
Remember me

Bilateral leg edema (BLE) in patients with cancer may occur because of malnutrition, thromboembolism, or lymphedema.1,2 In patients with malnutrition, control of cancer cachexia is required in addition to systemic treatment for cancer.3,4 Further, to control BLE it is important not only to treat the causative lesion that impedes blood and lymphatic flow but also to provide systemic treatment of the underlying malignancy. Although BLE most often occurs in patients with urologic and gynecologic cancers,1 refractory BLE can also develop from lung cancer because of metastasis to intraperitoneal lymph nodes or malnutrition.5,6
There have been two major advances in the treatment of advanced lung cancer in the past 20 years. One is the discovery of driver genes and the emergence of tyrosine kinases that act specifically on each driver gene.7 These agents are used for first-line treatment and are expected to have a high response rate. Therefore, it is possible to treat refractory BLE with these tyrosine kinases, but it is difficult to treat BLE that develops after these drugs are no longer effective.
The other development regards immune checkpoint inhibitors (ICIs),8 which are drugs that bind to inhibitory receptors and block inhibitory signal transduction, releasing the brakes on the immune system and enhancing the immune response to tumors.8 Although ICIs can cause immune-related adverse reactions (IRAEs),9 the IRAE frequency is low. However, malnutrition due to colitis with severe diarrhea, pericarditis,10 hepatotoxicity,11 and circulatory disturbance due to IRAEs to lower extremity soft tissue are reported causes of BLE.12,13 Many patients who develop IRAEs recover with corticosteroids.
In addition to systemic therapy, elastic stockings and bandages are used as local treatment for BLE. Because elastic bandages have appropriate elasticity and compressive force, they are suitable for immobilizing affected areas and applying pressure. Similarly, elastic stockings resist slippage and apply a constant amount of pressure. However, because they continuously apply pressure to the lower extremities, care must be taken to avoid skin problems and complications.
The purpose of compressive therapy is twofold. One goal is to improve the patient’s subjective symptoms and prevent bruising, injury, and infection while waiting for the patient to respond to systemic therapy. The second purpose is to improve venous blood flow by compressing the perivenous tissues of the lower extremities, thus reducing edema and preventing thrombus formation.
In the authors’ hospital, some patients with lung cancer developed BLE. These patients were treated with elastic stockings and bandages in addition to systemic anticancer therapy, and some patients benefited from this therapy.
CASE SERIES PatientsThe authors searched their hospital database for all patients with lung cancer who were treated from April 2013 to March 2022 who developed BLE. The authors defined BLE as symptomatic, bilateral, and marked edema of the lower legs. Symptoms of BLE included discomfort, sensory impairment, and difficulty dressing and undressing. There were no patient exclusion criteria for patient backgrounds such as comorbidities, histologic types of lung cancer, treatment of lung cancer, and treatment of edema. However, dermatologists and cardiologists evaluated patients to determine their eligibility for compression therapy before beginning treatment. Patients who developed leg edema also received consultation with nephrologists to determine if the cause of the edema was renal disease.
ProcedureEach patient underwent a physical examination before starting compression therapy. The physician confirmed the absence of skin ulceration and cellulitis and performed bilateral palpation of the dorsal and posterior tibial arteries. Nurses and dermatologists carefully checked for skin infection at each patient visit both before and during treatment. The authors consulted dermatologists regarding each patient and confirmed that the patient had no dermatologic conditions that would interfere with the implementation of this bandage therapy. Under the direction of the cardiologist, patients underwent lower extremity ultrasonography to confirm that there was no stenosis or thrombosis in the arteries and veins of the lower extremities. Cardiologists also evaluated the low risk of heart failure with this bandage therapy for each patient.
Patients received elastic stockings (Gunze Leg Science) and elastic bandages (Elascot; Alcare) to wear. Under the guidance of nurses and their caregivers, the patients wore elastic stockings up to their knees and, if necessary, elastic bandages from the knees to the thighs. Bandages were applied simultaneously on both lower extremities. At the beginning of compression therapy, the nurse confirmed that the pressure on the upper part of the inner ankle and the calf was approximately 20 mm Hg.14,15 In addition, nurses and the dermatologist in charge educated the patient and his/her caregivers (usually family members) on precautions to take when wearing elastic stockings and the importance of appropriate pressure. Patients were informed that there were no minimum or maximum hours per day that the bandage therapy should be carried out. In the event of patient distress, it was permissible to loosen the bandage and provide a rest period.
