
Remember me
Nail unit squamous cell carcinoma (nSCC) represents a relatively unusual cutaneous squamous cell carcinoma variation that requires prompt diagnosis and appropriate surgical treatment. Traditionally, amputation was the standard therapy for nail unit malignancies.1 While amputation provides significant local control, it also causes remarkable physical and cosmetic damage, particularly in finger lesions. In recent years, researchers have demonstrated that functional surgery is a reliable therapeutic option that provides better function and cosmetic benefits than amputation. This is especially true in cases with nSCC without bone invasion. Functional surgery may provide successful management of minimally invasive tumours in the absence of additional negative prognostic factors. This systematic review of current studies summarises the local recurrence rates following functional surgery and amputation respectively, in nSCC without bone involvement.
Methods Eligibility criteria for inclusion and exclusionThe goal of this systematic review was to assess whether functional surgery or amputation is the better option for nSCC not involving the bone. Thus, the primary outcome of this study was local recurrence, and the secondary outcomes were metastasis or death related to this disorder. Complete text evaluation of all accessible papers was done through the implementation of specific criteria. We did not find any randomised controlled experiments; thus, observational study designs (retrospective studies and case series) with a minimum of 5 patients with nSCC were selected. Only those studies were included which described the histopathologic diagnosis of nSCC (in situ or invasive) as well as prognostic data (average 6 months of follow-up and outcomes such as recurrence, metastasis, or death caused by the nSCC).
Squamous cell carcinoma of the nail unit was defined as squamous cell carcinoma that originated from any component of the nail unit, which comprises the nail bed, nail matrix, nail groove, nail fold, and periungual skin. Functional surgery included Mohs micrographic surgery, wide surgical excision, local surgical excision, as well as other functional surgical modalities. Results were defined as metastasis, death, local recurrence, or persistent disease as described by the studies. Disease was classified as persistent when positive margins were reported after treatment. Squamous cell carcinomas growing at other sites of the body and articles that did not differentiate between nSCC and other tumours of the nail apparatus were excluded. Repeated publications, as well as studies in which data relevant to our interests could not be extracted, were removed [Table 1].
Table 1: Criteria for inclusion and exclusion of studies includes participants, interventions, comparators, outcomes, time, setting, and study designs (PICOS-SD)
Parameters Inclusion criteria Exclusion criteria Participants Studies include a minimum of 5 subjects who were diagnosed with localised/invasive nSCC through histopathology.1. Studies without histopathology confirming nSCC.
2. Data on nSCC in studies are reported as part of the overall data and cannot be isolated.
Interventions Articles reporting functional surgery or amputation at any level.1. There are no precise details of surgical techniques.
2. Participants who did not have prior therapy or had a combination of treatments were indistinguishable from the whole sample.
Comparators None None Outcomes Any local recurrence, metastasis, or related death.1. Studies lacking information on recurrence.
2. Results by stage & operational procedures were unable to be isolated from the overall dataset.
Time Average follow-up time of more than 6 months Average follow-up time less than 6 months Setting Any setting None Study designs Any study design Review articles, letters to editors, comments, posters, abstracts only, meeting reports. Procedures for searching the literatureWe conducted a comprehensive search strategy following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) and MOOSE (Meta-analyses Of Observational Studies in Epidemiology) guidelines. A search of the literature was carried out using Pubmed, Embase, Cochrane Library, Web of Science, and Scopus from inception until February 23, 2023. The search terms used in these databases were “nail” / “nail unit” / “subungual” / “ungual” and “squamous cell carcinoma” / “epidermoid carcinoma” and “Mohs surgery” / “wide excision” / “amputation” / “local excision” / “functional” / “treatment” / “surgery” / “en bloc excision” and “recurrence” / “death” / “metastasis” / “survival.”
Study selectionThe preliminary retrieved results were transferred from each database into Endnote. The results were then combined, and repetitions were discarded. The retrieved papers’ titles, abstracts, as well as publication types, were reviewed to determine whether to include them during the complete text evaluation. Articles that were not in English and non-human studies were excluded. We also excluded studies that did not focus on nSCC, as well as publications with unsuitable designs, which included review articles, commentaries, letters, and those with abstracts only.
