
Remember me





The tibiotalar joint is commonly described as a mortise and tenon joint because of its resemblance to the woodworking joint bearing the same name. The talar dome is stabilized beneath the distal tibia by osseous and ligamentous structures.1 Medially, the deltoid ligamentous complex stabilizes the talus against the medial malleolus. The deltoid complex is divided into deep and superficial ligament groups. The superficial deltoid originates from the medial malleolus and has a broad fan-like insertion on the talus, calcaneus, and navicular and functions as the primary restraint to hindfoot eversion.1,2 The deep deltoid ligament is confluent with the ankle capsule and inserts on the talus to provide primary restraint to the talar external rotation.3 Complete disruption of the deltoid complex leads to reduced surface contact areas and instability.4 The rationale for deltoid ligament repair is to restore the medial tether and optimize tibiotalar kinematics.3
Traditionally, deltoid repair has been performed with an open technique utilizing a medially based incision from the medial malleolus to the talus. Described techniques involve the placement of 1 or 2 suture anchors on the medial malleolus and/or the talus.5–9 The free limbs of the suture are then passed through the remnant deltoid ligament tissue incorporating the deep, superficial, and capsular layers. The use of a suture button to secure the free limbs to the medial malleolus has also been described.9 Although literature comparing repair techniques is sparse, a recent study comparing talar and malleolar anchor placement found no difference in radiologic or functional outcomes.10
In recent years, arthroscopic deltoid ligament repair has been reported for use in the treatment of both multidirectional ankle instability and ankle fractures.11–14 Vega et al11 first reported an all-inside arthroscopic deltoid repair technique in 13 patients who underwent simultaneous medial and lateral ankle repair for chronic ankle instability. They utilized a single suture passed and looped through the avulsed ligament and fixed it back to the medial malleolus with a suture anchor. Twelve of 13 patients returned to activity with no discomfort, while one had persistent medial ankle pain. Barbachan Mansur et al12 reported their series of 20 ankle fractures that underwent arthroscopic repair utilizing the technique described by Vega et al11 and reported excellent clinical results.
Kim et al13 published an arthroscopic repair technique using a single medial malleolus suture anchor and percutaneously passed sutures. They emphasized the importance of utilizing a “safe zone” between the saphenous vein and the tibial nerve.11 Acevedo et al14 utilized a similar technique and expanded on the safe zone concept, identifying a suture-passing triangle between the inferior medial malleolar tip, the medial tibialis anterior tendon, and the anterior border tibialis posterior tendon. They reported a 90% satisfaction rate in 87 patients.
The current technique describes how to perform an arthroscopic 2-suture anchor technique to stabilize the medial ankle. It is also the only all-inside technique to utilize osseous fixation on both the tibia and the talus.
INDICATIONS AND CONTRAINDICATIONSArthroscopic repair of the deltoid ligament complex is indicated for patients who have ligament disruption and medial instability. This approach can be utilized to repair isolated medial ligament instability or can be combined with an arthroscopic repair of chronic multidirectional instability. It can be used for fracture cases such as Maisonneuve patterns of bimalleolar equivalent fractures. Although it remains controversial which patients with bimalleolar equivalent ankle fractures would benefit from deltoid ligament repair, an arthroscopic technique provides the potential benefit of simultaneously addressing osteochondral lesions and directly visualizing the reduction of the ankle syndesmosis.15,16 In our practice, arthroscopic repair has been utilized for patients with bimalleolar equivalent ankle fractures.
