
Remember me
Anterior cervical diskectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) are the most common surgical procedures in the field of spinal surgery. Since the introduction of these procedures in 1958 by Smith and Robinson, ACDF and ACCF have been widely accepted in treating patients with symptomatic myelopathy or radiculopathy after cervical spondylosis.1,2
Most ACCF/ACDF surgeries result in good clinical outcomes. Owing to the large number of clinical series of successful ACCF/ACDF patients, there may be a misconception that ACCF/ACDF surgeries are risk-free procedures. On rare occasions, though, complications could arise and cause inconvenience or even death. As high as 79.7% of implant failure and 25% of ASD have been reported in the literature after ACDF or ACCF, with 6 to 17% requiring revision surgery.3–5 Furthermore, despite having undergone ACCF or ACDF surgery, some patients continue to experience a decrease in their functional abilities for reasons that are not fully understood. There is a shortage of research in the literature about the patient or surgical factors that predispose patients to additional functional decline. Since preventing additional decline is one of the main goals of surgical decompression, the knowledge of these factors may be useful in guiding surgical management and discussions with patients who are undergoing ACCF/ACDF surgery.6 The proper alignment of bone structures and joints is essential for the musculoskeletal system to operate properly. Furthermore, ergonomic balance and deliberate displacement of the human body require a complex interaction of the neurologic system and muscular recruitment. Therefore, it is essential to recognize that optimal spinal alignment permits an individual to assume a standing position with minimal muscular energy.7
Recent surgeons have focused on the role of sagittal balance in cervical spine disorders and the potential role of imbalance in predicting clinical and functional outcomes.8
However, our present understanding of cervical sagittal alignment (CSA) is broader and more nuanced. The normative parameters of the cervical spine have not been fully defined, and what constitutes a normal parameter for a given individual is even less clearly defined. There is no conclusive agreement on the definitive alignment of the parameters that are notable in forecasting the prognosis of patients both preoperatively and postoperatively.9
In this article, we hypothesize that “the cervical sagittal alignment is different in patients who have undergone ACCF or ACDF surgery, followed by failure, and consequently revision surgery, compared to patients who have not undergone revision surgery”.
The goal of this study was to assess the difference in CSA parameters between revision and nonrevision surgery patients after ACCF or ACDF surgeries, as well as the effect on patient's quality of life; moreover, to ascertain which cervical sagittal parameters are the most sensitive in predicting positive clinical outcomes after ACCF/ACDF surgeries in patients with symptomatic myelopathy/radiculopathy; and furthermore, to create an equation model that will guide the surgeon in decision making and counseling the patients on the outcome of quality of life after cervical fusion surgery.
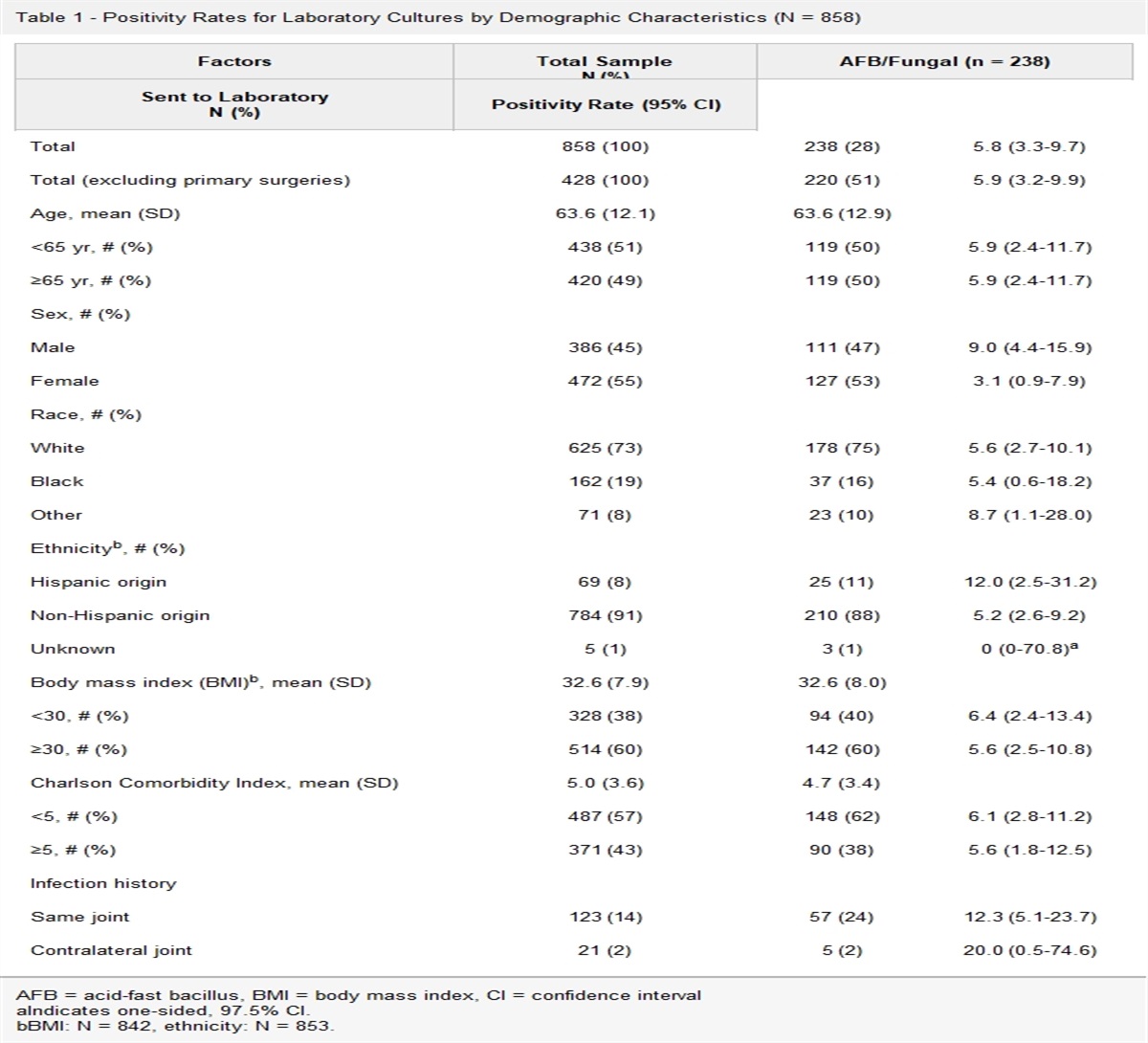