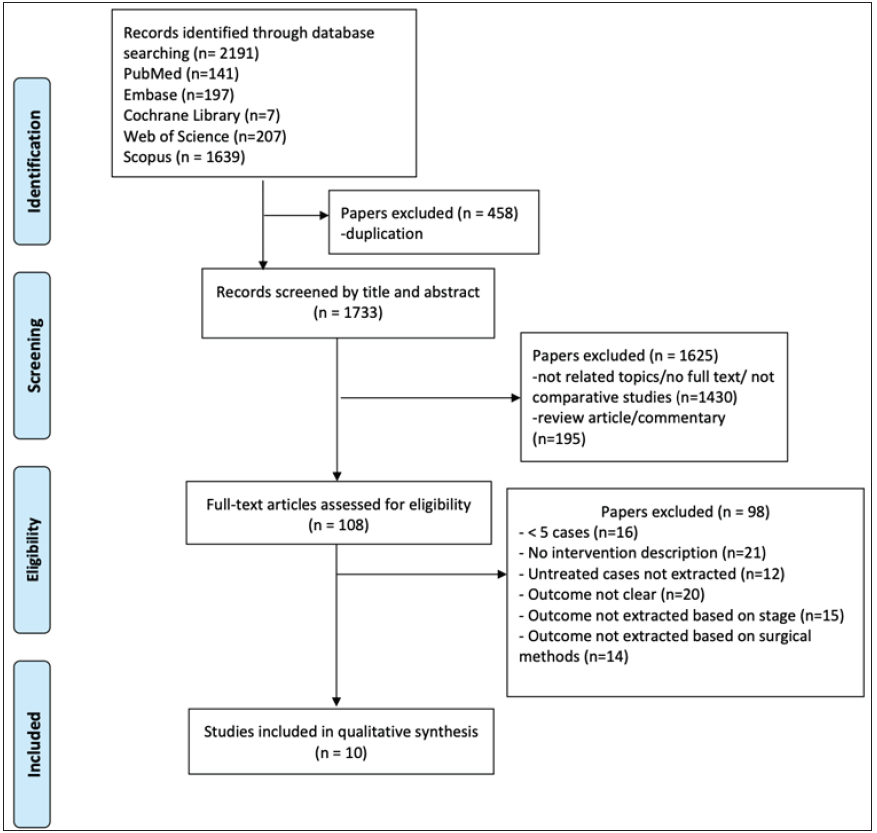
Data extraction processThree investigators (HS.W., F. L., and JY.J.) independently reviewed the titles and abstracts of the included publications before evaluating the complete articles for eligibility [Figure 1]. Following inclusion, the three authors (HS.W., F.L. and SD.H.) independently retrieved data on the treatment method, recurrence, and follow-up duration. Any disagreements were handled via a consensus meeting with the third investigator (DG.W.). Following inclusion, information gathered from every article was retrieved and subcategorized, encompassing the year of publication, period, number of patients, age, gender distribution, tumour stage, kind of intervention, number of recurrences, and follow-up duration.
Export to PPT
Risk of bias and quality assessmentThe risk of a bias assessment tool for non randomised studies (RoBANS) was applied to evaluate the bias of the 10 included studies.2 As all 10 studies were retrospective and non randomised in nature, we preferred using the RoBANS tool which is designed for non randomised studies. This tool is comprised of six domains: the selection of participants, confounding variables, measurement of exposure, blinding of the outcome, incomplete outcome data, and selective reporting.
Results Literature search and study characteristicsFigure 1 shows the systematic search procedure step by step. From a total of 2191 studies retrieved from 5 databases, we finally included 10 studies with a total of 319 lesions [Table 2]. All the included studies were non randomised and published between 1992 and 2020. Seven were retrospective studies and three were case series. Three studies came from the United States, five from Europe, and one from each Asia and Australia.3-12 All 10 investigations described the clinical and pathological characteristics of nSCC, with subungual hyperkeratosis being the most frequently reported presentation. Nail squamous cell carcinoma was suspected in about 38 cases before definite diagnosis and the remaining patients were often misdiagnosed and managed as onychomycosis and viral warts.4-6,12 Functional surgery was more commonly reported than amputation, with Mohs micrographic surgery being the most reported surgical modality. The number of studies was inadequate for comparing their outcomes based on each surgical modality.