At least once per week, a nurse and/or dermatologist physically examined each patient by inspection and palpation to determine whether the BLE had exacerbated or improved and if any complications had developed. If there were any inadequacies in the bandage (eg, too loose, too tight, slippage), the nurses implemented appropriate remedial measures with the patient and caregivers. If the patient showed improvement in BLE and did not experience distress, bandage therapy was continued for up to 2 months. Bandage therapy was terminated if the patient requested to discontinue it because of distress or other reasons, or if it was medically determined to be adversely affecting the patient’s body.
The authors evaluated the effect of the compression therapy based on the improvement of subjective symptoms and objective findings at 2 months after the start of compression therapy or the point at which therapy was discontinued. Objectively, compression therapy was judged to be effective if the circumference of any of the lower leg, ankle joint, or back of the foot had decreased by 2 cm or more.
EthicsThis study was conducted in accordance with the Declaration of Helsinki, and it was approved by the institutional review board of the authors’ institution. Each participant provided written informed consent to publish the case details and associated images.
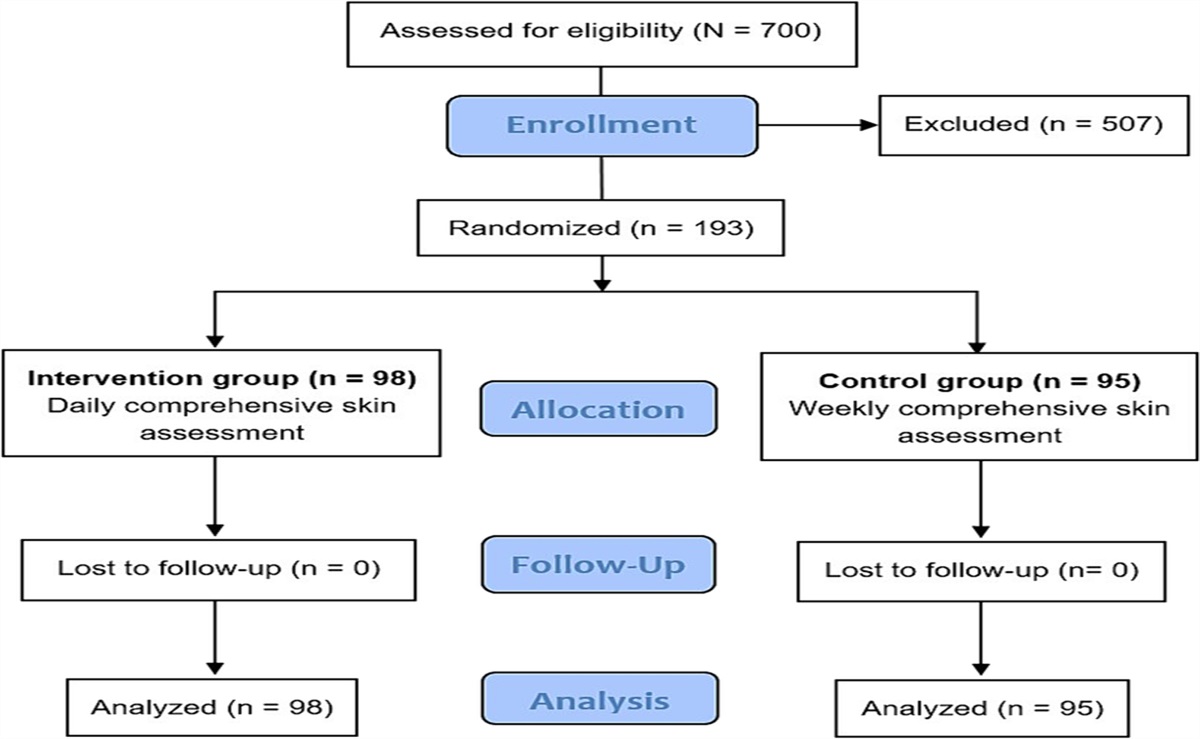
OutcomesThe authors included all seven consecutive patients with lung cancer (four men, three women) who developed BLE during the study period (Figure 1). Patient characteristics are shown in Table 1. The median patient age was 68 years (range, 41-85 years). Six patients had lung adenocarcinoma, and one had large cell neuroendocrine carcinoma. Six patients developed BLE when systemic chemotherapy failed, and one patient experienced BLE during the follow-up period after lung cancer resection. All patients received protein-based semidigestive nutrition supplements, and four patients received a selective oral ghrelin-like agonist, anamorelin.16 No patients experienced venous thrombosis.