MethodsFrom January 2010 to January 2022, 110 patients with symptomatic myelopathy/radiculopathy who underwent cervical fusion through ACCF or ACDF were consecutively collected from the hospital database. Eleven patients' radiographic images and other additional follow-up data were missing. Therefore, 99 patients (65 male and 34 female) were eligible for this study. Patients were divided into two groups (A and B). Patients in group A underwent revision surgery after the first surgery failed, whereas patients in group B underwent surgery with the same surgeon as patients in group A without failure. Data were retrieved from the medical records. The demographic data of the patients are summarized in Table 1, https://links.lww.com/JAAOS/B16.
Inclusion Criteria Weakness, pain in the neck and shoulder, upper limb numbness, impaired muscle tone, or signs and symptoms of peripheral nerve injury after excluding other systemic diseases Hyperreflexia hypertonia, positive pathological signs, and symptoms of upper motor neurone injury Patients with a follow-up period of more than 2 years with complete radiographic data Adult patients (>18 years old) Exclusion Criteria Patient with incomplete radiographic images Patients missing during follow-up Patients with cervical tumor or other cervical diseases Patients with a history of revision surgery due to cervical trauma Indication for Revision Surgery in Group AWe defined ACCF/ACDF failure for cases in group A with the help of postoperative history, physical examination, imaging, and laboratory tests as follows.
History and Physical ExaminationThe occurrence of postoperative signs or symptoms of myelopathy, radiculopathy, increasing weakness, weight loss, fever, nausea, or vomiting was all indicators of failure, requiring immediate medical intervention.
ImagingPlain radiographs helped to reveal implant failures such as screws or rod breakage, while lucencies surrounding screws indicated pseudarthrosis. Dynamic radiography also helped in the evaluation of motion and fusion at the surgical site. A CT scan helped to provide exquisite bone details and allowed for a more accurate assessment of fusion status. Magnetic resonance imaging revealed details on disk integrity, neural elements, bony structures, and surrounding soft tissue structures. In addition, magnetic resonance imaging helped to distinguish between scar tissue, disk tissue, and fluid collections, which could suggest infection.
Laboratory TestingConcerns for infection were evaluated at every time point after surgery using erythrocyte sedimentation rate, C-reactive protein, and complete white blood cell count with differentials.
The indication for revision surgery included implant failure 15 cases, adjacent segment disease (ASD) 28 cases, both implant and ASD 2 cases, infection 3 case, and hematoma 1 case (Table 2, https://links.lww.com/JAAOS/B17).
Data CollectionsEach patient's demographic information, radiologic measurements, and health-related quality of life were collected. Demographic data included patient age, sex, body mass index, disease duration, occupation, smoking status, and other comorbidities (Table 1, https://links.lww.com/JAAOS/B16). Health-related quality of life (HRQOL) outcomes included Neck Disability Index and Modified Japanese Orthopaedic Association Scale (mJOA).
