
Remember me




This study was based on retrospective data obtained from orthodontic records at the Peking University School and Hospital of Stomatology, and it was approved by the institution’s biomedical ethics committee (approval number: PKUSSIRB-201630096, retrospectively registered). The patients included in this study accepted orthodontic treatment between 2006 and 2018.
The study’s sample selection was based on the following inclusion criteria: good-quality orthodontic records, the presence of permanent dentition, age > 18 years, a convex profile, skeletal class II (ANB > 5°), and a hyperdivergent skeletal pattern (FMA > 28°) [24]. The exclusion criteria included the following: dental anomalies in size, number, shape, or structure; permanent tooth loss; orthodontic–orthognathic combined surgery treatment; and Botox injection or prosthesis implantation before or during orthodontic treatment.
Treatment protocolsAll the participants underwent systematic periodontal and endodontic assessments and therapies before orthodontic interventions. A straight-wire MBT technique was utilized after the extraction of four premolars from all patients. Braces and archwires were obtained from TP Orthodontics (La Porte, IN, USA). The alignment and leveling phases involved initial bracket-bonding followed by a certain procedure utilizing 0.014 in. NiTi, 0.016 in. NiTi, 0.016 in. × 0.022 in. NiTi, and 0.019 in. × 0.025 in. NiTi archwires sequentially. During the space-closing phase, a 0.019 × 0.025 in. stainless steel archwire was applied using a conventional sliding mechanism. This phase was terminated upon the complete closure of the premolar spaces. The patients’ dentition was finely adjusted before debonding. Miniscrews (diameter: 1.5 mm; length: 7 mm; Zhongbang Medical Treatment Appliance, Xi’an, China) were surgically inserted into the alveolar ridge.
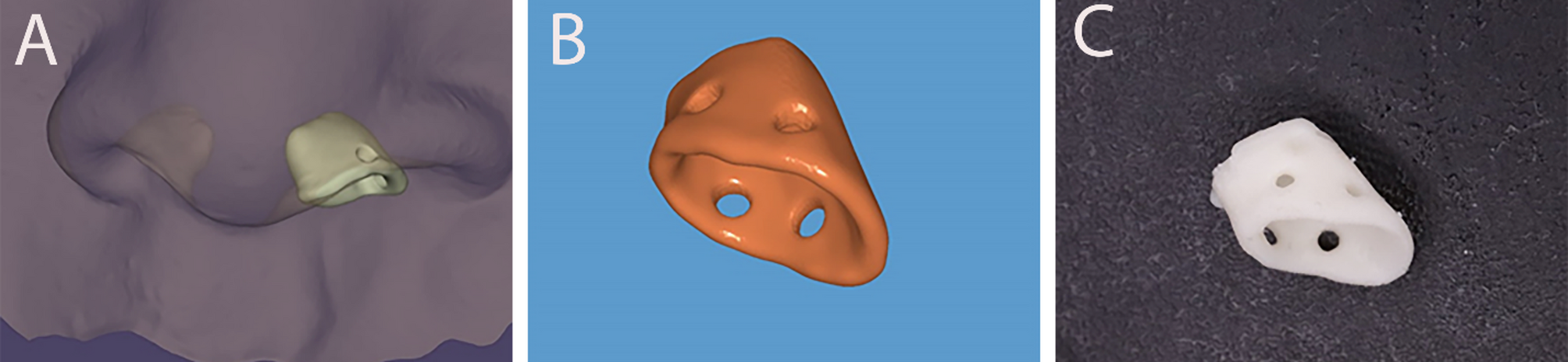
The patients were divided into two groups: (1) the maxillary maximum anchorage (MMA) group, in which TADs were implanted only at the bilateral buccal side of the alveolar bone, between the roots of the upper premolar and the upper first molar or between the upper first molar and the upper second molar; and (2) the maxillary maximum anchorage with vertical control (MMA + VC) group, in which TADs were implanted into the bilateral buccal and lingual sides of the alveolar bone, between the roots of the upper first molar and the upper second molar, to intrude the upper molars with or without the TADs implanted in the anterior segment for incisor intrusion (Fig. 1).
Fig. 1
Representative image of intraoral devices. A. TAD-assisted intrusion of the upper anterior teeth. B. Buccal view of the posterior intrusion devices. C. Palatal view of the posterior intrusion devices
Sample size calculationIn this study, the effect size of the primary outcome was expected to be 2.32. This number was the difference in mandibular counterclockwise rotation (the decrease in the FMA value) between the two groups calculated in our preliminary study. The sample size was calculated using online software (http://hedwig.mgh.harvard.edu/sample_size/) by assuming 5% type I errors and 20% type II errors. The sample calculation indicated that at least 10 patients were needed in each group.
In total, 36 patients were selected for the current study. The MMA group comprised 17 patients (14 females, 3 males) with a mean age of 24.18 ± 3.83 years and a mean treatment duration of 34.4 ± 12.8 months. The MMA + VC group consisted of 19 patients (16 females, 3 males) aged 25.00 ± 4.99 years, whose mean treatment duration was 34.7 ± 6.8 months. No significant difference in the patients’ gender, age, or treatment duration was observed between the groups (Additional Table 1).