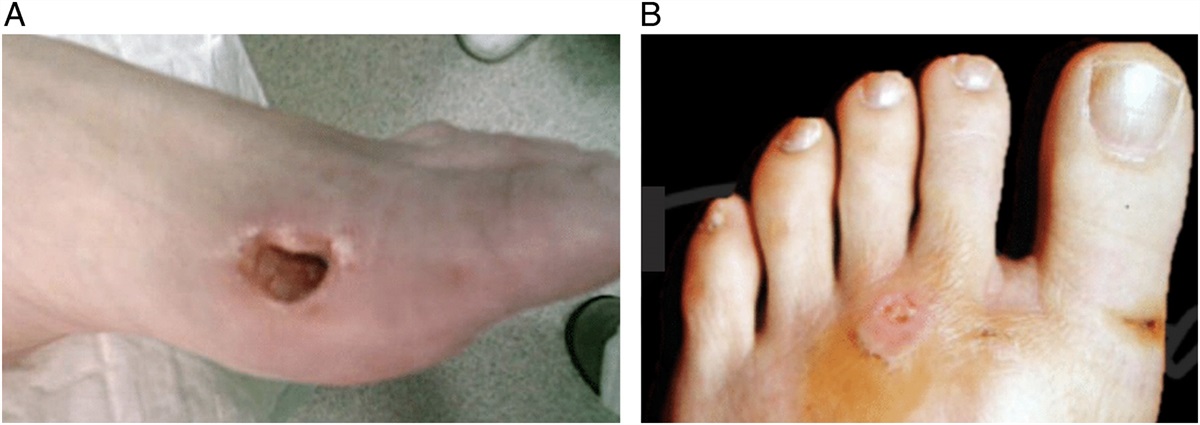
Contraindications to arthroscopic deltoid ligament repair include open fractures, medial wounds, active infections, and uncontrolled diabetes. While arthroscopic repair is more preserving of the soft tissue envelope in comparison to an open technique, we caution against acute repair in these high-risk populations. In addition, this technique requires the surgeon to recognize traumatically altered anatomy. Surgeons without significant experience in ankle arthroscopy may consider an open technique.
PREOPERATIVE PLANNINGDiagnosis of medial ligament injuries remains a challenge as physical exam and standard radiographs are unreliable.3,17 Manual and gravity stress are commonly used techniques to identify deltoid ligament injury, with >4 mm medial clear space traditionally used as an indicator of medial instability. The presence of a medial malleolus “fleck sign” is also predictive of deltoid incompetence.18 Although not routinely obtained for traumatic scenarios in our practice, magnetic resonance imaging remains the most reliable noninvasive diagnostic tool and may be beneficial for chronic multidirectional instability cases. Evaluation under anesthesia and fluoroscopy before or during surgical intervention can reveal deltoid ligament injury not evident on preoperative imaging.
TECHNIQUEThe patient is positioned supine on the operating table. Baseline valgus and external rotation stress views are obtained intraoperatively under fluoroscopy (Fig. 1). Comparison images of the noninjured side may be obtained at this time. Preoperative antibiotics are administered and a thigh tourniquet is placed. After prepping and draping, the notable surface anatomy is carefully drawn on the patient’s skin. Attention is given to identifying the location of the tibialis anterior, superficial peroneal nerve, the saphenous vein, and the posterior tibial tendon (Fig. 2), all of which course near the anticipated portal sites. An ankle distractor strap is applied and gentle traction is placed across the ankle joint.
 FIGURE 1:
FIGURE 1: Intraoperative stress imaging of medial ligamentous complex.
