
Remember me




How to interpret these recommendations
Prognosis: how does the biomarker influence risk? Risk prediction: can the biomarker classify patients into various levels of risk? Biomarker-enhanced management: can management strategies based on biomarker surveillance improve outcomes? Prognostic factor studies measure the variation in incidence of the outcome over time in a population of interestFor predictive models:
We are very confident that the estimated improvement in model performance (discrimination/calibration) resulting from consideration of the prognostic/risk factor
lies close to that of the estimate.
For predictive models:
We are moderately confident that the estimated improvement in model performance (discrimination/calibration) resulting from the consideration of the prognostic/risk factor is likely to be close to the estimate, but there is a possibility that it is substantially different.
For predictive models:
Our certainty in the estimate is limited - the estimated improvement in model performance (discrimination/calibration) resulting from the consideration of the prognostic/risk factor may be substantially different from the estimate.
For predictive models:
We have very little certainty in the estimate - the estimated improvement in model performance (discrimination/calibration) resulting from the consideration of the prognostic/risk factor is likely to be substantially different from the estimate.
In recent years, there has been increasing focus on the use of cardiac biomarkers in non-cardiac surgery patients. Biomarkers may be used in this setting with three separate aims: first, for prognosis, i.e. to establish how elevated biomarker concentrations influence the risk of specific outcomes. The associations between elevated biomarkers and risk increase are typically expressed in adjusted odds or hazard ratios. Second, for risk prediction, i.e. how much the biomarker contributes to the differentiation of patients with elevated risk. Within the context of cardiovascular risk prediction the incremental performance of the biomarker when added to clinical risk scores is of interest. Common approaches to quantify improved prediction are differences in Brier Score, c-statistics, net reclassification indices, integrated discrimination improvement (IDI), while the net benefit allows clinicians to make a judgement on the usefulness of the test taking into account the relative clinical cost of a false positive compared with a false negative diagnosis and disease prevalence.1,2 Third, for “biomarker-enhanced management”, i.e. the adoption of perioperative interventions in patients flagged as ‘at risk’ by the biomarker(s) to improve outcome. Typically, improved outcome would be demonstrated in relative (and absolute) risk reduction in randomized clinical trials.
The optimal perioperative cardiac biomarker would be one that can be easily and accurately measured, that allows identification of specific pathogenic processes at an early stage, thus allowing targeted intervention tailored to estimated risk. The most commonly evaluated biomarkers in non-cardiac surgery are the cardiac troponins (cTnI and cTnT) and B-type natriuretic peptides (which include BNP and NT-proBNP). Large, observational studies have demonstrated increased cardiac troponin (cTn) levels as prognostic factors in non-cardiac surgery patients. These studies have established an association between increased cTn and cardiovascular and non-cardiovascular complications, poor short- and long-term cardiovascular outcomes and mortality.3–58 The contribution of cTn to improved/incremental prediction is less well explored.3,10,15,16,18,24,26–32,40–44,55,58 Current literature suggests that myocardial injury occurring in the perioperative period is multifactorial and patterns that allow identification of specific pathogenesis are not established. As such, targeted treatment of the entity “myocardial injury” will remain difficult in spite of its potential value as early indicator of adverse outcomes.
Increased preoperative B-type NPs appear also to have prognostic value for mortality and poor cardiovascular outcomes. However, perioperative changes and postoperative B-type NPs for prognosis and for risk prediction are less well studied.8,9,12–14,59–108 Current European guidelines109,110 provide guidance on the use of cardiac biomarkers that differ in terms of strength of the recommendation and on the population to be submitted for cardiac biomarker evaluation.
The 2018 European Society of Anaesthesiology and Intensive Care (ESAIC) guidelines109 on pre-operative evaluation of adults undergoing elective non-cardiac surgery suggest considering assessment of cTn in high-risk patients, both before and 48 to 72 h after major surgery (2B = weak recommendation, moderate quality evidence). Preoperatively, the guideline suggested considering high-sensitivity cTn measurement in patients at risk of coronary artery disease and in patients undergoing major surgery (2C = weak recommendation, low quality evidence). Further, the guideline recommends B-type NP measurement in intermediate and high-risk patients undergoing vascular or major thoracic surgery (1C = strong recommendation, low quality evidence) and suggests considering B-type NP measurement in high-risk patients undergoing major general or orthopaedic surgery (2C = weak recommendation, low quality evidence). To define baseline clinical risk, the Revised Cardiac Risk Index is recommended, i.e. the consideration of the following risk factors: coronary artery disease, history of congestive heart failure, history of cerebrovascular events, insulin-dependent diabetes mellitus, and renal dysfunction.