 Figure 1.:
Figure 1.: FLOWCHART OF PATIENT SELECTION
Table 1. - PATIENT CHARACTERISTICS Case No. Age, y Sex Pathology Driver Gene Comorbidity First-Line Therapy for Lung Cancer Anticancer Therapy and Onset of BLE Lung Cancer Control Status VTE of the Lower Extremities 1 68 Female Adenocarcinoma EGFR None EGFR-TKI PD status (RECIST) after TKIs and other therapies Not controlled Not detected 2 41 Male Adenocarcinoma ALK None ALK-TKI PD status (RECIST) after TKIs and other therapies Not controlled Not detected 3 69 Female Adenocarcinoma EGFR None EGFR-TKI PD status (RECIST) after TKIs and other therapies Not controlled Not detected 4 72 Female Adenocarcinoma None None ICI During ICI treatment Controlled Not detected 5 71 Male Adenocarcinoma None IRAE colitis Chemotherapy During ICI treatment Controlled Not detected 6 48 Male LCNEC None Spinal invasion Chemoradiotherapy During supportive care Not controlled Not detected 7 71 Male Adenocarcinoma None IPF Surgery During postoperative follow-up Controlled Not detectedAbbreviations: ALK, anaplastic lymphoma kinase; BLE, bilateral leg edema, EFGR, epidermal growth factor receptor; ICI, immune checkpoint inhibitor; IPF, idiopathic pulmonary fibrosis, LCNEC, large-cell neuroendocrine carcinoma; PD, progressive disease; RECIST, Response Evaluation Criteria in Solid Tumors; TKI, tyrosine kinase inhibitor; VTE, venous thrombosis.
Three patients had driver genes: two patients had epidermal growth factor receptor, and one patient had anaplastic lymphoma kinase rearranged mutation. All three of these patients (patients 1-3) developed BLE when both first-line tyrosine kinase inhibitor (TKI) therapy and other therapies became progressive disease, as determined according to the RECIST (Response Evaluation Criteria in Solid Tumors) guideline, version 1.1.16 Two of these patients had metastases to the abdominal lymph nodes. One patient received anamorelin. Although all three of these patients received compression therapy for 1 month or longer, none showed improvement in BLE (Figure 2).
 Figure 2.:
Figure 2.: ULTRASONOGRAPHIC FINDINGS OF LOWER EXTREMITIES IN TWO CASESUltrasonographic findings of (A) right lower extremity and (B) left lower extremity of patient 1. There was no deformation or stenosis in the veins. Veins in both lower extremities had good mobility during compression (left, before compression; right, at the time of compression). Ultrasonographic findings of femoral artery and vein in the (C) right thigh and (D) left thigh of patient 3. No deformation or stenosis was found in the arteries or veins. Good mobility was confirmed in the veins during compression (left, before compression; right, at the time of compression).
Among the seven patients, four patients (patients 4-7) had no driver gene. Of these four patients, three developed BLE during systemic chemotherapy (patients 4 and 5 developed BLE during ICI treatment), and one developed BLE during postoperative follow-up (patient 7). Three of these patients received anamorelin, but two patients (patients 4 and 7) discontinued its use because of dizziness. Further, patients 4, 5, and 7 did not continue taking the nutrition supplement after a week because they disliked the taste. In patients 4 and 5, ICI was discontinued, and corticosteroids were administered, but BLE did not improve. However, after bandage therapy was started, BLE was greatly reduced in these patients within 2 months. Thereafter, bandage therapy was terminated, and these patients experienced no re-exacerbation of BLE over the next few months. Patient 6 had metastases to the thoracic and lumbar spine as well as metastatic lesions in the spinal cord. This patient failed to respond to any treatment, became paralyzed in the lower body, and died of lung cancer. Table 2 shows courses of treatment and therapeutic effects. None of the patients discontinued the bandage therapy due to adverse effects.
