
Remember me




Falls among inpatients affect health outcomes and are economic issues in hospitals. The incidence of falls is between 700,000 and 1 million patients annually in the United States, and studies have indicated that approximately one third of falls are preventable (Agency for Healthcare Research and Quality, 2023). Aging-related impaired mobility is one of the most well-known risk factors for falls. According to Japan's Ministry of Health, Labour and Welfare, Japan is the world's most super-aged society, with 35% of the population anticipated to be over 65 years old by 2040. The high risk of falls in hospitalized patients due to aging is increasing. Hence, preventing falls is an important and urgent area of risk management for healthcare organizations.
The impact of falls on patient safety has been of interest to nurses since the 1990s. Many studies have developed fall assessment scales and explored the relationship between nurse staffing level and falls. The results of previous studies indicate that higher registered nurse (RN) staffing is associated with lower fall rates (Staggs & Dunton, 2014). Moreover, staffing levels help improve patient fall performance (Cooke et al., 2022). Patient characteristics influencing falls include age and impaired mobility. Moreover, in terms of organizational factors, patients who receive more hours of care from RNs are significantly less likely to fall (Kim et al., 2019). Although many studies have found that better patient outcomes depend on higher nurse staffing levels, drawing robust conclusions between patient outcomes and nurse staffing levels in acute care hospitals has been difficult (Morioka et al., 2022).
Nursing systems in Japan often rely on hospitals and units. Most hospitals apply a team nursing framework in which, although all nurses are assigned specific patients, nursing care for the unit is a collective responsibility. Acute care hospitals generally apply a nurse–patient ratio of either 1:7 or 1:10. Nurse managers may vary this ratio based on unit characteristics. Thus, nurse managers within the team nursing framework must possess control and leadership abilities. Falls are affected by patient characteristics and environmental factors in the unit. Hence, patient safety in preventing falls is easily influenced by unit characteristics in team nursing. The great dispersion in data between administrative and unit-level data emphasizes the importance of unit-level data sources in measuring nursing staffing in healthcare facilities (Spetz et al., 2008). Consequently, evaluating fall-related risks, including those related to unit characteristics, is necessary.
No studies in Japan have examined falls related to unit characteristics such as nursing staffing and nursing hours. Therefore, this study was designed to determine the fall risk factors associated with unit environmental characteristics, nursing staffing, and nursing hours. This study quantified unit activities and utilized Diagnosis Procedure Combination (DPC) data to evaluate unit characteristics related to falls based on unit day.
Methods Data SourcesThe DPC database, which includes the Severity of a Patient's Condition and Extent of a Patient's Need for Medical/Nursing Care (SCNMN) database, the work record notification system (Format 9), and fall incidences reported on the hospital's incidence report system were used as data sources in this study. We linked Format 9 and fall incidence to the DPC data.
Diagnosis procedure combination databaseThe DPC was developed as a case-mix patient classification system for acute inpatient hospitals to make acute care more transparent and visible (Shigemi et al., 2021). This system started as a lump-sum per-diem payment system in 2003 and has been utilized for acute inpatient care and the distribution of medical resources. Many acute hospitals joined the DPC system to report medical information on Japanese Labor and Welfare (Hayashida et al., 2021; Yasunaga et al., 2012). According to the National Ministry of Health, Labor, and Welfare, 1,757 facilities and 483,180 beds in 2020 were included in the DPC system, covering 24.5% of all general hospitals and 54.4% of the medical beds in the country. The DPC data system is unique in terms of including diagnosis, dates of admission and discharge, hospital admission route, hospital discharge route, outcomes at discharge, and surgical procedure information along with international disease classification information for related health problems as defined under the 10th revision code (e.g., patient age, gender, main diagnoses, preexisting comorbidity diagnoses, and postadmission complications; Hayashida et al., 2021; Yamana et al., 2017). Japan's DPC data have already been used in many epidemiological studies (Oku et al., 2021), and using the database to estimate nurse workload is potentially feasible (Kamijo & Kanda, 2008).
Severity of a Patient's Condition and Extent of a Patient's Need for Medical/Nursing CareThe SCNMN is an index originally developed in Japan to measure the nursing care demand of inpatients. The SCNMN is used mainly for the standardization of medication fees, especially basic hospitalization fees for acute care. The SCNMN has been configured into three classifications, with each classification consisting of seven items for a total of 21 items. The three classifications include monitoring and treatment items (used to assess highly specialized nursing care), medical management items (used to evaluate medical treatments related to surgery and emergency care), patient functional status items (including activities of daily living [ADLs], which influence medical care; Hayashida et al., 2022). RNs collect these items daily and enter them into a database.