Table 2: Characteristics of included studies
Article Study Type N Mean Age (Range), yearsSex
F/M
Location, Hand/Foot Mean Time to Diagnosis (Range), mo. Staging Treatment Modality (N) Mean Follow-up (Range), mo. Recurrence Goldminz et al., 1992, USA3 Case series 25 61 (19–94) NR NR 60 (3–180) 2is, 23I MMS (25) 60 (12–144) 2/25->MMS Dalle et al., 2007, France4 Retrospective 35 NR (25–85) 10/25 28/7 NR (2–84) 4is, 31ILSE (9)
WSE (20)
DA (6)
33 (4–90)5/9 ->WSE
1/20 ->LSE
1/6->DA->died
Young et al., 2012, Australia5 Case series 12 (13nSCC) 49 (32–75) 4/8 13/0 57(18–168) 11is, 2I MMS (13) 51.5 (2–120)1->MMS->Topical imiquimod->MMS
1->DA
1->MMS
Lecerf et al., 2013, Belgium6 Retrospective 25 (27nSCC) 60 (21–80) 7/18 26/1 NR 11is, 16IDA (2)
Partial ablation (3)
En bloc ablation (14)
LECM (8)
40 (4–177)1/2 ->NR
0/3
5/14 ->NR
2/8 ->NR
Wollina et al., 2015, Germany7 Case series 8 (9nSCC) 60 (40–84) 2/6 6/3 9 (NR) 9is, 0I MMS (9) NR (48–60) 2->MMS Dika et al., 2015, Italy8 Retrospective 57 63 (26–89) 18/39 49/8 30 (NR) 7is, 50IMMS (43)
DA (12)
NR2/43->DA
0/12
Tang et al., 2016, USA9 Retrospective 33 (39 nSCC) 63 (33–92) 7/26 36/3 39 (3–360) NRDA (3)
MMS (35)
WSE (1)
NR (5–48)0/3
3/35->MMS, radiotherapy, DA
0/1
Topin-Ruiz et al., 2017, France10 Retrospective 55 64 (35–90) 23/32 39/16 34 (2–182) 6is, 49I WSE (55) 78 (60–134)1->WSE
1->WSE->DA
Lee et al., 2019, Korea11 Retrospective 17 61 (36–80) 5/12 12/5 62 (4–264)4is,
13I
MMS (8)
LSE (4)
WSE (1)
DA (4)
31 (5–75)0/8
2/4->LSE, NM
0/1
0/4
Gou et al., 2020, USA12 Retrospective 40 (42 nSCC) 61 (33–92) 6/34 38/4 24 (1–240) 24is,18IMMS (38)
MMS->DA (4)
45 (3–144)3/38->MMS
0/4
In total, all studies included 282 individuals, 82 females, and 200 males. The average age of these patients was 60 years. The duration from the discovery of the lesions to the diagnosis of nSCC ranged from 1 to 360 months. Most (247 lesions) were on the hand, and 47 lesions were on the foot. More than one digit were affected simultaneously in 4 cases. Two of these had 3 digits affected, while the other two had 2 digits affected.5-7,12 One of them was reported to have xeroderma pigmentosum.12 While 78 lesions were reported to be in situ and 202 were invasive, 1 study did not specify the degree of invasiveness.9 Only 1 study reported distant metastasis and death.4 The duration for post-surgical follow-up ranged from 2 to 177 months. There was a 12% overall recurrence rate, with a total of 34 recurrent cases. Post-surgical outcomes for each surgical modality were described.
