
Remember me



A randomized, controlled, single-blind study design was applied. The Ethics Committee of Cukurova University Faculty of Medicine approved the study (Date: 14.02.2020, decision no: 96), and the study protocol was registered to clinicaltrials.gov (NCT04308967). The study was conducted at a tertiary university hospital between March 2020 and April 2021. Written and verbal information about the protocol of the study was given to all participants, and written informed consent was obtained.
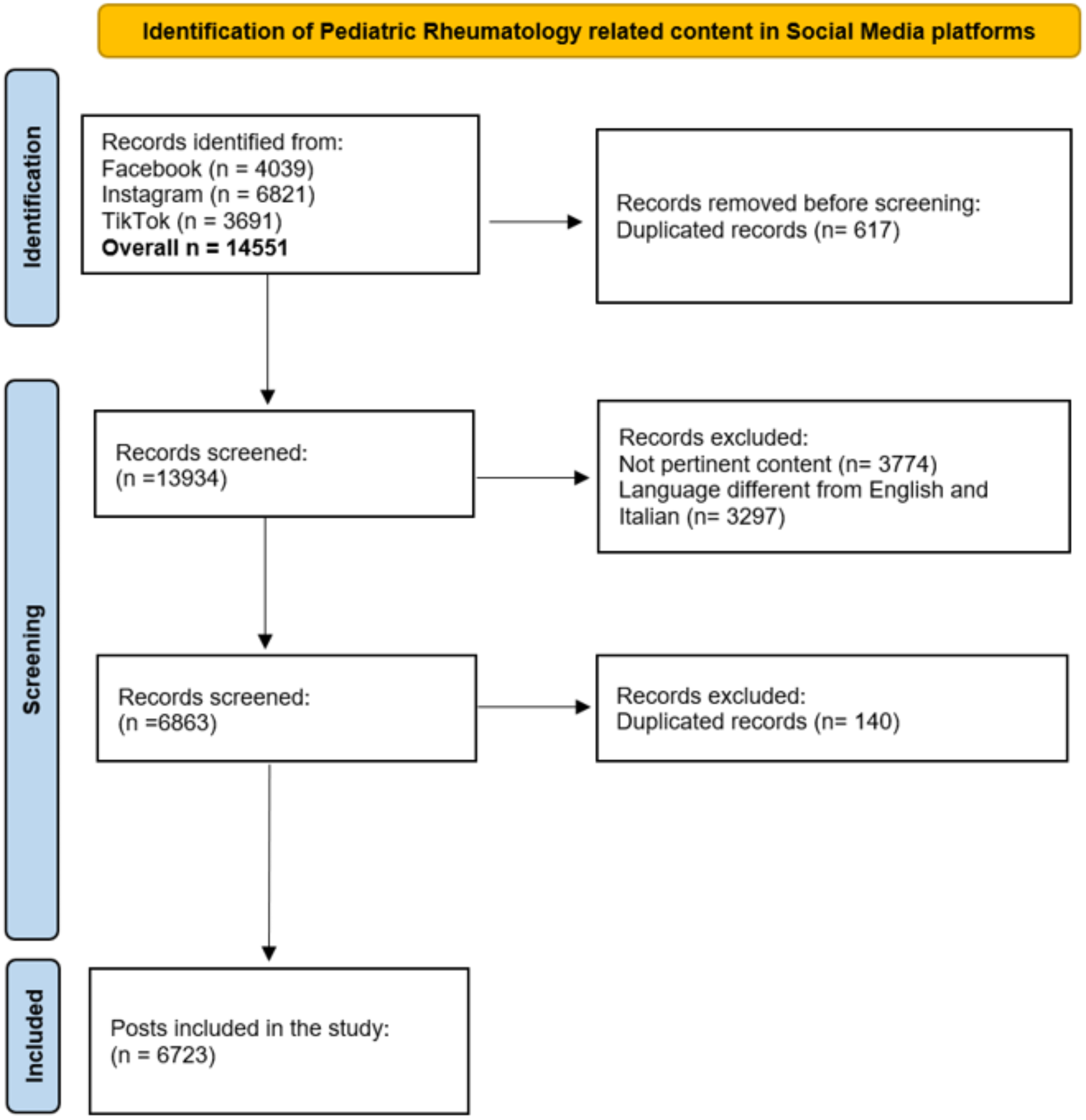
ParticipantsPatients who met all of the following inclusion criteria were included in the study: (i) diagnosed with primary knee OA based on the American College of Rheumatology criteria [19], (ii) having bilateral grade 2 or higher knee OA according to the Kellgren and Lawrence (KL) radiological grading system [20], and (iii) having a central sensitization score of 40 or higher according to the Central Sensitization Inventory (CSI) [21]. Patients who [i] were diagnosed with secondary knee OA, [ii] had at least one of the diseases in the B part of the CSI [21], (iii) had severe cognitive impairment, (iv) had a history of knee surgery, (v) received physiotherapy to the knee in the last 6 months, and (vi) had any injections to the knee joint during the previous 6 months were excluded. Patients were assigned to the treatment and control groups via the computerized randomization method by the research physiotherapist who did not participate in the evaluation process (Fig. 1). The evaluation of the participants was performed by a physiatrist who was blinded to the groups.
Fig. 1 Treatment protocol
Treatment protocolThe treatment group received a balance exercise program (Fig. 2), which consisted of three phases (each phase for 2 weeks), 3 days a week on alternating days for a total of 6 weeks. An exercise program, which was proven to be effective previously, was adopted, modified, and performed under the supervision of a physiotherapist [22]. The exercises were performed in three sets of eight to twelve repetitions. A five-minute aerobic warm-up period was applied before each session. Phase I of the program (0–2 weeks) included the following exercises: (i) in sitting position, holding 1 kg weight in hands and performing trunk rotation, (ii) standing up from sitting while holding the weights, iii) in standing position, rising on toes, (iv) side