Work record notification system (format 9)A work record notification system records individual nursing times, excluding overtime. Nursing staffing (nursing time) must be reported as a reference for basic hospitalization fees, which are claimed payments from medical facilities to the government. Format 9 is recorded in a national unification format.
Fall incidenceFrom April 2018 to March 2019, fall cases were extracted from the accumulated incident cases in the hospital's incidence report system. We adopted the definition of fall used by Kennedy: “unintentionally coming to the ground or some lower level other than because of sustaining a violent blow, loss of consciousness, sudden onset of paralysis as in stroke, or an epileptic seizure” (Kennedy, 1987). In this study, fall cases that were not under the hospital's control, such as stay-over falls, duplicated reports, and certifiable disease exacerbation, were excluded from the analyzed data.
Study PopulationThe study population included patients hospitalized at the academic hospital in Japan between April 2018 and March 2019. Patients in pediatric, obstetric, and intensive care units were excluded. The targeted academic hospital had 1,061 RNs with 772 beds as of October 2022.
Variables Patient variablesVariables related to sociodemographic status included age and gender; variables related to patient clinical status included with or without sedative–hypnotics, hypertension, osteoporosis, anemia, comorbidities at hospitalization, and emergency hospitalization. Comorbidities at hospitalization were assessed using the Charlson comorbidity index (CCI) score and calculated using the Quan version (Sundararajan et al., 2007). The variables of the SCNMN were classified into three items: monitoring and treatment, patient functional status, and medical management, for example, medical treatment related to surgery and emergency care. All applicable variables were divided by the number of patients in the units per day to calculate the numeric units per unit day.
Nursing time variableIndividual nursing times during day (8 hours) and night (16 hours) shifts per unit were recorded in Format 9. Nursing time per patient throughout the day and night shifts was calculated as the total nursing shift hours divided by the number of patients under a nurse's charge.