The 2022 European Society of Cardiology (ESC) guidelines on cardiovascular risk assessment and management of patients undergoing non-cardiac surgery110 issue a strong recommendation for awareness of perioperative myocardial injury, including surveillance using cTn with a view of identifying underlying pathophysiology and defining treatment. The preoperative assessment algorithm includes a strong recommendation for preoperative cTn (I) and to consider preoperative B-type NP measurement (IIa) in patients with cardiovascular risk factors or >65 years of age planned for intermediate or high-risk procedures. Surveillance with high-sensitivity cTn should extend to 24 and 48 h after surgery in this group of patients (I). In patients aged 45–65 years without signs, symptoms, or history of cardiovascular disease (CVD), these guidelines suggest considering cardiac biomarkers before high-risk non-cardiac surgery (IIa). In summary, the 2022 ESC recommendations on the routine use of cardiac biomarkers are stronger compared to those from the 2018 European Society of Anaesthesiology Task Force in Preoperative Evaluation and refer to a much broader population.
Both the ESA 2018 preoperative evaluation guidelines and 2022 ESC guidelines on cardiovascular risk assessment and management do not, or only inconsistently, differentiate between cardiac biomarkers as prognostic factors vs. its use of as a risk prediction tool. This fact and the differing recommendations described above make it difficult for clinicians to reconcile the utility of cardiac biomarkers.
The aim of this focused guideline is to provide updated guidance regarding the pre- and postoperative use of cardiac troponin and B-type natriuretic peptide in adult non-cardiac surgery patients using Grading of Recommendations Assessment Development and Evaluation (GRADE) methodology.111 The use of biomarkers for the diagnosis of acute myocardial injury, acute myocardial infarction and acute heart failure is well established and are not encompassed by the present guidelines. Specifically, the evidence on cardiac biomarkers as prognostic factors, as tools for (improved) risk prediction, and on biomarker-enhanced management strategies was appraised separately and the panel systematically evaluated the balance of biomarker measurement in terms of desirable and undesirable effects including clinical outcomes, resource use, health inequality, stakeholder acceptance, and implementation.
Methods OrganisationThis guideline was prepared on behalf of the ESAIC and in accordance to the framework of the ESAIC guidelines committee using GRADE methodology. The steering committee (SC) of the focused guideline committee led the guideline process. In particular, it was responsible for all methodological aspects with support from the methodologist appointed by ESAIC and for selection and invitation of the panel members. The SC aimed for diversity in the panel, including gender, age, specialty and country of practice. A list of all team members involved in the development process may be found in the Supplemental Digital Content (SDC) 1, https://links.lww.com/EJA/A841.
The panel comprised of 18 members including content experts, academic physicians, practicing clinicians, a patient representative and a methodologist. The content experts included representatives from Cardiac, Surgical, Anaesthesia, Perioperative medicine, Intensive Care and Laboratory Medicine specialties with full voting rights. The patient representative actively participated in the process and provided valuable insights regarding outcome selection and prioritisation, values and preferences.
Conflicts of interestTen panel members reported conflicts of interest (SDC2, https://links.lww.com/EJA/A842).
ESAIC provided administrative support for surveys, the Delphi process and coordination of meetings and had no financial conflicts of interest related to the guidelines. Panel members were not reimbursed for their work by ESAIC or a third-party.
ScopeThis guideline applies to the pre-, post, or combined pre- and postoperative measurement of cTn and of B-type NPs for prognosis, risk prediction, or for biomarker-enhanced management in patients ≥18 years undergoing non-cardiac surgery, except for transplantation (other than renal) and obstetric surgery. Due to limited evidence in the non-cardiac surgery setting for other cardiac biomarkers, these were not considered for these guidelines.
The target users are perioperative clinicians (e.g. anaesthetists, surgeons, cardiologists, perioperative and critical care physicians), allied health professionals (e.g. nurses, nurse-practitioners, assistant nurses and physiotherapists), patients, patient representatives and policymakers.
The panel used the Population, Intervention/Exposure, Comparator, Outcome (PICO) model to formulate research questions. We reported the guidelines following the Appraisal of Guidelines for REsearch and Evaluation (AGREE) II reporting checklist112 (SDC3, https://links.lww.com/EJA/A843).