Table 2. - TREATMENT RESULTS Case No. Albumin, g/dL Precise Timing of Edema Onset Nutrition Supplement Anamorelin Diuretics Corticosteroid Duration of Compression Therapy, mo Edema Control Control Period, mo 1 2.7 After the fourth-line anticancer therapy Administered Not administered Administered Not administered 1 Not controlled – 2 3.1 After the third-line anticancer therapy Administered Not administered Administered Not administered 1 Not controlled – 3 1.9 After the fourth-line anticancer therapy Administered Administered Not administered Not administered 2 Not controlled – 4 2.7 After the first-line anticancer therapy Administered Administered Not administered Administered 2 Controlled 6+ 5 2.0 After the fifth-line anticancer therapy Administered Administered Not administered Administered 2 Controlled 6+ 6 2.5 After the fifth-line anticancer therapy Administered Not administered Not administered Administered 2 Not controlled – 7 2.7 Postoperative follow-up Administered Administered Administered Not administered 2 Controlled 5+The authors used a Mann-Whitney U test to compare serum albumin levels at the onset of BLE to determine if nutrition status varied between patients who were and those who were not driver-gene positive. There was no between-group difference in albumin level (P = .71).
DISCUSSIONAmong the seven patients, the three who were driver-gene positive (patients 1-3) experienced no improvement in BLE. However, three of the four patients who were driver-gene negative (patients 4, 5, and 7) had improvement in BLE with compression therapy with elastic stockings and bandages. These improvements in BLE were achieved with multiple therapies, including systemic therapies for cancer, not with bandage therapy alone. However, in some patients whose BLE was not controlled by dietary supplements, anamorelin,17 or corticosteroids for IRAE, compression therapy improved BLE.
Not surprisingly, the outcome of treatment for lung cancer itself had a significant impact on the treatment of BLE. Ideally, if the first-line TKI becomes resistant, the next treatment would be effective; unfortunately, the efficacy of later-line therapeutic agents is currently inferior to that of TKIs. In the present case series, it was interesting to confirm the improvement of BLE that developed in patients during ICI treatment. The concurrent use of an appetite-promoting drug, a nutrition supplement, and corticosteroids in the case of IRAEs was important.