Risk of biasThe risk of bias assessed by RoBANS indicates that all 10 articles have an overall low risk of bias. The section on incomplete outcome data was reported high for the study by Lecerf et al. because they did not describe the mean time to diagnosis. The confounding variable was rated high in the study by Topin-Ruiz et al. due to a preference of surgical modality [Table 3].10
Table 3: Risk of bias based on the Risk of Bias Assessment Tool for Non randomised studies (RoBANS)
Study Selection of participants Confounding variables Measurement of exposure Blinding of outcome Incomplete outcome data Selective reporting Goldminz et al., 1992, USA3 Low Low Low Low Low Low Dalle et al., 2007, France4 Low Low Low Low Low Low Young et al., 2012, Australia5 Low Low Low Low Low Low Lecerf et al., 2013, Belgium6 Low Low Low Low High Low Wollina et al., 2015, Germany7 Low Low Low Low Low Low Dika et al, 2015, Italy8 Low Low Low Low Low Low Tang et al., 2016, USA9 Low Low Low Low Low Low Topin-Ruiz et al., 2017, France10 Low High Low Low Low Low Lee et al, 2019, Korea11 Low Low Low Low Low Low Gou et al, 2020, USA12 Low Low Low Low Low Low Treatment based on surgical modality Mohs micrographic surgeryA total of 171 nSCC lesions from 7 studies were treated by Mohs micrographic surgery [Table 4].3,5,7-9,11,12 Among these lesions, 49 lesions were in situ cases, and 48 lesions were invasive nSCC. Invasiveness for the remaining lesions could not be extracted from the whole data for 2 studies.8,9 A majority of the lesions affected the fingernails. Fifteen cases recurred, resulting in an overall reported recurrence rate of 9%. The mean duration for the recurrence of disease after Mohs micrographic surgery was 39 months. Among the recurrent cases with reported pathology, 4 cases were reported to recur as in situ nSCC, while 1 as invasive nSCC.5,7 The remaining studies did not describe the type of recurrence. Ten of the recurrent cases were treated with repeated Mohs micrographic surgery, 4 underwent amputation, and 1 underwent radiotherapy. One of the persistent (positive margins reported after treatment) cases recurred after Mohs micrographic surgery and topical imiquimod, which was later cleared after a third intervention by Mohs micrographic surgery. Meanwhile, a study treating 1 in situ and 7 invasive cases with Mohs micrographic surgery did not report any recurrences.11 None of the cases metastasized. However, the periosteal invasion was discovered in 9 cases during Mohs micrographic surgery, where 4 underwent amputation, and the remaining 5 were treated with curettage of the periosteum and close follow-up.8,12
Table 4: Details of studies reporting Mohs micrographic surgery
Article In situ/ Invasive Location Treatment Modality (N) [MMS Stages] Defect reconstruction Recurrences Time to recurrence (months) Goldminz et al., 1992, USA3is (2)
I (23)
NR MMS (25) [NR] SIH (25) 2/25-> MMS 12; 132 Young et al., 2012, Australia5Is (11)
I (2)
R1H (3) R3H (3)
R4H (1) L2H (2) L3H (2) L4H (1)
L5H (1)
MMS (13)
[1–3, mean two]
SIH (12)
primary closure (1)
1->MMS->Topical imiquimod->MMS
1->DA
1->MMS
13; 30; 96 Wollina et al., 2015, Germany7 is (9) R4H (1) R2H (1) R3 (2) R5 (1) L1F (1), L5F (1) 2 NR MMS (9)5STSG
3FTSG
1SIH
2->MMS 24; 36 Dika et al., 2015, Italy8 NR 1st fingernailMMS (43)
[1–4, mean, 3.2]
Hyalofill-F+SIH 2/43->DA 12, 18 months Tang et al., 2016, USA9 NRFingernails
R3 most common
MMS (35) NR3/35->1 MMS
1->radiotherapy
1->DA
NR Lee et al., 2019, Korea11is (1)
I (7)
R1H (2) R2H(1)
R4H(2)
L1H (1)
L3F (1)
R5F (1)
MMS (8) NR 0/8 0 Gou et al., 2020, USA12is (26)
I (16)
H (38/42)MMS (38)
MMS->DA (4)
[1–4, mean 1.8]
19 FTSG, 10SIH, 3STSG, 4 DA, 1nail bed graft, 1NR
(2 patients had extensive and continued tobacco use, and the other 2 had exposure of the periosteum.)