The specific research questions were:
(1) Do preoperative, postoperative or changes (postoperative minus preoperative) in cTn provide independent prognostic information for short- and long-term clinical outcomes? (2) Among adult patients undergoing non-cardiac surgery (3) Do preoperative, postoperative or changes (postoperative minus preoperative) in cTn provide incremental value for prediction of short- and long-term clinical outcomes when added to a baseline model (e.g. clinical risk scores)? (4) Do preoperative, postoperative or changes (postoperative minus preoperative) in B-type NP measurement provide independent prognostic information for short- and long-term clinical outcomes? (5) Do preoperative, postoperative or changes (postoperative minus preoperative) in B-type NP measurement provide incremental value for prediction of short- and long-term clinical outcomes when added to a baseline model (e.g. clinical risk scores)? (6) Does a biomarker-enhanced management strategy improve short- and long-term clinical outcomes? Literature searchA literature search (SDC4, https://links.lww.com/EJA/A844 Literature Search) was conducted from 1 January 1946 to 16 March 2021, with an update on 3 February 2022. The search was conducted by an independent Cochrane Information Specialist in Epistemonikos, Medline and EMBASE databases, and exported to a Rayyan© database where eligibility was assessed by two independent assessors (G.L.B., M.S.C. or B.B.P.).
The following studies were excluded:
(1) Experimental studies (animal or in-vitro) and veterinary clinical studies (2) Case reports, narrative reviews, editorials (3) Children (4) Adults with congenital heart disease (5) Obstetric surgery (6) Transplantation (liver, lung, heart) except renal (7) Percutaneous cardiac interventions, any cardiac surgery/procedure (8) Non full text articles, case reports, letters, brief reports.Disagreement was solved by discussion with involvement of a third assessor.
OutcomesThe literature search identified a large number of heterogeneous clinical outcomes. Therefore, a Delphi process was conducted to classify the level of importance of the various outcomes according to GRADE. Panel members rated the importance of the outcomes on a on a scale from 1 to 9 with low numbers reflecting limited importance and high numbers reflecting critical importance for perioperative decision making. The online survey was conducted using LimeSurvey (www.limesurvey.org) and SurveyMonkey (www.surveymonkey.com). Outcomes rated 7 to 9 and 4 to 6 by ≥70% of panel members were included in a second Delphi round. Only outcomes with a final score of 7 to 9 in >70% of responses were considered critical and included for data extraction. There was no attrition in the two Delphi rounds. None of the Delphi-determined outcomes included patient relevant outcome measures (PROMs). We then sought guidance from the patient representative regarding the validity and importance of the outcomes. Following this input and after an extensive discussion during a hybrid meeting at Euroanaesthesia 2022, all panelists voted in favour of the inclusion of two PROMs (quality of life and disability).
The following 12 critical outcomes were considered in appraisals of overall quality of evidence and for moving from evidence to recommendation:
(1) All-cause mortality up to 30 days after surgery (2) All-cause mortality up to 1 year after surgery (3) Cardiac mortality up to 30 days after surgery (4) Death or myocardial infarction up to 30 days after surgery (5) Death or myocardial infarction up to 1 year after surgery (6) Major adverse cardiac events up to 30 days after surgery (7) Major adverse cardiac events up to 1 year after surgery (8) Cardiac complications of any severity up to 30 days after surgery (9) Myocardial injury up to 30 days after surgery (detected by systematic troponin screening; not fulfilling 4th universal definition of myocardial infarction) (10) Complications (cardiac and non-cardiac) up to 30 days after surgery (11) Short-term disability using predefined scale/scoring system (collected up to 90 days after surgery) (12) Short-term Quality of Life (collected up to 90 days after surgery). Data extraction and risk of bias assessmentData were extracted into a predefined template and included the following information on methodology: design, type of non-cardiac surgery procedures, biomarker assay and its cutoffs, timing of sampling, approach used in the study to define biomarker elevation and relevant cut-offs, primary and secondary outcomes, variables used for risk adjustment and clinical risk score used. Study results extracted included sample size, overall number of events and in patients with and without elevated biomarker, the unadjusted and adjusted odds and hazard ratios for prognosis, and measures for predictive performance (e.g. Brier score, c-statistics, net reclassification improvement, IDI). Data was extracted by trained extractors.
Risk of bias was assessed using the Newcastle-Ottawa Score.