None of the patients discontinued the bandage therapy because of adverse effects. The authors surmise that allowing the patients to remove their elastic stockings and loosen the bandages when they felt pain improved adherence.
BLE TreatmentBilateral leg edema has a variety of etiologies.18,19 Serious BLE reduces patient quality of life and impedes daily behavior. Thus, this symptom should be improved if possible. Edema above the knee is less common than BLE below the knee but is not rare in general. The use of stockings below the knee and bandages above the knee is common. Other alternatives include Tubigrip/Elastogrip (Mölnlycke Health Care) and EdemaWear (Compression Dynamics).20
When treating BLE associated with cancer, it is important to treat the cancer itself, which is the basis of the pathologic condition. Further, if the patient presents with thromboembolism, inhibition of lymph flow, loss of appetite, or malnutrition associated with the cancer, treatment for these symptoms is also indicated. In addition to these treatments, providers may also give diuretics to patients with cancer who develop BLE. Diuretics are unlikely to be effective in patients with hypoalbuminemia and malnutrition, and providers should consider the risk of thromboembolism due to abnormalities in coagulation and fibrinolysis in patients with cancer.21
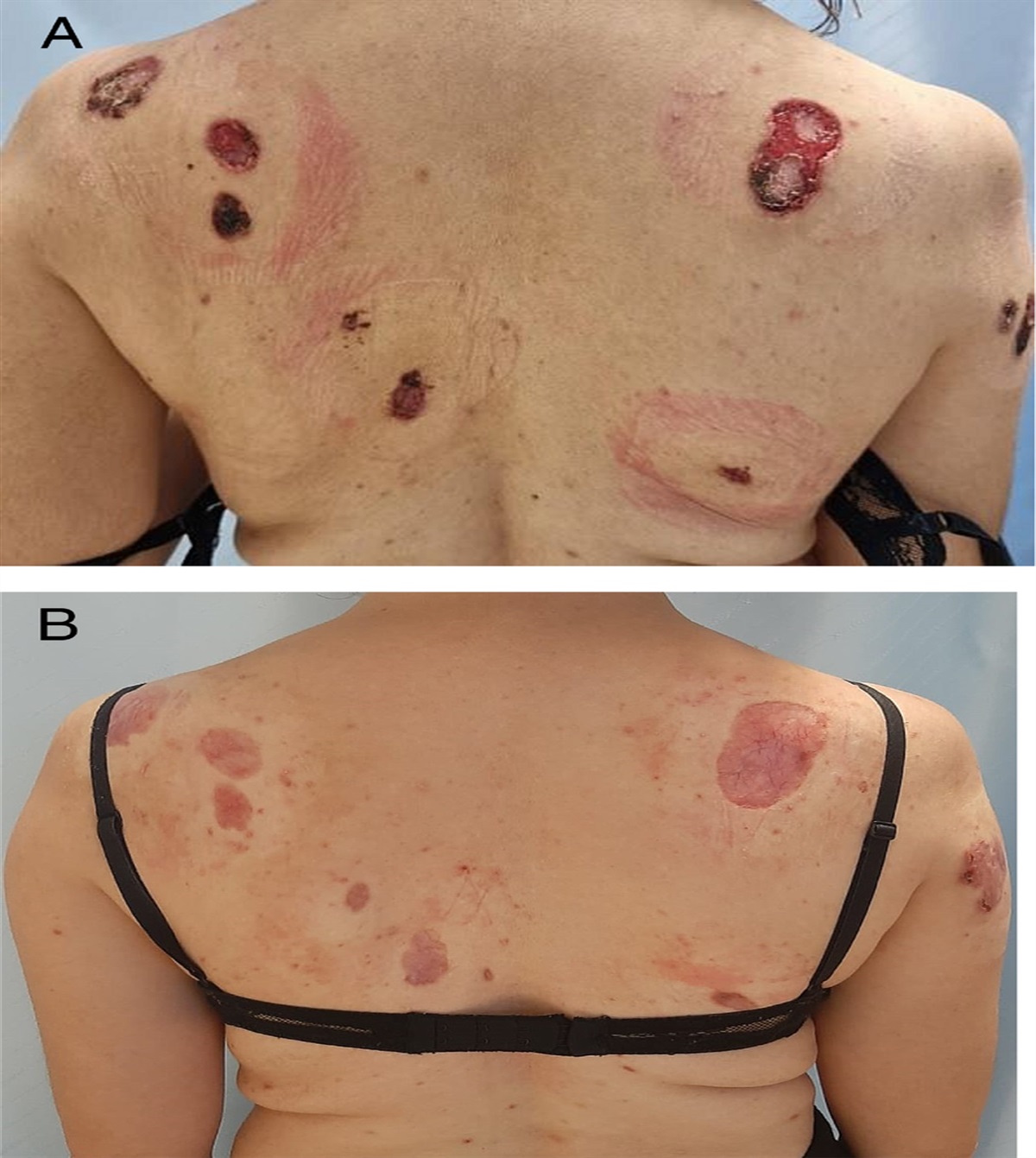
Rather than relying on the administration of diuretics, providers should aim to take a nonpharmacologic approach when appropriate. In patients with urologic, gynecologic, and gastrointestinal cancers, intraperitoneal lymph nodes, spinal cord metastasis, and iliac and leg vein thrombosis can cause BLE.22–25 In recent years, clinicians have used ICIs to treat patients with these cancers as well as patients with lung cancer, and the possibility of long-term survival has been documented.8 With ICI therapy, IRAEs can occur in organs throughout the body and require appropriate treatment. In the present care series, one patient (patient 5) had diarrhea associated with an endoscopically confirmed IRAE and enteritis, followed by BLE (Figure 3). For this patient, BLE was controlled by a combination of corticosteroid and compression therapy. The experience of treating this patient can provide suggestions for BLE treatment in other patients with cancer.