Cephalometric analysisPre-treatment and post-treatment lateral cephalograms were collected, digitized, and superimposed using the Dolphin 11.0 software (Dolphin Imaging, Chatsworth, CA). An investigator who was not informed about the study’s groups obtained the measurements, which a second blinded investigator checked for accuracy. Any disagreements between these investigators were resolved through a weighted reevaluation until they were both satisfied. The variables used in the cephalometric analysis included skeletal, dental, and soft-tissue-related measurements. In total, 29 such variables were used (8 skeletal, 12 dental, and 9 soft-tissue-related). Figure 2 depicts the landmarks and important variables used in this study, while Additional Table 2 provides definitions.
Fig. 2
Tracing of a pretreatment cephalometric radiograph
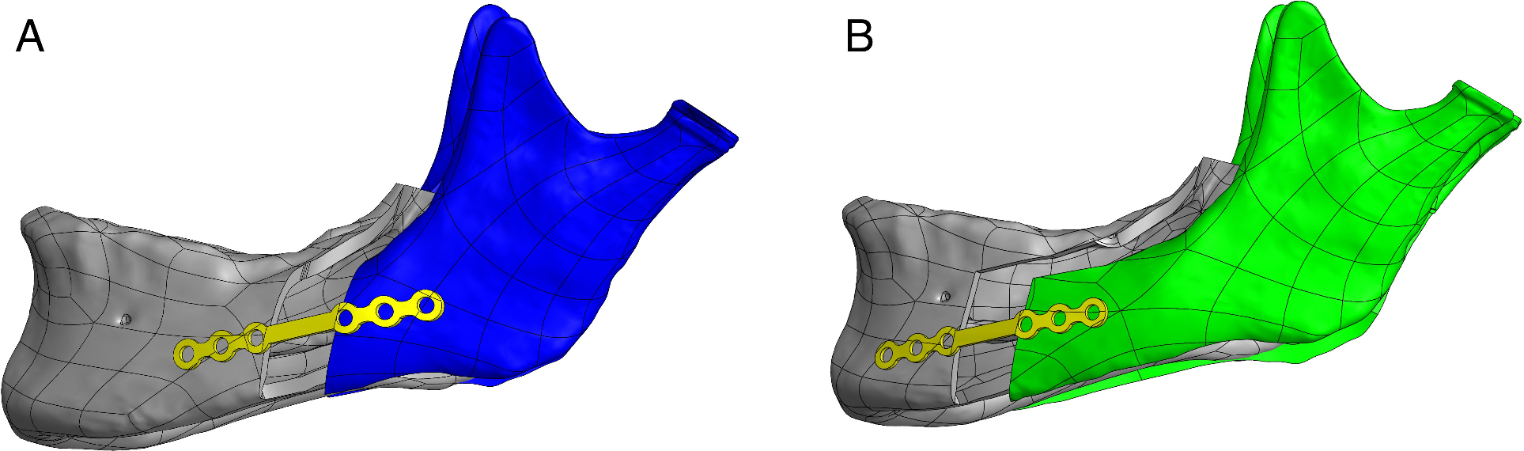
Dental cast analysisPre-treatment and post-treatment dental casts were scanned using a 3Shape scanner (3Shape D, Kopenhagen, Dänemark) and measured in a double-blinded manner by a trained orthodontist using the Geomagic 13.0 software (Geomagic Qualify, Durham, NC, US). As Fig. 3 shows, the superimposition of the dental casts was based on the palate’s stable structure. A coordinate system was built, based on the definition of the anatomical occlusal plane and the midline of the palate. The tooth movements were analyzed in two dimensions, anterior or posterior (X) and intrusion or extrusion (Z). Additionally, posterior and extrusive movement was defined as positive.
Fig. 3
Superimposition of the dental casts. A. The pre-treatment maxillary model. B. The post-treatment maxillary model. C. Superimposition based on the stable structure of the palate. D. Transfer of corresponding landmarks
To evaluate the method’s error, 10 post-treatment lateral cephalograms and digital casts were randomly selected and remeasured by the same examiners two weeks after the first measurement was obtained. The intraclass correlation coefficient (ICC) was used to assess intra-examiner reliability and the reproducibility of all linear and angular measurements.
Statistical analysisThe intraclass correlation efficient (ICC) was evaluated using a two-way random model. Descriptive statistics for the dental casts and radiographic measurements were calculated for both the first and second measurements. Comparisons were performed and correlations were identified using Student’s t test in accordance with the results of Shapiro–Wilk normality tests. The pre-treatment skeletal, dental, and soft-tissue-related variables were compared between the groups using independent-sample t tests. The same variables were also compared from pre-treatment to post-treatment using paired t tests. The differences in treatment changes (concerning both the lateral cephalograms and the dental casts) between the MMA and MMA + VC groups were evaluated using independent-sample t tests. Multiple linear regression analysis was used to test the correlation between the independent variables of craniofacial structures and the dependent variable, the Z angle. Both groups’ differences in treatment changes were normalized to the mean variance. Then, a backward method was used to screen the independent variables. The entry probability of F was 0.05, and the removal criterion was 0.1. The statistical tests were performed with SPSS 18.0 software (IBM Corp., Armonk, NY). The results were considered statistically significant at P < 0.05.
Comments (0)