Data synthesis and drafting of recommendationsData synthesis was conducted according to GRADE. Certainty of evidence determined with consideration of risk of bias, inconsistency, indirectness, imprecision and publication bias. Based on these considerations, certainty of evidence was classified as high, moderate, low, very low. Only adjusted measures of association were considered for summarizing evidence for prognosis.
Summary of evidence tables following the GRADE format were presented and discussed at a hybrid meeting at Euroanaesthesia 2022. We used the GRADE framework and corresponding templates to move from evidence to recommendation.
In making recommendations, the panel considered the overall certainty of evidence across all outcomes, the priority of the problem, whether there would be important uncertainty in how people would value the main outcomes, the size of the desired anticipated effects, whether the desirable anticipated effects are large compared to undesirable effects, the required resources, possible incremental cost compared to net benefits, impact on health inequalities, feasibility and acceptance among key stakeholders including members from cardiology, surgery and laboratory medicine specialities, as well a patient representative. A draft version of the recommendations was circulated to all panel members via E-Mail and discussed at an on-line meeting. Following this, the recommendations were revised and expanded with clinical practice statements for questions where the panel considered that evidence was too limited to issue a formal recommendation but where guidance for clinicians was deemed important. Finally, all panelists were asked to vote (agree, disagree, I do not know) online on each recommendation and clinical practice statement separately. All 18 panel members voted in the first round. After further discussion in an attempt to achieve consensus, some recommendations and clinical practice statements were re-worded. A second round of voting was conducted with attrition of 3 panel members i.e. 16 panel members finally voted. A third round of voting with 16 panel members was conducted to achieve consensus regarding the MANAGE trial113. All voting was anonymous and conducted on-line. Consensus was defined a priori by agreement of ≥70% of panel members.
Recommendations were classified as strong (1) and weak (2).
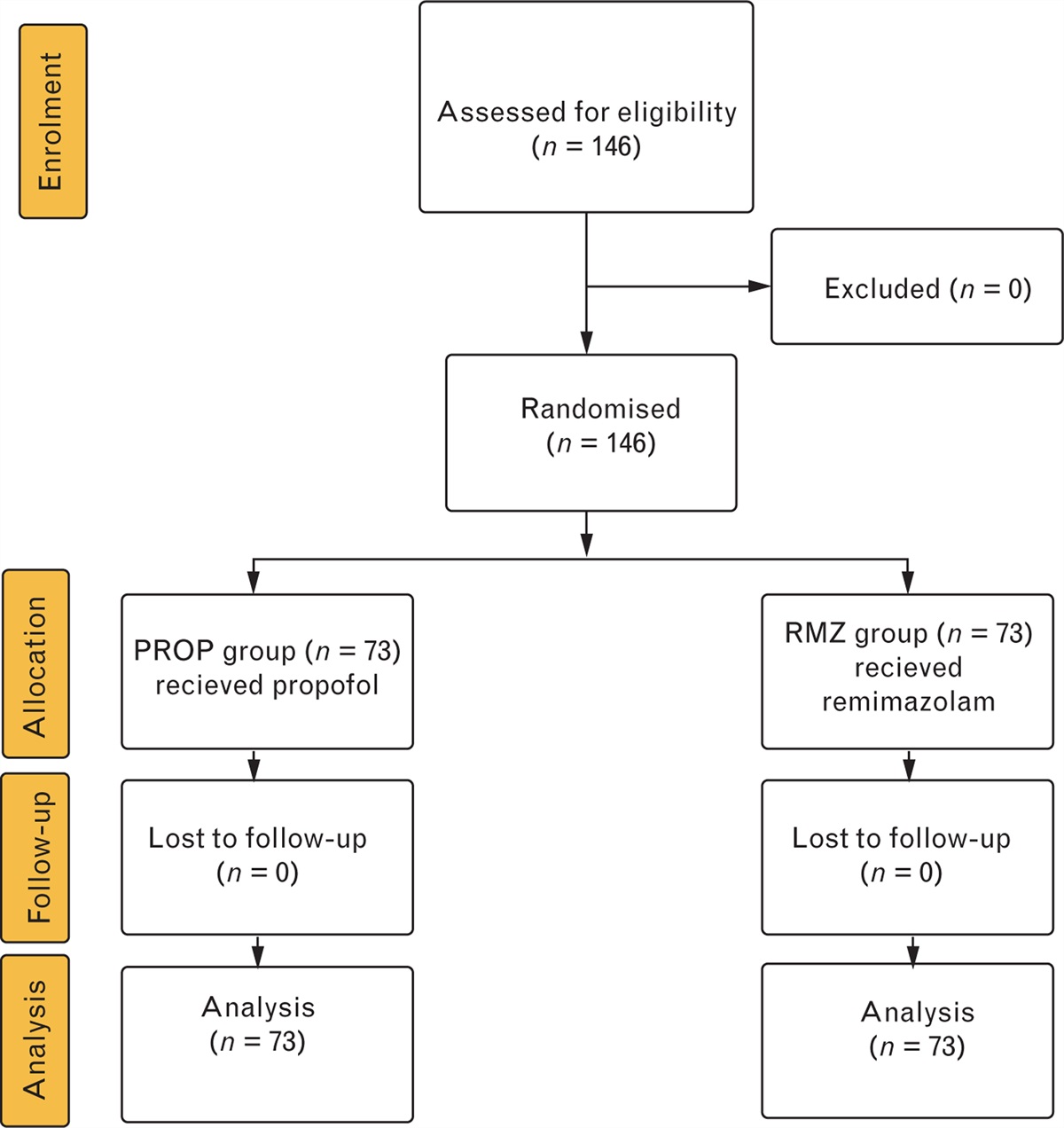
Results Research evidenceA PRISMA flowchart of the retrieved and assessed papers is shown in Figure 1.
 Fig. 1:
Fig. 1: PRISMA flowchart of retrieved and assessed papers.