 Figure 3.:
Figure 3.: BILATERAL LEG EDEMAPatient 5 had thickening, luster, swelling, and mild redness in both lower extremities due to swelling. There was no warmth on palpation.
In recent years, several studies have reported on compression therapy for BLE in patients with cancer.26–28 Tennison et al26 showed the usefulness of multicomponent compression, reporting on the outcomes of treatment of seven patients with various cancers. In patients with urologic or gynecologic cancers, local anatomic factors impacted the therapeutic effects of compression therapy on BLE. Of note, it may be difficult to ensure that bandages maintain a particular pressure unless the person applying the bandage is a medical professional. Further, two of seven patients in that case series had shortness of breath and could not continue treatment.26
In the present case series, nurses checked the bandage for appropriate pressure at the beginning of treatment and confirmed that the bandage was properly applied each time the patient visited the hospital. It was usually the patient or family members who applied and removed the elastic stocking and bandages, rather than medical staff.
LimitationsThis case series included patients with various backgrounds, and implementation and evaluation methods were not strictly determined. Although ankle-brachial pressure index and audible handheld Doppler with a biphasic or triphasic wave are considered the best methods for setting the appropriate pressure,29,30 the authors measured patients’ BP. Transcutaneous oximetry can also be used to assess arterial blood flow in combination with or instead of ankle-brachial pressure index.
Applying compression to both legs simultaneously could cause or aggravate congestive heart failure. Urbanek et al31 reported that it might be best to apply compression to one leg first for 24 hours and then the other if it does not result in fluid overload in patients with heart failure. The authors performed bandage therapy under the direction of cardiologists, and no patients developed heart failure. In addition, the authors have never encountered BLE that developed long after the end of ICI treatment, so treatment outcome in such cases is unknown.
CONCLUSIONSIn this retrospective case series, the authors reported outcomes of compression therapy using elastic stockings and bandages for BLE in patients with lung cancer. One beneficial aspect of compression therapy was that it could be performed by families and did not require intervention by professional medical staff or the purchase of expensive items. It showed positive effects in some patients, particularly those who were driver-gene negative, in combination with the lung cancer treatments. These results provide suggestions for the medical care of similar patients in the future. This case series also highlights the importance of collaboration among many medical professionals. In many case study scenarios such as this, more emphasis is needed on the role of nurses and other medical professionals who equally complement patient medical care.
REFERENCES 1. Powell AA, Armstrong MA. Peripheral edema. Am Fam Physician 1997;55:1721–6. 2. Ciocon JO, Fernandez BB, Ciocon DG. Leg edema: clinical clues to the differential diagnosis. Geriatrics 1993;48:34–40. 3. Von Meyenfeldt M. Cancer-associated malnutrition: an introduction. Eur J Oncol Nurs 2005;9:S35–8. 4. Dahele M, Fearon KC. Research methodology: cancer cachexia syndrome. Palliat Med 2004;18:409–17. 5. Shijubou N, Sumi T, Keira Y, et al. Pseudocirrhosis due to liver metastasis from lung adenocarcinoma. Thorac Cancer 2021;12:2407–10. 6. Chang IH, Ha MS, Chi BH, Kown YW, Lee SJ. Warfarin-induced penile necrosis in a patient with heparin-induced thrombocytopenia. J Korean Med Sci 2010;25:1390–3. 7. Guo Y, Cao R, Zhang X, et al. Recent progress in rare oncogenic drivers and targeted therapy for non-small cell lung cancer. Onco Targets Ther 2019;12:10343–60. 8. Filleron T, Bachelier M, Mazieres J, et al. Assessment of treatment effects and long-term benefits in immune checkpoint inhibitor trials using the flexible parametric cure model: a systematic review. JAMA Netw Open 2021;4:e2139573. 