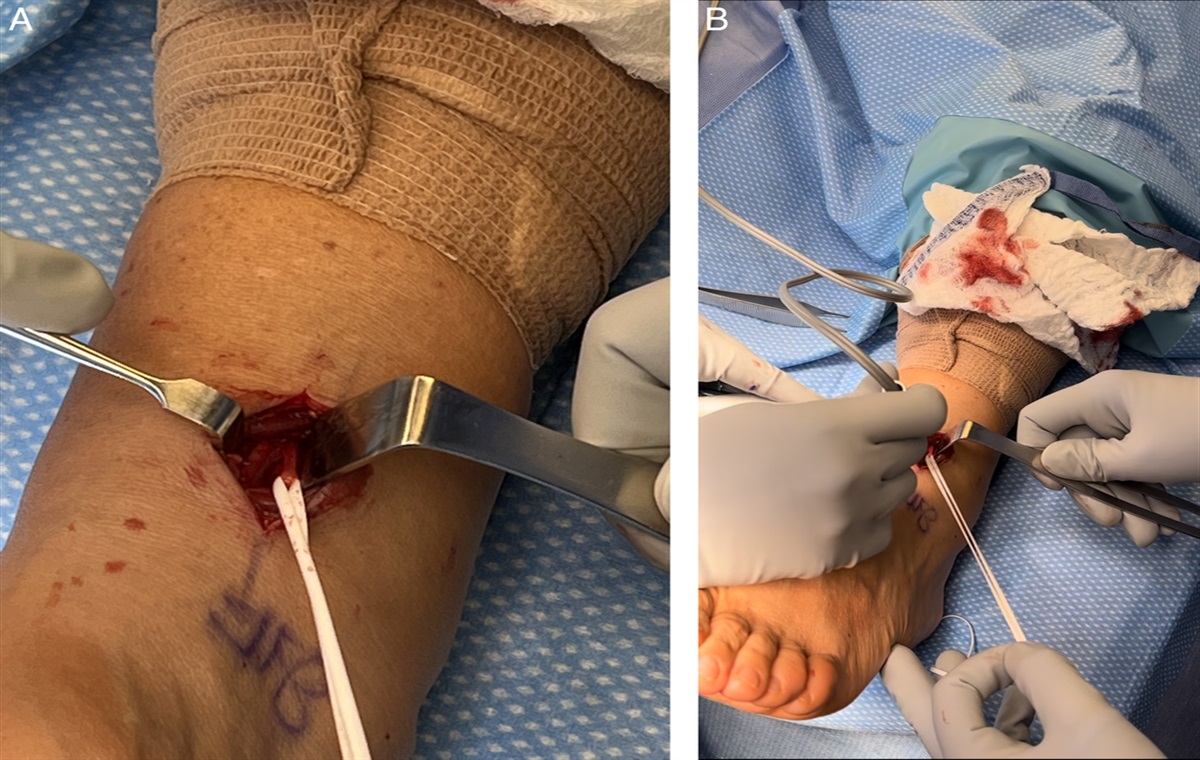
 FIGURE 2:
FIGURE 2: Superficial surface anatomy. AM, accessory medial portal; M, medial malleolus; MP, anteromedial portal; PT, posterior tibial tendon; S, saphenous vein; SN, superficial peroneal nerve; TN, tibial neurovascular bundle.
In our series, attention is first turned to the arthroscopic portion of the case. A nick-and-spread technique is used to create standard anterolateral and anteromedial portals. Extensive hematoma extrusion is typically encountered during portal creation. The arthroscope is advanced through the anterolateral portal and a standard diagnostic exam is performed. We typically begin at low-pressure inflow (20 mm Hg) but have increased to as high as 40 mm Hg without excessive extravasation. A 3.5-mm shaver is used for moderate debridement of the ankle joint. At this point, the degree of medial ligamentous disruption is appreciated. In our series, the deep and superficial layers of the deltoid have all been in discontinuity. It is important to assess for loose bodies or other osteochondral defects during the diagnostic portion of the procedure.