Statistical AnalysesThe following procedures were analyzed: First, chi-squared or Mann–Whitney U tests were used to assess the associations between fall incidence and nonfall incidence and the following variables: sociodemographic status, patients' clinical status, monitoring and treatment, patient functional status, medical management, and nursing time. The finalized variables were selected as significant variables using comparison tests. Finally, logistic regression analysis was performed using these variables as independent variables and fall and nonfall units as dependent variables. The required sample size was not calculated in advance in this study because the reliable effect size (in this case, the proportions and/or the odds ratio [OR]) was not available. Instead, the achieved power was calculated using a post hoc power analysis when no significant difference was found. Statistical analyses were performed using SPSS Version 28 (IBM Corp., Armonk, NY, USA).
Ethical ConsiderationsThis study was approved by the ethical review board of the Graduate School of Medicine, Tokyo Medical and Dental University (approval number: M2018-284).
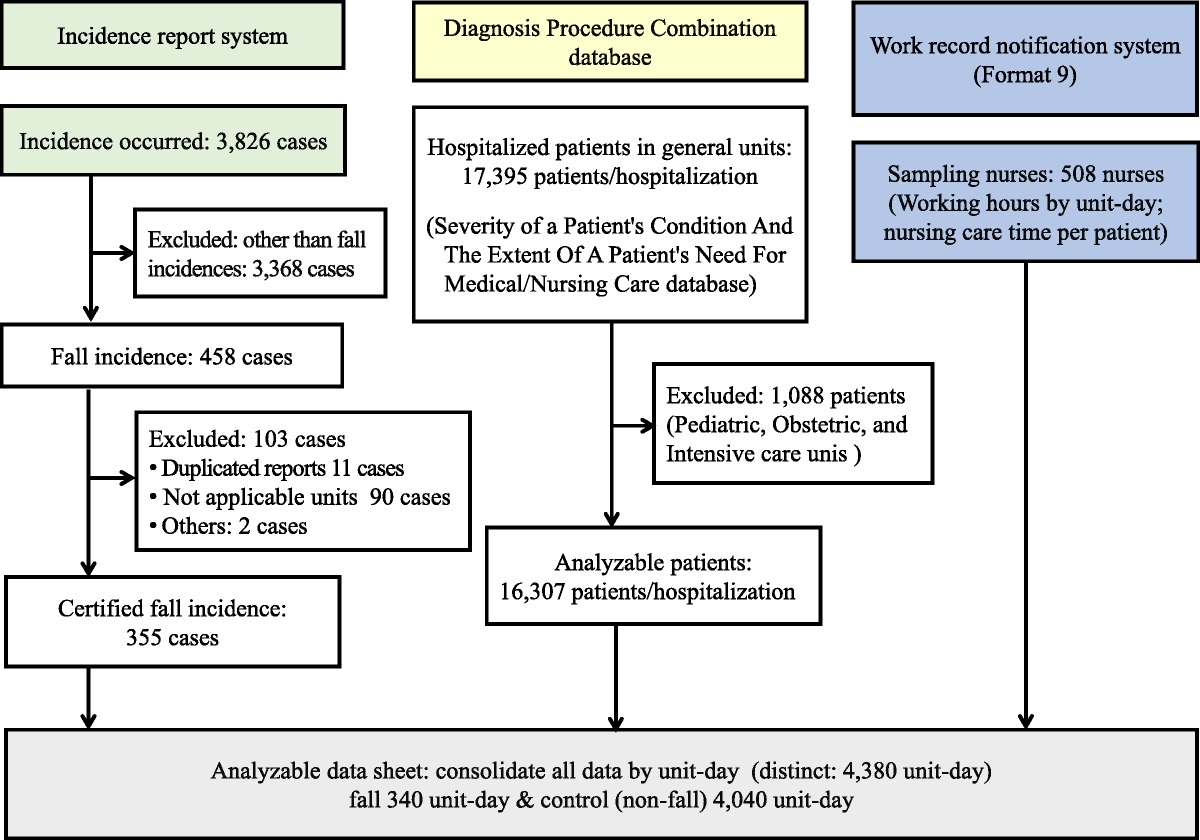
Results Sample DescriptionThis study included 16,307 patients out of the total 168,159 patients in the DPC data (Figure 1). The DPC data were linked to the hospital incidence report and work record notification systems, and 4,380 unit days were extracted. Of the 4,380 unit days, 355 were certified as fall events, with 15 fall cases deducted due to the simultaneous occurrence of two fall event cases per day and unit. Thus, 340 cases were selected as analyzable unit-day fall events. Fall incidence unit days were assigned to the fall group, and nonfall incidence unit days were assigned to the nonfall group. Patient characteristics are presented in Table 1.
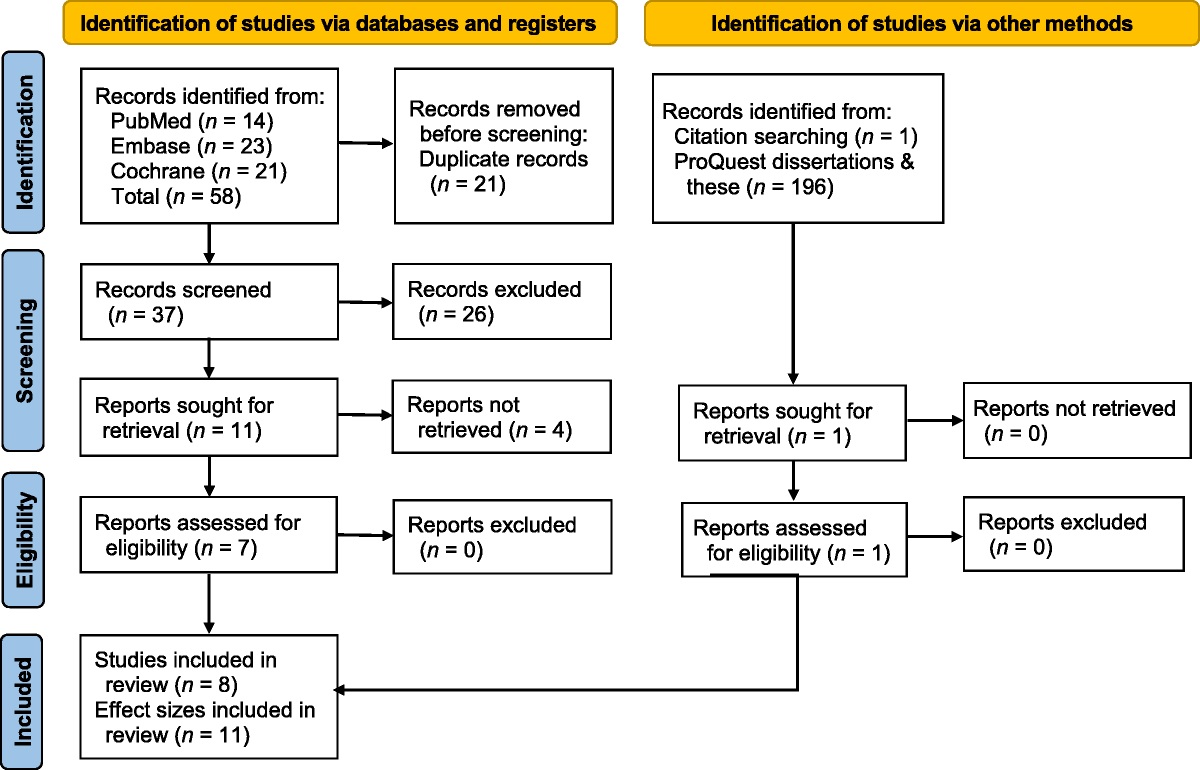
 Figure 1:
Figure 1: Flowchart of the Study Selection Process
Table 1 - Participant Characteristics (N = 16,307) Characteristic n % Male 6,372 39.08 Age (years; mean and SD) 63.90 15.99 Length of stay (day; median and INR) 8 3–15 Hypertension 3,998 24.52 Osteoporosis 688 4.22 Anemia 933 5.72 Hospital in death 321 1.97 Emergency hospitalization 663 4.07 Surgery 2,617 16.05 Eye surgery 1,418 8.70 Fall 355 2.18Note. INR = interquartile range.
