
Remember me
Dear Editor,
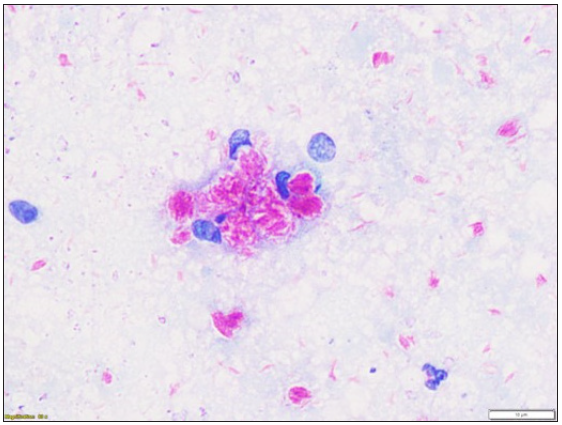
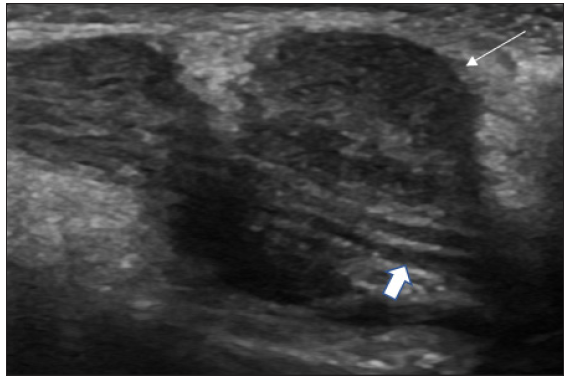
A 55-year-old woman presented with a complaint of four painless swellings on the bilateral wrist areas and right thumb for the last six months. These gradually increased in size with recent ulceration of the swellings on the right side. She denied any history of local trauma, joint pains, tingling/numbness of hands or recurrent oozing. Cutaneous examination showed four well-circumscribed, skin-coloured, firm, non-tender nodules of size 1 × 1 and 0.5 × 0.5 cm (left) and 1 × 1 cm and 0.5 × 0.5 cm (right wrist and thumb, respectively) on the bilateral wrist area around the distal radial border and right thumb [Figure 1]. The overlying skin was not fixed, and the nodules were mobile on lateral movement but fixed longitudinally. The nodules on the right side had a small ulcer of size 4 mm2 and 2 mm2 with thin brownish crusts. On further detailed examination, a linear rope-like structure could be palpated in continuation with the nodules. In addition, diffuse infiltration of the face, including bilateral earlobes, skin-coloured papules on the upper limbs and trunk and a glove-and-stocking pattern hypo-aesthesia were noted. The differential diagnoses of ganglion cyst, giant cell tumour of the tendon sheath (GCTTS), and epidermoid cyst were considered, and a fine needle aspiration cytology (FNAC) was done. FNAC revealed foamy macrophages containing clumps of acid-fast-bacilli (AFB) on Ziehl Neelsen (ZN) staining [Figure 2]. High-resolution ultrasonography (HRUS) of nerves showed nodular thickening of the right radial cutaneous nerve proximal to the wrist joint over a length of approximately 6 cm. The maximum diameter of the nerve was 15 mm. The nerve fascicles were swollen and appeared heterogeneously hypoechoic, surrounded by the echogenic perineurium and epineurium. Focal outpouchings were also noted arising from the nerve [Figure 3]. Colour Doppler evaluation showed mildly increased vascularity suggestive of subclinical neuritis. Similar features were noted in the nodular thickening of the left radial cutaneous nerve. The nerve conduction study was consistent with peripheral demyelinating sensorimotor neuropathy. Slit skin smear from bilateral ear lobes was positive with a bacteriological index of 4+ and morphological index of 50%. A skin biopsy was not done as the patient didn’t consent for the same. A diagnosis of lepromatous Hansen’s disease with silent neuritis was made, and MB-MDT (multibacillary multi-drug therapy) was started.

Export to PPT
Export to PPT
Export to PPT
Swellings at the wrist can have various etiologies. The common causes are non tumoural swellings such as ganglion cysts and implantation cysts. The others are localised nerve thickening, pseudo-neuroma, giant cell tumour of the tendon sheath (GCTTS) and bone tumours such as enchondroma.1 Hansen’s disease is a chronic mycobacterial infection caused by Mycobacterium leprae. It primarily affects skin and peripheral nerves resulting in various skin lesions and sensory-motor peripheral neuropathy and rarely can cause localised nerve swellings. Multiple reports of localised nerve swellings secondary to abscesses with leprosy infection are there in the literature but such large nodular nerve thickenings without abscess formation are not reported.2,3 FNAC4 and high-resolution HRUS5 can be of diagnostic help in revealing AFB on special staining and nerve thickening/abscess formation, respectively.
In conclusion, we report this unusual presentation of lepromatous leprosy as bilateral asymptomatic nodular swellings at the wrist. In the era of leprosy elimination, this can be easily missed and can be misdiagnosed.
Comments (0)