
Remember me




This prospective study evaluated the accuracy of implant placement in a clinical setting using a dynamic navigation system (DCARER, Suzhou Digital-health Care Co. Ltd.), static surgical guide, and freehand placement. The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee at the Xian Jiaotong University Hospital of Stomatology, Xian, China (xjkqII[2021] No: 043). It was also registered with the TCTR identification number TCTR20230804001 on 04/08/2023 at Thai Clinical Trials Register-Medical Research Foundation of Thailand (MRF). All participants in this study provided written informed consent.
Patient recruitmentPatients seeking implant treatment were randomly assigned to each group and underwent implant placement at Xi’an Jiaotong University Hospital of Stomatology (Xi’an, China) between November 2021 and February 2023.
The inclusion criteria were as follows:
1.Patients over 21 years old.
2.Partially edentulous and in need of one or more dental implants.
3.Agreed to sign a consent form.
The exclusion criteria were as follows:
1.Heavy smokers (> 10 cigarettes a day).
2.Metabolic bone disorders.
3.Uncontrolled diabetes.
4.History of radiotherapy in the head and neck region.
5.Patients who required extensive bone grafting.
Randomization was carried out using sealed opaque envelopes, each containing cards denoting one of the three groups. Patients were requested to draw envelopes. The implant surgeries were performed by a trained and experienced surgeon, aided by a CBCT-based prosthetically oriented digital implant planning. Subsequently, postoperative CBCT scans were acquired, and accuracy was measured through the superimposition of the postoperative CBCT scans and the preoperative plan. All CBCT scans were obtained using Meyer Dental CBCT machine (Meyer, China) with standard exposure parameters (16.7 cm x 11.0 cm FOV, 0.2 mm voxel size, 100 kV, 10 mA). Detailed methodologies for each group are explained further below.
Sample size calculation was conducted based on the deviation values for dynamic navigation, static surgical guides, and freehand placement as reported in previous studies [20,21,22]. Computer Software (G*Power software version 3.1.9.6, Erdfelder, Faul, Buchner, & Lang) was used to calculate the sample size, yielding a required total sample of 90, 87, and 66 implants for entry point, apical and angular deviations, respectively. The significance level was set at 0.05, with 90% power. The calculation method is consistent with previous comparable studies [2, 22, 23].
Study Hypothesis 1)There is a significant difference between computer-guided implant placement and freehand implant placement.
2)Dynamic navigation and static surgical guides offer similar accuracy.
Dynamic navigationThe dynamic navigation system utilizes infrared light emitted from devices affixed to the handpiece and within the patient’s mouth. This light is tracked by cameras to provide real-time feedback and guidance regarding the handpiece’s position and angulation. To register the patient accurately in the navigation software, a registration device with fiducial markers was attached to the patient’s jaw. A CBCT scan was obtained with this device positioned in the same quadrant as the planned implant site. Subsequently, DICOM data was transferred to the software, allowing for the design of virtual implants in accordance with the desired position, angulation, and implant dimensions. After placing the positioning devices, calibration of the surgical handpiece and jaw positions was carried out. An oral positioning device was securely fixed on the opposite side of the implant site using a resin material. The registration device with fiducial markers was then used to coordinate and link the patient’s mouth with the CBCT data in three dimensions. Soft tissue reflection was performed under local anesthesia, and each drill was calibrated before use. Site preparation was performed under real-time guidance from the dynamic navigation system (Fig. 1). Finally, a postoperative CBCT scan was taken, and the data were transferred to an individual not involved in the treatment for analysis. Patient data were registered using case numbers with no identifiers.
Fig. 1
Workflow using dynamic navigation (a) registration device adapted intraorally before taking a CBCT scan (b) the CBCT scan is uploaded to the software and calibrated with the real-life situation by detection of fiducial markers, followed by treatment planning. (c) calibration of the handpiece and drills using the positioning device (d) the positioning device is attached to the registration device (e) surgery performed under dynamic navigation guidance (f) real-time display of the procedure and is shown on screen
Preoperative CBCT scans, postoperative CBCT scans, and the surgical plan were used to analyze the data and measure accuracy. 3D models constructed from CBCT scans were superimposed using accuracy analysis software of Dcarer implant navigation. The software utilized built-in algorithms to calculate angular and positional deviations between the placed implant and the virtual plan.
Static surgical guidePreoperative CBCT scans and intraoral scans were obtained prior to the surgery. Implant treatment planning and the design of tooth-supported surgical guides were carried out using Implant Studio software (3Shape, Copenhagen, Denmark). SLA surgical guides were then manufactured using a Perfactory® 4 Digital Dental Printer (DDP4) Series (Envisiontec, Dearborn, MI, USA). The surgical guides had a uniform thickness of 2 mm and were equipped with closed sleeves. The surgeon verified the proper fit of the guides, and the surgeries were conducted under local anesthesia. Postoperative CBCT scans were acquired for the purpose of accuracy analysis. The preoperative plan and intraoral scans were subsequently uploaded to another software application (RemebotDent, Beijing Ruiyibo Technology Co., Ltd). A 3D structure was created by combining the CBCT data with the 3D intraoral scan. The postoperative CBCT was then superimposed on the preoperative CBCT and the initial plan. The software was used to pinpoint the exact location of the placed implant, and deviations were calculated through the software’s algorithms (Fig. 2). Ultimately, the data was extracted and systematically organized.