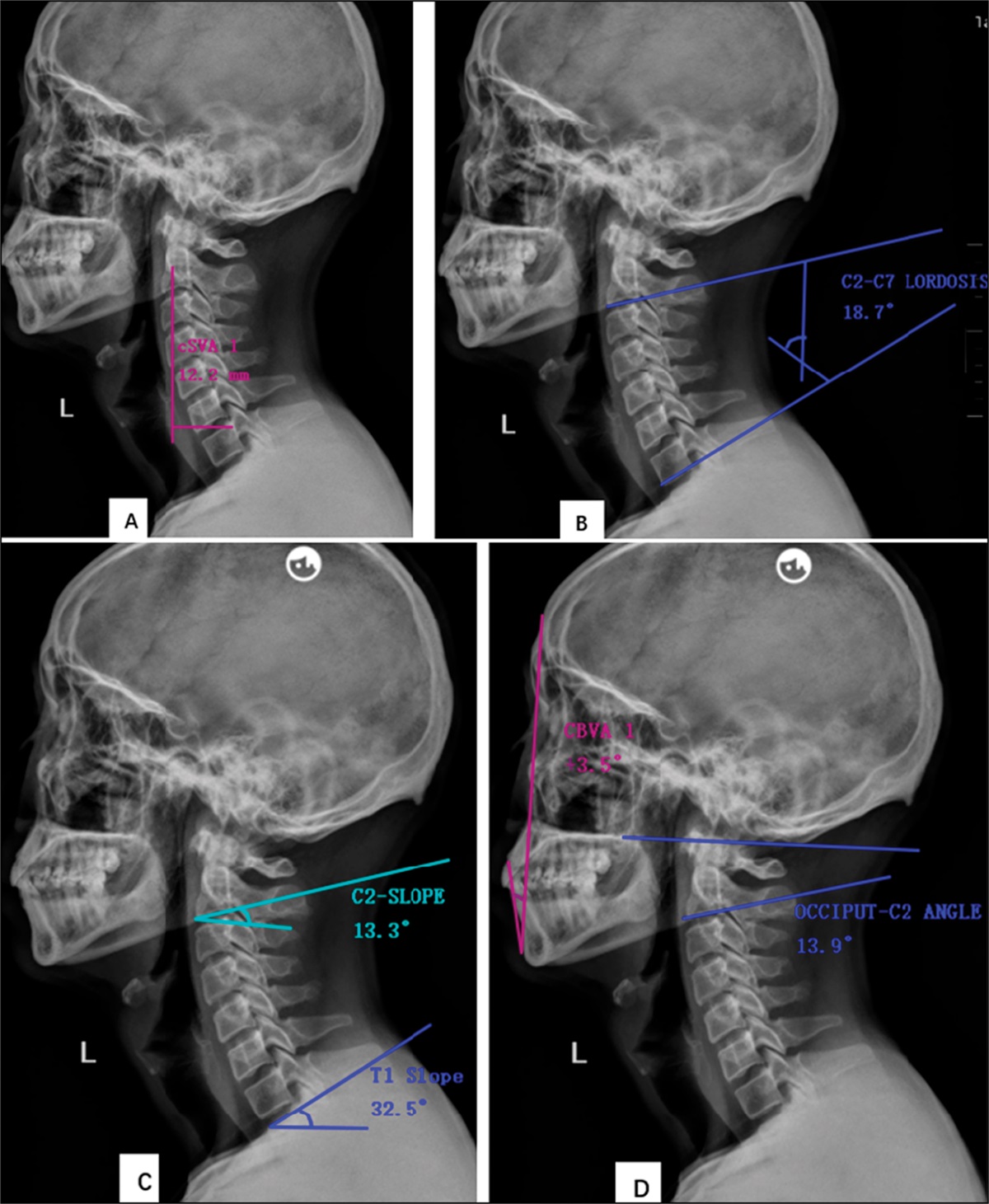
Both preoperative and postoperative CSA included C2 slope (C2S), which was measured as the angle between the lower end plate of C2 and the horizontal plane. T1 slope (T1S) was measured as the angle between the superior end plate of T1 and the horizontal plane. Cervical lordosis C2-C7 (CL) was measured as the angle between the inferior end plate of C2 vertebra and the inferior end plate of C7 vertebra. C2-C7 sagittal vertical axis (C2-C7 SVA) was measured as the distance between the C2 plumb line and the posterior upper end plate of C7 vertebral. Occiput-C2 lordosis angle (C0-C2 angle) was measured as the angle subtended between McGregor line and the inferior end plate of C2. Chin brow vertical angle (CBVA) was measured as the angle formed by a vertical line and a line connecting the most anterior aspect of the forehead and chin (Figure 1). The timing for measuring radiographs in the revision surgery group was right before the primary surgery, right after the primary surgery, and right before-revision surgery (Table 3, https://links.lww.com/JAAOS/B18). All measurements were done by using surgmap software.
 Figure1:
Figure1: Diagram showing the description of radiographic measurement. A= C2-C7 sagittal vertical axis was measured as the distance between the C2 plumb line and the posterior upper end plate of C7 vertebra. B= Cervical lordosis (C2-C7) was measured as the angle between the inferior end plate of C2 vertebra and the inferior end plate of C7 vertebra. C= C2-slope was measured as the angle between the lower end plate of C2 and the horizontal plane, and T1-slope was measured as the angle between the superior end plate of T1 and the horizontal plane. D= Chin brow vertical angle (CBVA) was measured as the angle formed by a vertical line and a line connecting the most anterior aspect of the forehead and chin. Occiput-C2 lordosis angle (C0-C2 angle) was measured as the angle subtended between the McGregor line and the inferior end plate of C2.