stepping aside while knees are flexed slightly, and (v) stepping each side on a plus ( +) sign formed by sticky bands on the floor. Phase II of the program (2–4 weeks) included the following exercises: (i) in standing position, holding 1 kg weight in hands and performing trunk rotation, (ii) climbing one stair up, (iii) rising on toes and walking slowly, (iv) stepping sideways onto step, and (v) stepping each side on a plus ( +) sign formed by sticky bands on the floor. Phase III of the program (4–6 weeks) included the following exercises: (i) starting from standing position, stepping one stair up while holding 1 kg weight in hands and performing trunk rotation, (ii) stepping forward and lowering into lunge, (iii) hopping while knees are flexed slightly, (iv) Tandem walk, and (v) 8-walk around cones [22] (Fig. 2).
Fig. 2
All patients in the treatment and control groups were informed about knee OA and the modifications that should be made in daily living activities to reduce the symptoms. Besides, a brief pain neuroscience education and a written brochure were given to the participants. The patients were allowed to use paracetamol (acetaminophen) when needed without exceeding 2 g/day.
EvaluationsDemographic characteristics such as age (years), gender, body height (cm), body weight (kg), and body mass index (BMI) of the patients were recorded. The assessment tools/questionnaires included the CSI, Visual Analog Scale (VAS), Berg Balance Scale, Y Balance Test, and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). The patients were evaluated by the same investigator three times: before the treatment (t0), at the end of the treatment (week 6) (t1), and at the 12th week (t2).
Central Sensitization Inventory (CSI)Central sensitization was evaluated by the CSI [21]. This inventory has moderate reliability in patients who develop central sensitization due to knee OA [23]. The CSI consists of 2 parts, part A and part B. Part A contains 25 items related to central sensitization symptoms, scored on a 4-point Likert scale. The total score in section A ranges from 0 to 100 points. A score of 40 and above indicates central sensitization (sensitivity: 81% and specificity: 75%). Part B evaluates whether the patient had been diagnosed with another disease in the family of central sensitization syndromes by any physician. A high score obtained by CSI indicates severe central sensitization [21].