9. Capaccione KM, Valiplackal JP, Huang A, et al. Checkpoint inhibitor immune-related adverse events: a multimodality pictorial review. Acad Radiol 2022:S1076-6332(22)00171–4. 10. Moriyama S, Fukata M, Tatsumoto R, Kono M. Refractory constrictive pericarditis caused by an immune checkpoint inhibitor properly managed with infliximab: a case report. Eur Heart J Case Rep 2021;5:ytab002. 11. Chatterjee A, Bivas BK, Gehani A, Sen S. Pembrolizumab-induced large duct cholangiopathy: diagnosis and follow up imaging. J Postgrad Med 2021;67:43–5. 12. Bourcier L, St-Hilaire È, LeBlanc M, Picard L. Complete reversibility of pembrolizumab-induced eosinophilic fasciitis without corticosteroids: a case report. SAGE Open Med Case Rep 2021;9:2050313X211025111. 13. Tjarks BJ, Kerkvliet AM, Jassim AD, Bleeker JS. Scleroderma-like skin changes induced by checkpoint inhibitor therapy. J Cutan Pathol 2018;45:615–8. 14. Fife CE, Davey S, Maus EA, Guilliod R, Mayrovitz HN. A randomized controlled trial comparing two types of pneumatic compression for breast cancer-related lymphedema treatment in the home. Support Care Cancer 2012;20:3279–86. 15. Gianesini S, Tessari M, Menegatti E, et al. Comparison between the effects of 18- and 23-mmHg elastic stockings on leg volume and fatigue in golfers. Int Angiol 2017;36:129–35. 16. Eisenhauer EA, Therasse P, Bogaerts J, et al. New Response Evaluation Criteria in Solid Tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: 228–47. 17. Fonseca GWPD, von Haehling S. An overview of anamorelin as a treatment option for cancer-associated anorexia and cachexia. Expert Opin Pharmacother 2021;22:889–95. 18. Scherer K, Khilnani N. Evaluation and management of patients with leg swelling: therapeutic options for venous disease and lymphedema. Semin Intervent Radiol 2021;38:189–93. 19. Ely JW, Osheroff JA, Chambliss ML, Ebell MH. Approach to leg edema of unclear etiology. J Am Board Fam Med 2006;19:148–60. 20. Sibbald RG, Elliott JA, Coutts P, Persaud-Jaimangal R. Evaluation of longitudinal and tubular compression treatment for lower limb edema. Adv Skin Wound Care 2020;33:643–9. 21. Fujieda K, Nozue A, Watanabe A, et al. Malignant tumor is the greatest risk factor for pulmonary embolism in hospitalized patients: a single-center study. Thromb J 2021;19:77. 22. Abu-Rustum NR, Alektiar K, Iasonos A, et al. The incidence of symptomatic lower-extremity lymphedema following treatment of uterine corpus malignancies: a 12-year experience at Memorial Sloan-Kettering Cancer Center. Gynecol Oncol 2006;103:714–8. 23. Plimack ER, Geynisman DM. Targeted therapy for metastatic urothelial cancer: a work in progress. J Clin Oncol 2016;34:2088–92. 24. Patel SA. The inferior vena cava (IVC) syndrome as the initial manifestation of newly diagnosed gastric adenocarcinoma: a case report. J Med Case Rep 2015;9:204. 25. Shayestehpour M, Ehsani M, Dadkhah D, Zamani B. A case of antiphospholipid syndrome following gastric signet ring cell adenocarcinoma. Am J Case Rep 2020;21:e919037. 26. Tennison JM, Narayanan S, Cummings R, Bruera E. Multicomponent compression bandaging for refractory bilateral lower extremity edema of multifactorial origin in cancer patients: a retrospective case series. J Pain Symptom Manage 2019; 58:e5–8. 27. Tennison JM, Fu JB, Bruera E. Improvement of refractory peripheral edema with multilayered compression bandaging: a case report. Phys Ther 2018;98:763–6. 28. Gradalski T. Diuretics combined with compression in resistant limb edema of advanced disease—a case series report. J Pain Symptom Manage 2018;55:1179–83. 29. Elwell R, Sneddon M. Introducing the British Lymphology Society position paper on ankle brachial pressure index. Br J Community Nurs 2019;24:206–11. 30. Chang CC, Wong CH, Wei FC. Free-style free flap. Injury 2008;3(93):S57–61. 31. Urbanek T, Jus´ko M, Kuczmik WB. Compression therapy for leg oedema in patients with heart failure. ESC Heart Fail 2020;7:2012–20.
Comments (0)