Statistical AnalysisIBM SPSS (version 22) was used for statistical analysis. Data normality was assessed using the one-sample Kolmogorov-Smirnov test. An independent sample t-test was used for continuous variables that follow the normal distribution and the Wilcoxon sum rank test for the variable that does not follow the normal distribution. The chi-square test was used for categorical variables. The binary logistic regression equation of containing the variables (number of comorbidities, smoking status, level of fusions, and BMD) was established. The Pearson correlation coefficient was used to evaluate the strength of association between T1S-CL and C2S. A P-value of < 0.05 was considered to be statistically significant.
Development of the prediction model: The prediction model was developed from a sample of 99 patients. We included six variables in the binary logistic regression model (number of comorbidities, smoking status, level of fusions, BMD, C7SVA, and T1CL-C2S). The outcome of surgery as a dependent variable was coded as no revision surgery = 0 and revision surgery = 1. To develop the best model fit and easy to use in healthcare practice, the number of predictors in the 6-predictor model was reduced to the 5-predictor model (BMD, smoking status, level of fusions, C2C7SVA, and T1CL-C2S) by the backward stepwise statistical method. The Nagelkerke R-square was used as a measure of overall predictive performance. The agreement between the predicted and observed revision surgery cases was assessed by the Hosmer-Lemeshow goodness-of-fit test; a P value ≥ 0.05 shows that the predicted outcome does not deviate from the observed outcome, meaning that the model is adequate. The ability of the model to discriminate between revision and nonrevision surgery patients was investigated by the receiver operating characteristic curve (ROC) analysis. The area under the ROC curve (AUC) reflects discrimination.
As potential CSA predictors of the results of revision surgery, T1CL-C2S and C7SVA caught our attention as well. Using binary logistic regression, we created a predictive model for T1CL-C2S and C2C7SVA alone and examined its capacity to distinguish between revision and nonrevision surgery. We calculated the TICL-C2S's sensitivity, specificity, accuracy, and optimal cutoff point from the ROC curve.
Results Demographic InformationNinety-nine of the patients met the inclusion criteria, and the mean age of the patients was 53.42 ± 9.30 years. Sixty-six percent of the patients were male, and 34% of the patients were female. Compared with the nonrevision surgery group (B), there were more smokers in the revision surgery group (A) (14/50 versus 30/49, P = 0.001), respectively. Patients in group A had more additional comorbidities than patients in group B (30/49 versus 20/50, P = 0.012). Other patients' preoperative demographic information can be seen in Table 1, https://links.lww.com/JAAOS/B16.
Radiographic Outcome of Cervical Sagittal AlignmentThe (T1-CL)-C2S mismatch was highly significant in group A compared with group B (9.95 ± 9.95)0, (3.79 ± 6.58)0, P < 0.05. Moreover, there was a strong association between C2S and T1CL in group B relative to group A postoperatively (R2 = 0.42 versus R2 = 0.09), respectively (Figure 2). Postoperative C2S was relatively lower in group A (8.30 ± 10.86)0 compared with group B (11.62 ± 7.11)0, P = 0.07. Compared with group B, patients in group A had significantly higher C2C7SVA values preoperatively (8.37 ± 5.07 mm versus 5.37 ± 2.68 mm, P = 0.002) and postoperatively (8.56 ± 6.40 mm versus 6.44 ± 3.00 mm, P = 0.04). The (C0-C2)-C2 mismatch was high in group A compared with group B ([11.97 ± 8.30] versus [7.48 ± 5.26], P = 0.008). In addition, group A had more levels of fusion compared with group B ([3.67 ± 1.04] versus [3.06 ± 0.68], P = 0.001). Other preoperative and postoperative CSA values can be seen in Tables 1, https://links.lww.com/JAAOS/B16, and 4, https://links.lww.com/JAAOS/B19.
 Figure 2:
Figure 2: A scatter plot depicting the association between C2 slope (C2S) and T1S-CL preoperatively and postoperatively in the revision and nonrevision groups.
Revision Surgery Prediction ModelWhen all six predictors were included in the binary logistic regression model (Nagelkerke R-square 0.48). Smoking was the best predictor of revision surgery followed by number of fusions, BMD, number of comorbidities, (T1S-CL)-C2S, and C2C7SVA. After backward statistical reduction, five predictors remained in the final model (smoking, number of fusions, BMD, [T1S-CL]-C2S, and C2C7SVA) (Nagelkerke R-square 0.476). The 5-predictor model was adequate with Hosmer and Lemeshow goodness of fit (χ2 = 6.67 df 8 P = 0.57). The model has a sensitivity of 73.5%, specificity of 84%, and accuracy of 78.8%. The log odds for revision surgery from our prediction model are given by the following equation:
Y= logit(p) = −10.51 +1.56*smoking +0.96*(number of fusions) +1.11*BMD +0.14*(C2C7SVA) +0.13((T1-CL)-C2S).
Discrimination between revision surgery and nonrevision surgery was good (AUC = 0.856; 95% CI 0.781 to 0.931) (Figure 3).
 Figure 3:
Figure 3: ROC curve of the 5-predictor model among revision and nonrevision surgery patients.
The equation Y= −1.92 +0.146*(C2C7SVA) +0.141*((T1-CL)-C2S) predicted the log odds for revision surgery when only (T1-CL)-C2S and C2C7SVA were included in the binary logistic regression. This equation's description was given as (AUC = 0.787; 95% CI 0.695 to 0.878), Figure 4. For (T1-CL)-C2S, the optimal cutoff was 9.100, and for C2C7SVA, it was 2.8 mm.