Using the nonparametric Mann–Whitney U test, significant differences were observed between fall and nonfall events per unit for the following patient characteristics: sedative–hypnotics, hypertension, anemia, and 1-point CCI (Table 2).
Table 2 - Comparison Between Falls and Nonfalls Based on Unit Characteristics Unit Characteristic Nonfall (n = 4,040) Fall (n = 340) Mann–Whitney U Test Mean SD Mean SD p Nursing time per patient: day shift (8 h), hours 2.33 0.66 2.36 0.57 .10 Nursing time per patient: night shift (16 h), hours 2.02 0.59 1.96 0.48 .16 Hospital in death (rate) 0.00 0.01 0.00 0.01 .33 65 years old and over (rate) 0.62 0.10 0.62 0.10 .94 75 years old and over (rate) 0.32 0.10 0.32 0.09 .73 Emergency hospitalization (rate) 0.00 0.01 0.00 0.01 .77 Surgery (rate) 0.02 0.03 0.01 0.03 .81 Oral medicine (rate) 0.91 0.06 0.90 0.06 .16 Injection (rate) 0.26 0.12 0.27 0.12 .48 Sedative–hypnotics (rate) 0.14 0.07 0.15 0.07 .03 Psychotropic (rate) 0.16 0.07 0.17 0.07 .09 Hypertension (rate) 0.26 0.13 0.24 0.12 .02 Osteoporosis (rate) 0.06 0.06 0.06 0.05 .10 Anemia (rate) 0.11 0.07 0.10 0.06 .00 Eye surgery (rate) 0.03 0.09 0.02 0.07 .38 Charlson comorbidity index score of 0 (rate) 0.41 0.13 0.41 0.14 .67 Charlson comorbidity index score of 1 (rate) 0.21 0.08 0.19 0.08 .01 Charlson comorbidity index score of 2 (rate) 0.16 0.07 0.16 0.07 .55 Charlson comorbidity index score of 3 (rate) 0.11 0.07 0.12 0.08 .22 Charlson comorbidity index score of 4 (rate) 0.05 0.04 0.04 0.04 .24 Charlson comorbidity index score ≥ 5 (rate) 0.02 0.03 0.03 0.03 .47No significant differences were observed based on day of the week or between weekdays and weekends. Furthermore, the comparison test between fall and nonfall identified antineoplastic injections, radiation therapy, aseptic treatment room, and functional status of partly assisted transfers, meals, and oral care as significant patient condition and medical treatment predictors (Table 3).