Summaries of evidence used to inform the evidence to decision framework are reported in Tables 1–5 for preoperative (stand-alone) cTns, combined pre- and postoperative cTns, postoperative cTns, preoperative B-type NPs and postoperative B-type NPs. The data on prognostic and predictive values of postoperative B-type NP elevation was extracted from an individual patient-level meta-analysis that included elevated preoperative B-type NP in the baseline model.105 The authors primarily presented their results for the addition of elevated postoperative B-type NP to the baseline model and not for a change between preoperative and postoperative concentrations. Therefore, this evidence was labelled only as “postoperative” to differentiate it from a change in concentrations (as used for “combined pre-and postoperative cardiac troponin”). Although Rodseth et al. also evaluated changes between preoperative and postoperative concentrations, none of the change variables were significantly predictive of death and nonfatal myocardial infarction at 30 and 180 days after surgery. The results of the primary studies were not available thus we were unable to construct summary tables for combined pre- and postoperative B-type natriuretic peptides.
 Table 1:
Table 1: Evidence summary for stand-alone preoperative cardiac troponins. The left column indicates the overall certainty of evidence for all 12 outcomes
 Table 2:
Table 2: Evidence summary for combined pre- and postoperative cardiac troponins. The left column indicates the overall certainty of evidence for all 12 outcomes
 Table 3:
Table 3: Evidence summary for postoperative cardiac troponins. The left column indicates the overall certainty of evidence for all 12 outcomes
 Table 4:
Table 4: Evidence summary for preoperative B-type natriuretic peptides. The left column indicates the overall certainty of evidence for all 12 outcomes
 Table 5:
Table 5: Evidence summary for postoperative B-type natriuretic peptides. The left column indicates the overall certainty of evidence for all 12 outcomes
Summary of evidence tables (Tables 1–5) were constructed to show the certainty of evidence in three domains: (1) prognosis, (2) risk prediction, (3) biomarker-enhanced management strategy. For each domain, we rated the certainty of evidence as: no data, very low  , low
, low  , moderate
, moderate  , high
, high  for each of the 12 outcomes. An overall evaluation of the evidence across all outcomes was also made.
for each of the 12 outcomes. An overall evaluation of the evidence across all outcomes was also made.
Panelists appraised the balance of desirable and undesirable effects, values and preferences, resource use, health equity, acceptability and feasibility. Summaries of these judgements for preoperative (stand-alone) cTn, combined pre- and postoperative cTn, postoperative cTn, preoperative B-type NPs and postoperative B-type NPs are provided in Tables 6–10. An overall appraisal was made across ALL 12 outcomes and ALL three domains.
Table 6 - Summary of judgements for preoperative (stand-alone) cardiac troponins Preoperative (stand-alone) cardiac troponin overall judgement Is the problem a priority? No Probably no Probably yes Yes Varies Don’t know How substantial are DESIRABLE anticipated effects? Trivial Small Moderate Large Varies
Comments (0)