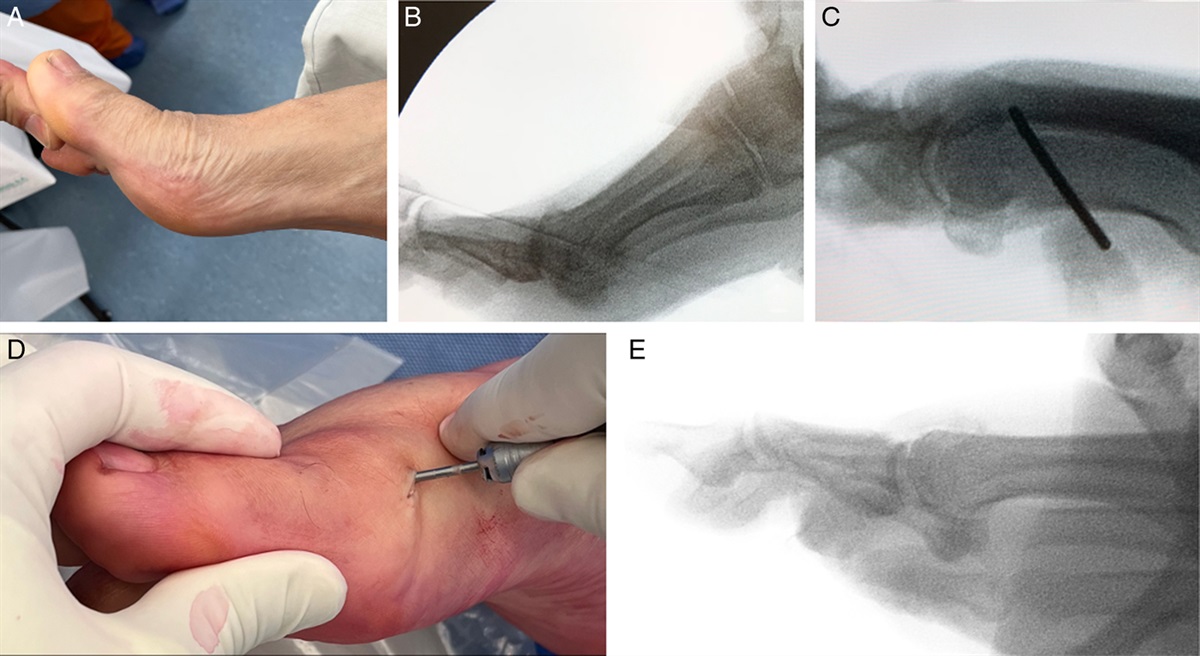
The deltoid repair is performed with 2 suture anchors. An accessory medial portal is created distal to the tip of the medial malleolus. The posterior tibial tendon can be reliably avoided by keeping the accessory portal just anterior to the midline of the distal most tip of the medial malleolus. Through the accessory portal, a 2.3-mm unicortical drill hole is made at the medial talus distal to the medial tibiotalar articular cartilage and parallel with the plafond (Fig. 3). Next, a double-loaded suture anchor (Iconix 2 TT, Stryker) is placed in the drill hole. The 2 free limbs of the attached suture tapes are then retrieved through the anteromedial portal. The suture limbs are subsequently passed through the eyelet of a self-punching knotless anchor system (Omega, Stryker). The loaded suture anchor is then advanced through the anteromedial portal, keeping the free ends outside of the skin for later tensioning. The ankle is manually reduced and held in neutral dorsiflexion. The tibial anchor is placed at the central tip of the medial malleolus in the coronal and sagittal planes (Fig. 4). After the location is confirmed with fluoroscopy, the suture anchor is malleted in place with gentle taps while the construct is manually tensioned to the surgeon’s liking by pulling the suture limbs fed through the Omega anchor (Fig. 5).
 FIGURE 3:
FIGURE 3: Intraoperative placement of talar suture anchor. A pilot hole is drilled and a double-loaded suture anchor is placed. Anc, position of suture anchor placement; LC, arthroscope light cord crossing field; Sc, arthroscope through anteromedial portal; Ta, talus; Ti, tibia.
 FIGURE 4:
FIGURE 4: Confirmation of the medial malleolar suture anchor location. Suture limbs from the talus anchor are passed through the eyelet of the talus anchor. The reduction must be held (not shown) before tensioning the suture and malleting the anchor in place.
 FIGURE 5:
FIGURE 5: A, Medial malleolar anchor in place before punching. B, Buried medial malleolar anchors with tensioned sutures. The reduction of the medial articular shoulder can be visualized.
The fibula may be instrumented before or after ligamentous repair if indicated. Following the completion of all instrumentation, the ankle is once again stressed under fluoroscopy to assess the integrity of the syndesmosis and medial ligamentous complex. The excess suture limbs may then be cut.
The wounds are irrigated and closed. A well-padded posterior splint is applied over sterile dressings.