Table 3 - Comparison Between Falls and Nonfalls by Severity of Patient Condition and Extent of Patient Need for Medication/Nursing Care (SCNMN) per Unit Item of the SCNMN Nonfall (n = 4,040) Fall (n = 340) Mann–Whitney U Test Mean SD Mean SD p Monitoring and treatment Wound treatment 0.06 0.08 0.06 0.07 .75 Respiratory care (except for only sputum aspiration) 0.09 0.08 0.09 0.08 .32 Management of three or more intravenous lines simultaneously 0.06 0.06 0.06 0.06 .25 Electrocardiogram monitor management 0.11 0.13 0.10 0.11 .99 Syringe driver management 0.03 0.03 0.02 0.03 .86 Management of blood transfusion and blood product 0.02 0.03 0.02 0.03 .08 Professional treatment 0.75 0.26 0.75 0.25 .81 Use of antineoplastic agents (injection only) 0.02 0.03 0.03 0.04 .01 Management of oral administration of antineoplastic agents 0.03 0.03 0.03 0.03 .72 Use of narcotics (injection only) 0.03 0.04 0.03 0.04 .12 Internal use of narcotics, application, and management of suppositories 0.03 0.04 0.03 0.04 .31 Radiation therapy 0.02 0.04 0.03 0.04 .00 Immunosuppressant management 0.18 0.13 0.17 0.12 .72 Use of pressor agent (injection only) 0.02 0.03 0.01 0.02 .04 Use of antiarrhythmic agent (injection only) 0.00 0.01 0.00 0.01 .03 Use of continuous infusion of an antithrombotic embolic drug 0.05 0.05 0.04 0.04 .04 Drainage management 0.08 0.09 0.08 0.09 .54 Treatment in a sterile treatment room 0.01 0.05 0.02 0.05 .00 Medical management such as medical treatment to surgery and emergency care Craniotomy (within 7 days from the day of surgery) 0.01 0.02 0.01 0.02 .38 Thoracotomy (within 7 days from the day of surgery) 0.01 0.02 0.00 0.02 .42 Laparotomy (within 4 days from the day of surgery) 0.01 0.01 0.01 0.02 .29 Bone surgery (within 5 days from the day of surgery) 0.02 0.05 0.02 0.04 .75 Thoracoscopic/laparoscopic surgery (within 3 days from the day of surgery) 0.01 0.02 0.01 0.02 .57 General anesthesia/spinal anesthesia surgery (within 2 days from the day of surgery) 0.04 0.05 0.03 0.05 .80 Percutaneous endovascular treatment 0.00 0.01 0.00 0.01 .52 Treatment such as percutaneous myocardial ablation 0.01 0.02 0.00 0.01 .02 Invasive gastrointestinal treatment 0.00 0.02 0.00 0.02 .82 Patient functional status Turnover (without assistance) 0.51 0.22 0.51 0.21 .82 Turnover (partially assisted) 0.37 0.20 0.37 0.20 .53 Turnover (fully assisted) 0.12 0.10 0.12 0.09 .16 Transfer (without assistance) 0.58 0.11 0.57 0.11 .10 Transfer (partially assisted) 0.32 0.10 0.33 0.09 .01 Transfer (fully assisted) 0.10 0.09 0.10 0.08 .93 Oral care 0.39 0.18 0.42 0.20 .03 Meal intake (without assistance) 0.79 0.11 0.78 0.11 .28 Meal intake (partially assisted) 0.13 0.08 0.14 0.08 .01 Meal intake (fully assisted) 0.08 0.09 0.07 0.07 .48 Personal dressing (without assistance) 0.64 0.11 0.64 0.10 .68 Personal dressing (partially assisted) 0.20 0.10 0.20 0.09 .24 Personal dressing (fully assisted) 0.16 0.10 0.15 0.09 .19 Not able to receive directions on medical care and treatment 0.07 0.08 0.07 0.07 .40 Engaged in dangerous behavior 0.03 0.03 0.03 0.03 .39Logistic regression analysis was performed on the significant variables in the comparison tests. Variables with a patient ratio of less than 0.01 and duplicated diagnoses with CCI were excluded. Reduced nursing time per patient during night shifts (OR = 0.75, p = .04) and higher numbers of patients requiring partial transfer assistance (OR = 5.69, p = .01) were found to be significantly related to fall incidence in the unit (Table 4).
Table 4 - Logistic Regression Analysis for the Variables Related to Fall Unit Characteristics (N = 4,380) Variable Β SE OR 95% CI p Lower Upper Nursing time per patient: day shift (8 h) 0.14 0.11 1.15 0.93 1.41 .19 Nursing time per patient: night shift (16 h) −0.29 0.14 0.75 0.57 0.98 .04 Transfer (partially assisted) 1.74 0.64 5.69 1.61 20.04 .01 Oral care 0.71 0.37 2.04 1.00 4.18 .05 Meal intake (partially assisted) 0.10 0.90 1.11 0.19 6.40 .91 Sedative–hypnotics 0.58 0.85 1.79 0.34 9.39 .49 Anemia −1.69 0.94 0.18 0.03 1.17 .07 Charlson comorbidity index score of 1 −0.61 0.83 0.54 0.11 2.74 .46 Use of antineoplastic agents (injection only) 0.30 1.82 1.35 0.04 47.48 .87 Use of continuous infusion of an antithrombotic embolic drug −2.26 1.70 0.10 0.00 2.88 .
Comments (0)