 Figure 4:
Figure 4: ROC curve for the cervical sagittal alignment predictor model ([T1S-CL]-C2S, C2C7SVA) among revision and nonrevision surgery patients postoperatively.
DiscussionPrevious scholars10 have shown that patients with spinal sagittal malalignment of the thoracolumbar or spinopelvic region experience poor health-related outcomes; however, the relationship between cervical sagittal balance and patients' functional outcomes has received less attention. In this study, we compared the postoperative cervical sagittal parameters of revision versus nonrevision surgery in symptomatic cervical myelopathic patients and analyzed the differences. We found a significant (T1S-CL)-C2S mismatch in the revision surgery group compared with the nonrevision surgery group postoperatively (Figure 5). Moreover, there were strong correlations between C2S and T1S-CL in the nonrevision surgery group compared with the revision surgery group. In a study done by Protopsaltis et al9 to define a simplified singular measure of cervical deformity, the authors found a strong correlation between C2S and T1S-CL. Moreover, the authors reported poor health-related quality of life (HLQOL), such as Neck Disability Index and mJOA numeric rating scale for neck pain (NRS), in cervical deformity patients with higher C2S. In a study done by Jeon S-I et al11 to investigate the relationship between CSA and patient-reported HRQOL after ACDF, the authors found that a greater TS-cervical lordosis (CL) mismatch corresponded to poor HRQOL outcomes and positive cervical sagittal malalignment. In addition, a study done by Hyun et al12 to investigate the long-term relationship between CSA and HRQOL after multilevel posterior fusion surgery, the authors found that a high T1S-CL mismatch was associated with a greater degree of cervical sagittal malalignment. C2S correlates with upper-cervical and subaxial alignment, while T1S-CL describes the harmony between cervical alignment and thoracolumbar alignment, or more specifically upper thoracic alignment. If the two components of T1S-CL are considered separately, the T1S is a reflection of the primary thoracolumbar alignment. C2S is a mathematical estimate of T1S-CL that is useful when T1S and C7 slopes are approximately equal. Furthermore, it is proposed that the C2S by functioning as a link between the occipitocervical and cervicothoracic spines can accurately describe cervical deformity.9,13 Patients with a notable mismatch of C2S and T1S-CL after ACDF or ACCF had a high rate of revision surgery in this study, most likely due to an imbalance of upper cervical and thoracolumbar alignment, which resulted in maximum energy expenditure during activities or during rest.14
 Figure 5:
Figure 5: Radiographs of a 45-year-old man (A, B, and C) who underwent anterior cervical corpectomy and fusion) secondary to cervical disk herniation at C4/C6. Immediate postoperative (B) T1S-CL versus C2 slope was 5.40; after 3 years, the same patient developed disk herniation at C3/C4 and underwent revision surgery. D and E depicts a 54-year-old woman who underwent ACCF at C4/C6 for a herniated cervical disk. The immediate postoperative (B) mismatch between T1S-CL and C2S was 0.70, and more than 3 years of follow-up revealed no recurrence.
We found a notable increase in C2C7SVA postoperatively in the revision surgery group compared with the nonrevision surgery group. Zoher et al15 in their study determined the effect of cervical sagittal balance on HRQOL outcome on symptomatic cervical myelopathic patients after surgery and also found that increased C2C7SVA was associated with poor HRQOL outcome scores. Smith et al16 in the study correlated preoperative CSA with symptomatic cervical myelopathic patients and also found that cervical sagittal balance C2C7SVA correlates with myelopathy severity. Some studies17,18 have shown that increased C2C7SVA after fusion results in increased load on the adjacent segment, which ultimately leads to the occurrences of adjacent segmental diseases. In this study, more than 51% cause of revision surgery was adjacent segmental diseases (ASD). The mean C2C7SVA in patients with ASD was 10.15 ± 5.5 mm. We believe that the cause is due to the complex kinematics of cervical equilibrium in a live individual. C2C7SVA is a measure of the severity of the forward head posture. In addition, increased C2-C7SVA correlates with higher T1S. Patients with higher T1S rely on the posterior paraspinal muscle to maintain horizontal gaze and conserve energy for head positioning. Having posterior muscular weakness increases the likelihood of postoperative problems such as cervical sagittal malalignment and kyphosis.19
In (C0-C2)-C2S, we identified a notable difference between the two groups. Patients who had revision surgery had a larger (C0-C2)-C2S mismatch than patients who did not have revision surgery. However, no notable differences in C0-C2 angle or C2S were found between the revision and nonrevision groups. Studies20,21 have suggested that the normal value of C0-C2 angle should be in the range of 00 to 300, in health individual, and more than 300 was reported to associate with complications such as dysphagia and cervical misalignment. In this study, all patients in revision and nonrevision groups have values of C0-C2 angle within the range of the health individual. In addition, we did not encounter dysphagia among the complications from both groups. Probably is because of our surgical technique through which we fix the patients' head in neutral posture during surgery and maintain that posture for 3 months postsurgery by having the patients wear a neck collar. Moreover, our fusion did not involves C0-C2.22
We also found a negative correlation of C0-C2 relative to CL in both groups postoperatively. Similar result has been reported by other authors as follows: A study was done by Korovessis et al23 to investigate HLQOL after instrumentation fusion after subaxial cervical trauma, and the authors found that C0-C2 had a negative correlation with CL in patients who underwent fusion surgery relative to the control health individual. A study by Nojiri et al24 in asymptomatic health individual established the standard values of upper and lower cervical regions, and the authors found notable negative correlations between C0-C2 and CL. In addition, Sherekar et al25 in the study to establish the standard values of upper and lower cervical spine in Indian population reported similar findings. The explanation is that as the C0-C2 angle decreases, the cranium's center of gravity shifts forward, requiring the lower spine's lordosis (CL) to drop to maintain the horizontal gaze.21 However, the (C0-C2)-C2S mismatch between the revision and nonrevision surgery groups is a discovery that is new to us, and we do not yet have a good explanation. However, we concur with other authors23,26 that alterations at C0-C2 and CL are a physiologic mechanism for maintaining horizontal gaze in response to thoracolumbar malalignment.