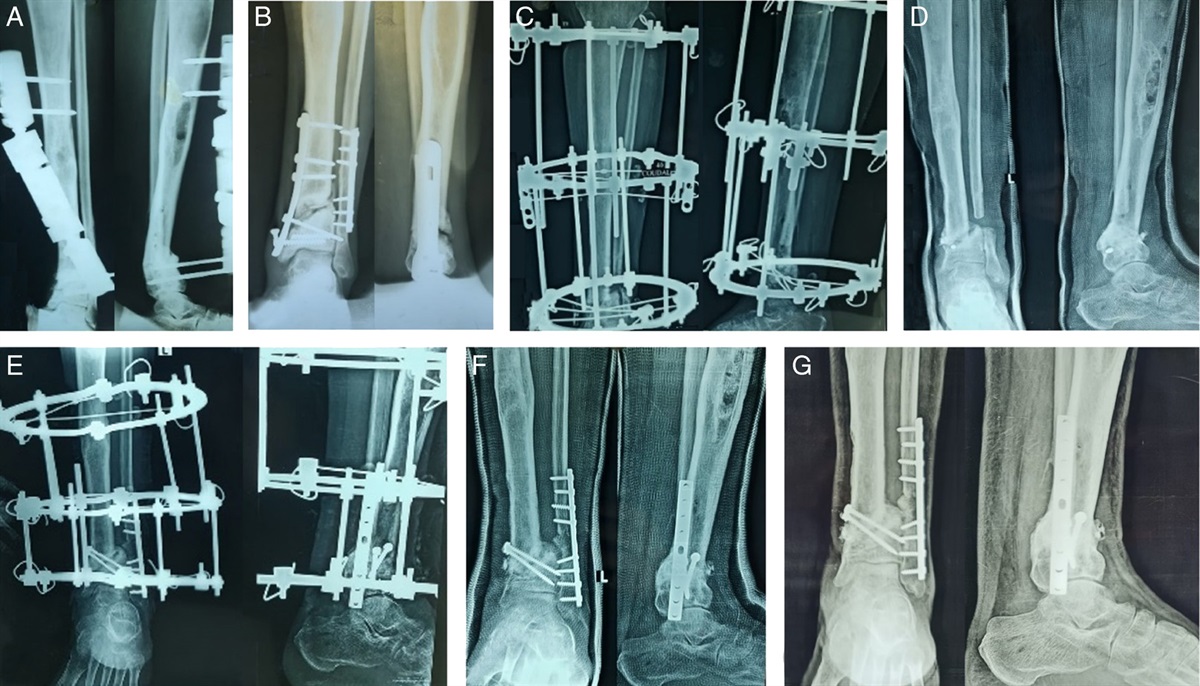
RESULTSThis technique has been performed on 3 ankles (3 patients) all for bimalleolar or trimalleolar equivalent fractures. All were closed injuries. The average age was 29.6 (range, 25 to 35) years. No patients had a prior history of ankle fracture, arthritis, neuropathy, smoking, or diabetes. Anatomic reduction of the mortise was achieved in all ankles. To date, our longest clinical follow-up is 1 year, with an American Orthopaedic Foot and Ankle Score of 82 and a Lower Extremity Functional Score of 73. Radiographically, the mortise remains anatomically reduced at 1 year (Fig. 6). Medial clear space was equal between injured and uninjured extremities on weight-bearing views (2 mm). Injury and postoperative images from 2 additional patients are shown in Fig. 7. There have been no complications to date.
 FIGURE 6:
FIGURE 6: One-year postoperative weight-bearing films. A, Uninjured side. B, Operative side.
 FIGURE 7:
FIGURE 7: Preoperative and postoperative ankle mortise films of additional patients who underwent arthroscopic deltoid ligament repair using this technique. A, A Weber C ankle fracture (left) treated with proximal fibula shaft open reduction internal fixation (not shown), syndesmosis fixation, and deltoid ligament repair (right). B, A trimalleolar ankle fracture (left) treated with fibula open reduction internal fixation, syndesmosis fixation, and deltoid ligament repair (right).