3/38->MMS
0/4
5; 8; 79Following Mohs micrographic surgery, 30 cases were closed by skin grafts, 1 by primary closure, 91 by secondary intention healing, and 1 by splint nail bed graft. Four cases further underwent phalanx amputation because of prolonged smoking history and periosteum exposure.12 Reconstruction data were unavailable for 44 lesions. Of the skin grafts, 22 were full-thickness skin grafts (FTSG) and 8 were split-thickness skin grafts (STSG). In one study the defects were repaired with hyaluronic acid followed by secondary intention healing; 60% of these patients reported subsequent nail dystrophy.8 The number of stages required for histological clearance was described in 3 studies, with an average of 2 stages, ranging from one to four stages of Mohs micrographic surgery.5,8,12 Only 1 study described the number of tissue sections required, with an average of 4 sections.5 One study reported discovering 5 cases of periosteal invasion during Mohs micrographic surgery although X-rays did not show any abnormalities.8 Post-surgical cosmetic and functional evaluations after Mohs micrographic surgery were reported in 1 study, with an overall high satisfaction rate.5 Dysesthesia was reported in 3 cases as the most common late complication in another study.12
Wide surgical excisionFive studies evaluated the outcome of wide surgical excision for nSCC not involving the bone, representing 91 lesions [Table 5].4,6,9-11 The fingernails were the most common site affected. Depth of invasion was described in 4 studies, with 14 in situ cases and 74 invasive cases. Two cases were described as microinvasive because of the difficulty in determining tumour cells invasion of the papillary dermis.6 One report used the term ‘en bloc ablation’, which specified the excision of a nail unit with 6-mm margins.6 This study also included a case of polydactylous nSCC which affected 3 digits simultaneously.
Table 5: Details of studies reporting wide surgical excision
Article In situ/ Invasive Location Treatment Modality (N) Defect reconstruction Recurrences Time to recurrence (months) Dalle et al., 2007, France4is (3)
I (17)
R1H(7) R2H(2)
R4H(2)
L1H(3)
L2H(2)
L5H(1)
R1F(2)
L1F(1)
WSE (20) FTSG (20) 1/20 ->LSE 36 Lecerf et al., 2013, Belgium6is (5)
Microinvasive (2)
I (7)
R1H(2)
R2H(2)
R3H(1)
R4H(3)
L1H(1)
L2H(2)
L3H(1)
L5H(1)
R1F(1)
En bloc ablation with 6-mm margins (14) NR 5/14 ->NR 36; 58; 58; 46; 8 Tang et al., 2016, USA9 NR NR WSE (1) NR 0/1 Topin-Ruiz et al., 2017, France10is (6)
I (49)
L1H(12)
R1H(11)
R1F(8)
WSE (55) FTSG (55)2/55
1->WSE
1->WSE ->5 months ->DA
7; 8 Lee et al., 2019, Korea11 I (1) L1H (1) WSE (1) NR 0/1In two studies FTSG was performed after wide surgical excision, while the other 3 studies did not mention the reconstruction method.4,10 There was a 9% recurrence rate following wide surgical excision, with 8 cases recurring after an average of 32 months after the first surgery.4,6,10 Six of these cases had clear histological margins reported after the initial surgery, 1 did not have clear margins, and margins were not mentioned in 1 case. Five of the recurrent cases were invasive nSCC, 1 was microinvasive, and 2 were in situ nSCC. One of the relapses occurred adjacent to the graft and was treated with local surgical excision.4 Another 2 recurrent cases were further treated by wide surgical excision, in which 1 persistent disease later underwent amputation.10 One study did not mention the treatment after recurrence.6 Post-surgical patient satisfaction was assessed only in 1 study, with overall high satisfaction.10
Digital amputationA total of 6 studies with 31 cases reported amputation performed [Table 6].4,6,8,9,11,12 Two of the cases were in situ nSCC, while 14 were invasive, and one study did not describe invasiveness.9 Fingernails were the most common site. Six cases were reported as partial amputation, whereas 4 cases were initial Mohs micrographic surgery cases that failed to obtain clear margins.4,12 Recurrences were seen in 2 cases of amputation, with a recurrence rate of 6%.4,6 One of the patients died after metastasis to the lungs. This was an in situ nSCC that recurred at the stub 2 months after initial partial amputation and the patient subsequently underwent complete amputation.4 Another case recurred 19 months later but the treatment for recurrence was not described.6 Amputations were usually performed in bone-invasive cases that were evidenced from radiology, however, 2 cases of amputation were performed because of patient preference and treatment convenience.6
Table 6: Details of studies reporting digital amputation
Article In situ/ Invasive Location Treatment Modality (N) Recurrences Time to recurrence (months) Dalle et al., 2007, France4is (1)
I (5)
R1H(1); R4H(1); L1H(1); L2H(1); L3H(1); L1F(1) DA (6) 1/6->DA->died 2 Lecerf et al., 2013, Belgium6is (1)
I (1)
R2H(1)
L2H(1)
DA (2) 1/2 ->NR 19 Dika et al., 2015, Italy8 NR NR DA (12) 0/12 NR Tang et al., 2016, USA9 NR NR DA (3) 0/3 Lee et al., 2019, Korea11 I (4) L1H(1); L4H(1); R5F(2) DA (4) 0/4 Gou et al., 2020, USA12 NR NR MMS->DA (4) 0/4 Other surgical modalitiesThree studies described three alternative methods of functional surgery that cannot be included in wide surgical excision or Mohs micrographic surgery [Table 7].4,6,11 Eight cases with in situ nSCC were treated by limited excision until clearing of margins (LECM). The authors described the complete excision of the defect and obtaining clear margins by evaluating the lateral and deep margins.6 Two of the cases after LECM recurred after 19 and 14 months after clear marginal excision, further treatment was not described. Partial ablation was described in 3 cases, and no recurrences were reported.6 Seven of the 13 cases that were treated by local surgical excision relapsed after an average of 17 months, giving a recurrence rate of 54%.4,11 Five of the cases underwent wide surgical excision, 1 repeated local surgical excision, and 1 was not reported.