In CBVA, there was no statistically significant difference between the revision and nonrevision surgery groups. A study by Suk et al27 to assess the significance of CBVA in patient with ankylosing spondylitis (AS) after surgery, found that the patient with CBVA between (-10 and 10)0 has better horizontal gaze and HLQOL satisfaction. Zheng et al28 investigated the significance of CBVA in patients with AS after thoracolumbar kyphotic deformity correction, and the authors also found that postoperative patients with CBVA ≥300 were extremely dissatisfied and the quality of life was very low. In our study, the mean CBVA of all patients in all groups was in the normal range of −100 -+100, and none of our patients reported about horizontal gazing. Furthermore, our cases were non-AS patients.
Researchers have inadequately described the normative and pathological values of CBVA. CBVA has only recently emerged as a potential parameter in the context of cervical pathology in patients with AS.29 Therefore, the role of CBVA in global sagittal alignment after ACCF/ACDF procedures needs to be explored further.
In fusion levels, the revision surgery group had more fused segments than the nonrevision surgery group, and the difference was statistically significant. Similar results have been reported by Veeravagu et al30 in the study describing a revision rate, complications and readmission for patients after single-level and multilevel ACDF. The authors found that patients with multilevel ACDF are more likely to undergo revision surgery compared with patients with single-level ACDF. The reasons given by the research studies31 are as follows: Increasing levels of fusion diminish range of motion, increase intradiskal pressure, and lead to the development of ASD, which is a risk factor for revision surgery.
The revision surgery group had many number of smokers than the nonrevision surgery group, and the difference was statistically significant. The relationship between smoking and the outcome of cervical surgery has not been thoroughly examined, and the available evidence is contradictory. Some scholars32 claim that smoking is associated with increased blood loss during surgery, increased number of hospital stays, poor wound healing, high rate of revision surgery, and other perioperative complications. While a study by Tsung-Hsi et al33 to compare the clinical outcome between smokers and non-smokers after anterior cervical fusion surgery, the authors found no correlation between smoking and poor clinical outcomes. A recent meta-analysis34 analyzed the data from eight studies and found that smokers were more associated with revision surgery than nonsmokers (ES = 1.80, 95% CI 1.06 to 3.06, P = 0.0029).
The probable explanations why smoking has adverse outcomes after cervical spine surgery are as follows: The formation of prostacyclin, a strong vasodilator and inhibitor of platelet aggregation, has been demonstrated to be inhibited by tobacco smoke products. This effect can result in diminished angiogenesis and epithelialization as well as impaired blood flow and increased blood viscosity, all of which affect blood supply. Furthermore, nicotine was found to block revascularization in animal research, which may slow cellular metabolism and hasten tissue degeneration.35
In addition, smoking has been shown to affect bone physiology, which leads to poorer fusion rates and decreased bone mineral density, impaired bone metabolism, and hastened osteoporosis.36
The revision surgery group was also shown to have more comorbidities than the nonrevision surgery group in this study. Furthermore, the difference was statistically significant. In a study by Veeravagu et al30 on revision rate, complications, and incidence of patients after ACDF surgery, the authors found that an increased number of comorbidities such as hypertension (HTN), diabetes mellitus, osteoporosis, and lung diseases were more prevalent in multilevel fusion patients who were also associated with a high rate of revision surgery. A study by Campbell et al37 on the incidence of complications and hospital-acquired conditions after spine surgery, the authors found that an increasing number of comorbidities in a single patient considerably increase the probability of a perioperative adverse events, including revision surgery. Scholars38 have also discovered that comorbidity such as diabetes, osteoporosis, consuming alcohol, lung disorders, renal failure, and heart failure are substantial risk factors for medical complications after cervical spine surgery.
We created the prediction equation model with the purpose of assisting healthcare professionals in improving the odds of detecting patients at risk of revision before ACCF/ACDF surgery or immediately after surgery and then recommends the best treatment suggestion.