COMPLICATIONSRisks inherent to anterior ankle arthroscopy with the use of a standard anterolateral portal include injury to the superficial peroneal nerve. When making the stab incision for the accessory medial portal for placement of suture anchors, damage to the posterior tibial tendon, saphenous vein, and tibial neurovascular structures is possible. Identifying surface anatomy and utilizing the described “safe zones” as described by Kim et al13 and Acevedo et al14 can help minimize these risks.
POSTOPERATIVE MANAGEMENTA short leg splint is applied. Dressings and sutures are removed at the 2-week follow-up appointment. The patient is transitioned to a walking boot but kept non–weight-bearing until their 6-week follow-up. Further appointments are scheduled for 3, 6, and 12 months. Further precautions may be dictated by the presence of additional pathology.
POSSIBLE CONCERNS AND FUTURE OF THE TECHNIQUEThe indications for deltoid ligament repair continue to be controversial. A recent meta-analysis of 5 studies and 281 patients with bimalleolar equivalent ankle fractures concluded that no clear indications for repair exist.19 Still, 30% of patients who did not have repair complained of persistent medial symptoms.15 As the literature does not clearly define the benefit of deltoid repair, some may consider an additional incision an unnecessary risk factor for surgical infection. Although traditional open deltoid repair has not been associated with increased infectious risk, the use of an arthroscopic technique may further minimize this potential complication.19
Arthroscopic treatment of chronic lateral ankle instability has become increasingly popular in recent years and has shown outcomes equivalent to open techniques.20,21 Vega et al11 reported 100% satisfaction in their series of 13 patients who underwent a combined medial and lateral arthroscopic repair procedure for multidirectional ankle instability. While we have not yet performed our described technique in a chronic instability case, we believe it would also effectively treat that pathology.
While this technique does not entail passing sutures directly through the ruptured fibers of the deltoid ligament, we still consider this to be an indirect repair of the tibiotalar portion of the deltoid ligament. However, some may consider this technique a form of deltoid fixation rather than repair. We consider both terms to be accurate, akin to the interchangeable use of fixation and repair when discussing the treatment of syndesmosis through indirect means in the literature.22–24
In summary, the deltoid ligament is a medial ankle tether that is frequently disrupted in ankle fractures. While indications for repair are not clearly defined, repair of the deltoid is thought to restore anatomy and ankle kinematics.15 The current technique describes an all-inside arthroscopic deltoid ligament repair using osseous fixation on the medial malleolus and talus. This technique provides anatomic reduction of the medial ankle mortise and has shown good early clinical outcomes without any complications. Additional benefits of an arthroscopic technique include direct visualization of the ankle syndesmosis and the opportunity to treat symptomatic osteochondral injuries.25 A prospective trial is warranted to further elucidate the effectiveness of this technique compared with an open approach.