Table 7: Details of studies reporting other functional surgeries
Article In situ/ Invasive Location Treatment Modality (N) Recurrences Time to recurrence (months) Lecerf et al., 2013, Belgium6LECM:
is (5)
I (3)
Partial ablation:
I (3)
LECM:
R3H(2); R4H(1); L1H(2); L2H(2); L3H(1)
Partial ablation:
R1H(1); R3H(1); L1H(1)
LECM (8)
Partial ablation (3)
2/8 ->NR
0/3
14
19
Dalle et al., 2007, France4 I (9) R1H(1); R2H(1); R3H(1); L1H(2); L3H(1); L5H(1); R1F(1); L1F(1) LSE (9) 5/9 ->WSE 6; 36; 6; 16; 7 Lee et al., 2019, Korea11is (3)
I (1)
R5H(1); L2H(1); L3H(1); R1F(1) LSE (4) 2/4->1 LSE, 1 NR 43; 4 DiscussionThe nail apparatus has a rather complex anatomical structure. A good understanding of its structure is required to diagnose and manage entities involving this organ. Malignant nail tumours are typically rare with nSCC being the most common carcinoma reported. When nSCC is present, the nail unit might appear in a variety of clinical presentations. Despite being the most prevalent malignant subungual tumour, nSCC is frequently misdiagnosed as an innocuous condition like onychomycosis, verruca vulgaris, or trauma-induced nail dystrophy.13 Middle-aged males are more likely to be affected, and the hand is the most commonly reported area.4 A high level of suspicion is therefore required when addressing a nail condition to avoid a delay in diagnosis, which may complicate therapy and significantly affect the prognosis. While metastasis and mortality are uncommon in nSCC, early biopsies of chronic non-healing and persistent lesions may merit a better prognosis.4 Clinicians in practice should therefore be aware of benign-presenting nail lesions that do not improve with appropriate management and should suggest that patients undergo nail biopsies when applicable.
Functional procedures, such as Mohs micrographic surgery and wide surgical excision, were routinely tested to establish the best first-line treatment for nSCC. However, the existing research does not recommend a specific therapeutic strategy as the first line of therapy. Studies conducted over the last decade have shown that more conservative approaches for nSCC management are preferable to traditional amputation. These authors believe that traditional amputations may result in functional problems, undesirable cosmetic results, and possibly psychological distress. This is particularly noticeable in the amputation of the thumb, which accounts for about 40% of the hand’s normal function.14 Further, the patient may experience loss of sensation at the amputated site, unusual pains, excessive sensitivity, and difficulties when gripping small items, which may interfere with daily tasks.8,15
Mohs micrographic surgery has the advantage of eliminating the tumour with histological confirmation of the actual extent of malignancy, as well as removing the diseased tissue while preserving its normal structure.3,12,16 Preserving the viable tissues of the finger to the greatest extent feasible is critical for a functioning digit.8 However, imaging methods typically fail to detect the depth of nSCC invasion. Mohs micrographic surgery can detect periosteal invasion and accurately differentiate bone invasion from inflammation or compression.8,12 In general, Mohs micrographic surgery
Comments (0)