A 5-predictor model including smoking, BMD, levels of fusion, C2C7SVA, and T1CLC2S as predictors showed adequate calibration and good discrimination between revision and nonrevision surgery. The model's sensitivity, specificity, accuracy, and discrimination were, respectively, 73.5%, 84%, 78.8%, and 85.6%, showing strong predictive performance.
Khan et al39 recently conducted a study utilizing machine learning to identify predictors of worsening functional status in patients with cervical myelopathy after ACCF/ACDF surgery. The authors used only mJOA as a functional status marker and obtained an equation model with a 74.3% accuracy, 88.2% sensitivity, 72.4% specificity, and 83.3% discrimination. These results are comparable with ours with minimal variations. This is probably due to the fact that the authors excluded radiographic variables such as CSA parameters from their model. In addition, the authors used mJOA, which is assessed by the clinician and may not reflect the patient's own perception of their health status. In addition, the authors excluded comorbidities from the equation model.
Among the 5-predictors, smoking was the strongest predictor of revision surgery with the highest odds followed by BMD, levels of fusions, C2C7SVA, and (T1S-CL)-C2S mismatch. Other scholars40 have found that smoking, increased levels of fusion, and low BMD are among the comorbidities that are highly associated with poor outcome after spine surgery.
We were particularly fascinated in C2C7SVA and (T1S-CL)-C2S because they were the only CSA parameters that differed markedly between revision and nonrevision surgery groups. The C2C7SVA and (T1S-CL)-C2S single-equation model performed well, with a sensitivity of 69.4%, specificity of 80.0%, accuracy of 74.7%, and discrimination of 78.7%. The optimum cutoff for (T1S-CL)-C2S was 9.10, whereas the optimal cutoff for C2C7SVA was 2.8 mm. We discovered that even with a normal C2C7SVA, a (T1S-CL)-C2S mismatch can result in a poor clinical outcome after ACCF/ACDF procedures. Thus, surgeons must minimize (T1S-CL)-C2S mismatch during preoperative surgical planning to optimize postoperative patient outcomes.
Despite these successes, this study has limitations which shall be addressed. First, the sample size was small, but despite this, our findings are consistent with what other scholars have reported in the literature. Second, we did not have extra data to test the performance of the prediction model. Moreover, the data were collected from a single center. We call upon future studies with a large sample size from multiple centers to confirm our findings.
ConclusionThe causes of revision surgery in cervical myelopathic patients after ACCF/ACDF are multifactorial. (T1S-CL)-C2S mismatch and high C2C7SVA are the best cervical sagittal parameters that increase the odds of revision surgery, and the effect is more enhanced when comorbidities such as smoking, low BMD, and increased levels of fusion are taken into account.
References 1. Woods BI, Hilibrand AS: Cervical radiculopathy: Epidemiology, etiology, diagnosis, and treatment. J Spinal Disord Tech 2015;28:E251-E259. 2. Oglesby M, Fineberg SJ, Patel AA, Pelton MA, Singh K: Epidemiological trends in cervical spine surgery for degenerative diseases between 2002 and 2009. Spine 2013;38:1226-1232. 3. Cho SK, Riew KD: Adjacent segment disease following cervical spine surgery. J Am Acad Orthop Surg 2013;21:3-11. 4. Hilibrand AS, Robbins M: Adjacent segment degeneration and adjacent segment disease: The consequences of spinal fusion?. Spine J 2004;4:190s-194s. 5. Saifi C, Fein AW, Cazzulino A, et al.: Trends in resource utilization and rate of cervical disc arthroplasty and anterior cervical discectomy and fusion throughout the United States from 2006 to 2013. Spine J 2018;18:1022-1029. 6. Sherief T, White J, Bommireddy R, Klezl Z: Cervical spondylotic myelopathy: The outcome and potential complications of surgical treatment. Acta Chir Orthop Traumatol Cech 2013;80:328-334. 7. Ames CP, Smith JS, Scheer JK, et al.: Impact of spinopelvic alignment on decision making in deformity surgery in adults: A review. J Neurosurg Spine 2012;16:547-564. 8. Tang JA, Scheer JK, Smith JS, et al., ISSG: The impact of standing regional cervical sagittal alignment on outcomes in posterior cervical fusion surgery. Neurosurgery 2012;71:662-669. 9. Protopsaltis TS, Ramchandran S, Tishelman JC, et al.: International Spine Study Group. The importance of C2 slope, a singular marker of cervical deformity, correlates with patient-reported outcomes. Spine. 2020;45:184-192. 10. Le Huec JC, Saddiki R, Franke J, Rigal J, Aunoble S. Equilibrium of the human body and the gravity line: The basics. Eur Spine J. 2011;20 (suppl 5):558-563. 11. Jeon SI, Hyun SJ, Han S, et al.: Relationship between cervical sagittal alignment and patient outcomes after anterior cervical fusion surgery involving 3 or more levels. World Neurosurg 2018;113:e548-e554. 