Visual Analog Scale (VAS)Pain intensity at rest and pain during activity were evaluated by VAS. One end of the scale with a length of 10 cm represented “0 = no pain” and the other end represented “10 = most severe pain.” The value found by measuring the distance from the place marked by the patient to the “0 = no pain” point represented pain intensity [24].
Berg Balance ScaleBerg Balance Scale was used to evaluate functional balance [25]. Berg Balance Scale has high validity [intraclass correlation coefficient (ICC) = 0.95] in patients with knee OA [26]. The Berg Balance Scale is a 14-item test. A 4-point Likert scale is used for each item. The person gets a score between 0 and 56. Points between 0 and 20 represent “high fall risk”; 21–40, “medium fall risk”; and ≥ 41, “low fall risk”[25].
Y Balance TestY Balance Test, which requires strength, flexibility, and proprioception, was used to evaluate dynamic balance. This test includes extensions in the anterior, posterolateral, and posteromedial directions. The patient stands on one foot at the midpoint of the test setup. Then, the patient touches the anterior, posteromedial, and posterolateral directions with the other foot while maintaining balance with the toe tip. In all directions, the test was performed three times. The average is recorded in centimeters. The score was obtained by taking the average of three elongations for each direction, dividing this average by the leg length, and multiplying by 100 [27]. It has high reliability with median ICC values for intra-rater reliability being 0.88 (0.84–0.93), 0.90 (0.68–0.94), and 0.88 (0.85–0.94) for the anterior, posterolateral, and posteromedial directions, respectively [28].
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)WOMAC was used to assess physical function, knee pain, and stiffness. This questionnaire, which consists of 24 questions and three parts (pain, stiffness, physical function), also has good validity and reliability in patients with knee OA [29]. The total WOMAC score ranges from 0 to 30, with high scores indicating severe loss of function, pain, and stiffness. The minimum clinically significant difference is 1.33 points.
Statistical analysisA per-protocol analysis was conducted, and data of the participants who partook in three assessments were analyzed. Statistical analysis was performed using the IBM® SPSS® Statistics for Windows, version 23.0 software (IBM Corp. Armonk, NY, USA). Visual methods (histograms and probability plots) and the Shapiro–Wilk test were performed to test the normality of data. Descriptive data were expressed in mean and standard deviation (SD) and number/frequency. To analyze within-group changes and between-group differences, a two-way repeated measures of analysis of variance (ANOVA) test [time × group (within-subject × between-subject)] were applied. A p value < 0.05 was considered statistically significant. Cohen’s d was calculated for the effect size of the significant difference. For within-group pairwise comparisons of delta values, a Bonferroni correction was applied. p values < 0.017 were considered statistically significant. A two-model multiple linear regression analysis was performed to determine the underlying factor(s) through which balance exercises improved central sensitization. In this analysis, change in VAS pain (during activity) constituted the first model as an independent variable. Delta values of Y Balance Test and WOMAC pain, WOMAC physical function, and WOMAC total scores were included in the second model. A p value < 0.05 was regarded as statistically significant. The required sample size was calculated using the G*Power® program (Heinrich Heine Universität Düsseldorf, Düsseldorf, Germany). ANOVA repeated measures and within-between interactions were used in the system. Considering the study performed by Lluch et al. [6], the effect size was determined at 0.252. The correlation between repeated measurements assumed was 0.5. Considering three measures in two study groups, the sphericity correction was determined at 1.0. The statistical power was set as 0.95 and the alpha level as 0.05. The sample size was estimated as 44 participants. Considering a possible loss to follow-up of up to 10%, 48 patients (n = 24 in each group) were recruited.
Comments (0)