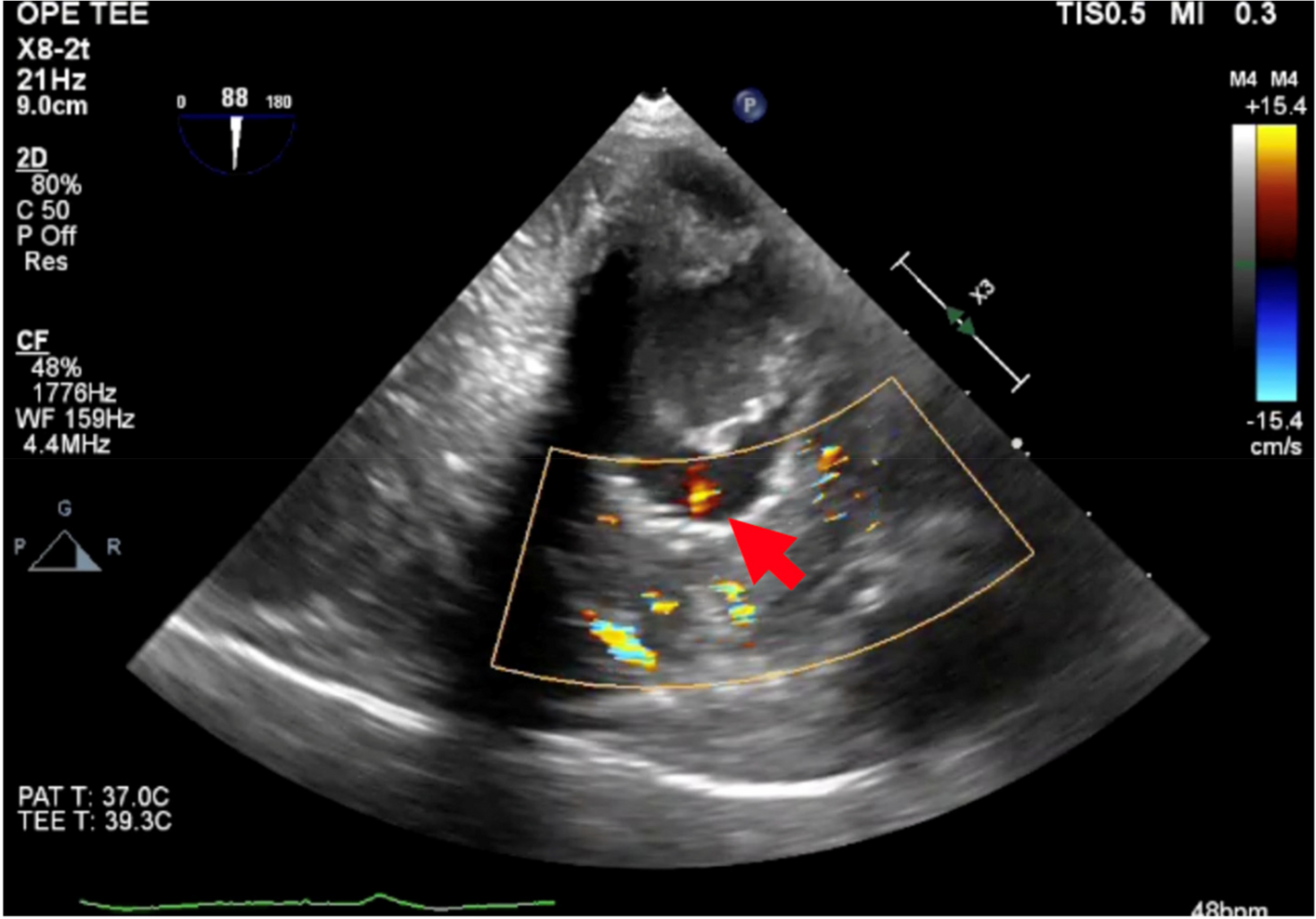
Fig. 2
Radiograph of case 2 after SCS placement. A Cervical radiograph after SCS implantation. B Thoracic radiograph after SCS implantation
Comments (0)