REFERENCES 1. Campbell KJ, Michalski MP, Wilson KJ, et al. The ligament anatomy of the deltoid complex of the ankle: a qualitative and quantitative anatomical study. J Bone Joint Surg Am. 2014;96:e62. 2. Lötscher P, Lang TH, Zwicky L, et al. Osteoligamentous injuries of the medial ankle joint. Eur J Trauma Emerg Surg. 2015;41:615–621. 3. Lee S, Lin J, Hamid KS, et al. Deltoid ligament rupture in ankle fracture: diagnosis and management. J Am Acad Orthop Surg. 2019;27:e648–e658. 4. Earll M, Wayne J, Brodrick C, et al. Contribution of the deltoid ligament to ankle joint contact characteristics: a cadaver study. Foot Ankle Int. 1996;17:317–324. 5. Lack W, Phisitkul P, Femino JE. Anatomic deltoid ligament repair with anchor-to-post suture reinforcement: technique tip. Iowa Orthop J. 2012;32:227–230. 6. Woo SH, Bae SY, Chung HJ. Short-term results of a ruptured deltoid ligament repair during an acute ankle fracture fixation. Foot Ankle Int. 2018;39:35–45. 7. Hsu AR, Lareau CR, Anderson RB. Repair of acute superficial deltoid complex avulsion during ankle fracture fixation in National Football League players. Foot Ankle Int. 2015;36:1272–1278. 8. Yu GR, Zhang MZ, Aiyer A, et al. Repair of the acute deltoid ligament complex rupture associated with ankle fractures: a multicenter clinical study. J Foot Ankle Surg. 2015;54:198–202. 9. Luckino FA 3rd, Hardy MA. Use of a flexible implant and bioabsorbable anchor for deltoid rupture repair in bimalleolar equivalent Weber B ankle fractures. J Foot Ankle Surg. 2015;54:513–516. 10. Park YH, Jang KS, Yeo ED, et al. Comparison of outcome of deltoid ligament repair according to location of suture anchors in rotational ankle fracture. Foot Ankle Int. 2021;42:62–68. 11. Vega J, Allmendinger J, Malagelada F, et al. Combined arthroscopic all-inside repair of lateral and medial ankle ligaments is an effective treatment for rotational ankle instability. Knee Surg Sports Traumatol Arthrosc. 2020;28:132–140. 12. Barbachan Mansur NS, Raduan FC, Lemos A, et al. Deltoid ligament arthroscopic repair in ankle fractures: case series. Injury. 2021;52:3156–3160. 13. Kim JG, Gwak HC, Lee MJ, et al. Arthroscopic deltoid repair: a technical tip. J Foot Ankle Surg. 2017;56:1253–1256. 14. Acevedo JI, Kreulen C, Cedeno AA, et al. Technique for arthroscopic deltoid ligament repair with description of safe zones. Foot Ankle Int. 2020;41:605–611. 15. Doty JF, Dunlap BD, Panchbhavi VK, et al. Deltoid ligament injuries associated with ankle fractures: arguments for and against direct repair. J Am Acad Orthop Surg. 2021;29:e388–e395. 16. Martin KD, Callender NW, Luplow C, et al. High ankle syndesmosis disruption: all-inside arthroscopic reduction and internal fixation. Tech Foot Ankle Surg. 2023;22:14–19. 17. DeAngelis NA, Eskander MS, French BG. Does medial tenderness predict deep deltoid ligament incompetence in supination-external rotation type ankle fractures? J Orthop Trauma. 2007;21:244–247. 18. Nwosu K, Schneiderman BA, Shymon SJ, et al. A medial malleolar “fleck sign” may predict ankle instability in ligamentous supination external rotation ankle fractures. Foot Ankle Spec. 2018;11:246–251. 19. Dabash S, Elabd A, Potter E, et al. Adding deltoid ligament repair in ankle fracture treatment: is it necessary? A systematic review. Foot Ankle Surg. 2019;25:714–720. 20. Corte-Real NM, Moreira RM. Arthroscopic repair of chronic lateral ankle instability. Foot Ankle Int. 2009;30:213–217. 21. Vega J, Golanó P, Pellegrino A, et al. All-inside arthroscopic lateral collateral ligament repair for ankle instability with a knotless suture anchor technique. Foot Ankle Int. 2013;34:1701–1709. 22. Degroot H, Al-Omari AA, El Ghazaly SA. Outcomes of suture button repair of the distal tibiofibular syndesmosis. Foot Ankle Int. 2011;32:250–256. 23. Chen B, Chen C, Yang Z, et al. To compare the efficacy between fixation with tightrope and screw in the treatment of syndesmotic injuries: a meta-analysis. Foot Ankle Surg. 2019;25:63–70. 24. Parker AS, Beason DP, Slowik JS, et al. Biomechanical comparison of 3 syndesmosis repair techniques with suture button implants. Orthop J Sports Med. 2018;6:2325967118804204. 25. Leontaritis N, Hinojosa L, Panchbhavi VK. Arthroscopically detected intra-articular lesions associated with acute ankle fractures. J Bone Joint Surg Am. 2009;91:333–339.
Comments (0)