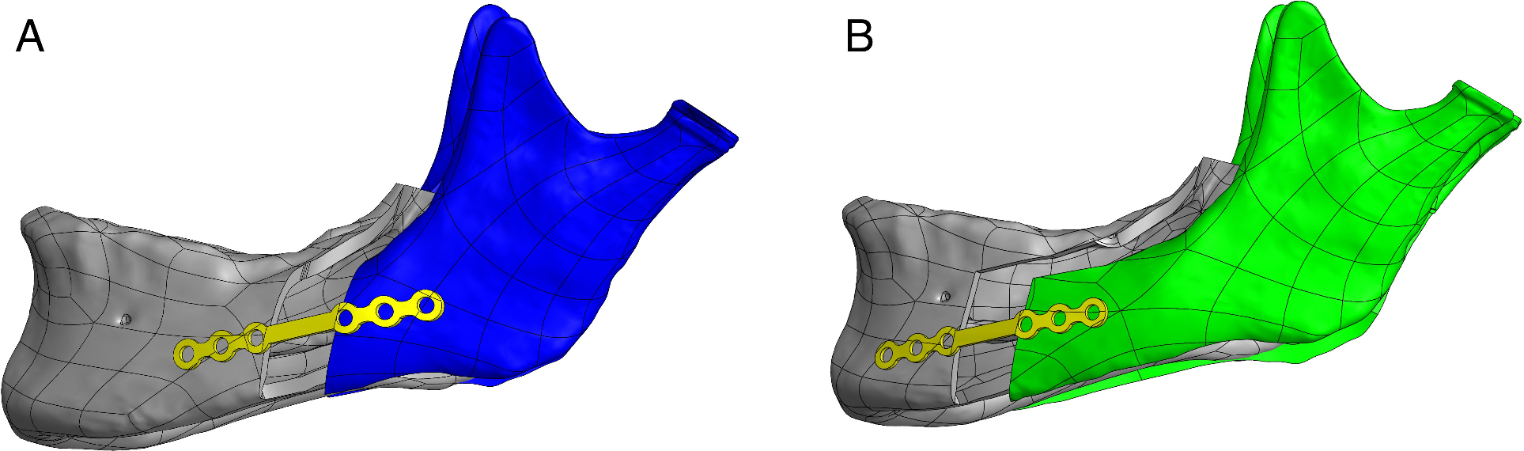
Fig. 2
Superimposition of the postoperative CBCT and the preoperative plan showing the planned implant (red) and the actual implant outlines (green)
Freehand approachFollowing the initial patient examination and CBCT acquisition, the implant surgery was scheduled. On the day of the surgery, the preoperative CBCT data was uploaded into the RemebotDent software. The surgeon then directly designed the implant treatment plan using this software. To enhance visualization and facilitate angle adjustments, a virtual prosthetic crown was used. In an effort to minimize any deviations and employ a form of “mental navigation,” the surgeon assessed the implant positions and angulations from both coronal and sagittal views. Subsequently, the implant placement surgery was performed promptly, with laser markers on drills providing depth references. After surgery, a postoperative CBCT was taken and uploaded to the same software followed by superimposition and deviation calculation. A deviation report was then exported and saved.
Deviation analysisAn experienced technician performed the deviation calculation process for all the implants. A total of seven deviation values were calculated (Fig. 3). The primary outcome variables were defined as follows:
Fig. 3
Deviation calculations between the planned and actual implants: (a) global platform deviation (b) global apical deviation (c) angular deviation (d) platform lateral deviation (e) apical lateral deviation (f) platform depth deviation (g) apical depth deviation
1.Angular deviation: Representing the largest angle between the axes of the planned and the actual implants.
2.Platform deviations: These include depth, lateral, and global (3D) deviations measured at the implant shoulder.
3.Apical deviations: These include depth, lateral, and global (3D) deviations measured at the apical point of the implant.
Additionally, demographic and consistency analyses were conducted to investigate the descriptive and deviation values of each group individually, as well as detect any significant differences regarding implant positions (maxilla vs. mandible, anterior vs. posterior, left vs. right), sex, age, and implant dimensions.
Statistical analysisStatistical analysis was conducted using SPSS® Statistics version 27 (IBM Corp. 2020, NY, USA). A descriptive analysis of the accuracy values was carried out using means and standard deviations. The level of significance was set at p < 0.05. The Shapiro-Wilk test was performed at each step to assess normal distribution. Levene’s test was applied to determine the equality of variances. No missing data were reported.
Demographic and consistency analyses for each group were performed using the independent samples t-test and the Mann-Whitney U test. One-way analysis of variance (ANOVA) was utilized to compare deviation values among the three groups. For statistically significant values, post-hoc Tukey’s HSD and Tamhane’s T2 tests were employed to identify significant outcomes.
Comments (0)