12. Hyun SJ, Kim KJ, Jahng TA, Kim HJ. Clinical impact of T1 slope minus cervical lordosis after multilevel posterior cervical fusion surgery: A minimum 2-year follow up data. Spine. 2017;42:1859-1864. 13. Passfall L, Williamson TK, Krol O, et al.: Do the newly proposed realignment targets for C2 and T1 slope bridge the gap between radiographic and clinical success in corrective surgery for adult cervical deformity?. J Neurosurg Spine 2022;37:368-375. 14. Tang JA, Scheer JK, Smith JS, et al., ISSG: The impact of standing regional cervical sagittal alignment on outcomes in posterior cervical fusion surgery. Neurosurgery 2015;76suppl 1:S14-S21. 15. Roguski M, Benzel EC, Curran JN, et al. Postoperative cervical sagittal imbalance negatively affects outcomes after surgery for cervical spondylotic myelopathy. Spine. 2014;39:2070-2077. 16. Smith JS, Lafage V, Ryan DJ, et al.: Association of myelopathy scores with cervical sagittal balance and normalized spinal cord volume: Analysis of 56 preoperative cases from the AOSpine North America myelopathy study. Spine 2013;38:S161-S170. 17. Patwardhan AG, Khayatzadeh S, Havey RM, et al.: Cervical sagittal balance: A biomechanical perspective can help clinical practice. Eur Spine J 2018;27suppl 1:25-38. 18. Patwardhan AG, Khayatzadeh S, Nguyen NL, et al.: Is cervical sagittal imbalance a risk factor for adjacent segment pathomechanics after multilevel fusion? Spine. 2016;41:E580-E588. 19. Weng C, Wang J, Tuchman A, et al. Influence of T1 slope on the cervical sagittal balance in degenerative cervical spine: An analysis using kinematic MRI. Spine. 2016;41:185-190. 20. Matsunaga S, Onishi T, Sakou T: Significance of occipitoaxial angle in subaxial lesion after occipitocervical fusion. Spine 2001;26:161-165. 21. Zhu C, Wang LN, Chen TY, et al.: Sequential sagittal alignment changes in the cervical spine after occipitocervical fusion. World J Clin Cases 2022;10:1172-1181. 22. Bagley CA, Witham TF, Pindrik JA, et al.: Assuring optimal physiologic craniocervical alignment and avoidance of swallowing-related complications after occipitocervical fusion by preoperative halo vest placement. J Spinal Disord Tech 2009;22:170-176. 23. Korovessis P, Mpountogianni E, Syrimpeis V, Andriopoulou M, Korovesis A: Quality of life in adult patients receiving cervical fusion for fresh subaxial cervical injury: The role of associated spinal cord injury. Biomed Res Int 2021;2021:9931535. 24. Nojiri K, Matsumoto M, Chiba K, et al.: Relationship between alignment of upper and lower cervical spine in asymptomatic individuals. J Neurosurg 2003;99:80-83. 25. Sherekar SK, Yadav YR, Basoor AS, Baghel A, Adam N: Clinical implications of alignment of upper and lower cervical spine. Neurol India 2006;54:264-267. 26. Scheer JK, Tang JA, Smith JS, et al.: International Spine Study Group: Cervical spine alignment, sagittal deformity, and clinical implications: A review. J Neurosurg Spine 2013;19:141-159. 27. Suk KS, Kim KT, Lee SH, Kim JM. Significance of chin-brow vertical angle in correction of kyphotic deformity of ankylosing spondylitis patients. Spine. 2003;28:2001-2005. 28. Song K, Su X, Zhang Y, et al.: Optimal chin-brow vertical angle for sagittal visual fields in ankylosing spondylitis kyphosis. Eur Spine J 2016;25:2596-2604. 29. Lafage R, Challier V, Liabaud B, et al.: Natural head posture in the setting of sagittal spinal deformity: Validation of chin-brow vertical angle, slope of line of sight, and McGregor's slope with health-related quality of life. Neurosurgery 2016;79:108-115. 30. Veeravagu A, Cole T, Jiang B, Ratliff JK: Revision rates and complication incidence in single- and multilevel anterior cervical discectomy and fusion procedures: An administrative database study. Spine J 2014;14:1125-1131. 31. Hua W, Zhi J, Ke W, et al.: Adjacent segment biomechanical changes after one- or two-level anterior cervical discectomy and fusion using either a zero-profile device or cage plus plate: A finite element analysis. Comput Biol Med 2020;120:103760. 32. Wen-Shen L, Sheng MLW, Yeo W, et al.: No difference in functional outcome but higher revision rate among smokers undergoing cervical artificial disc replacement: Analysis of a spine registry. Int J Spine Surg 2020;14:916-923. 33. Tu TH, Kuo CH, Huang WC, Fay LY, Cheng H, Wu JC: Effects of smoking on cervical disc arthroplasty. J Neurosurg Spine 2019;30:168-174. 34. Zheng LM, Zhang ZW, Wang W, Li Y, Wen F: Relationship between smoking and postoperative complications of cervical spine surgery: A systematic review and meta-analysis. Sci Rep 2022;12:9172. 35. Buccoliero C, Oranger A, Colaianni G, et al.: The effect of Irisin on bone cells in vivo and in vitro. Biochem Soc Trans 2021;49:477-484. 36. Pearson RG, Clement RG, Edwards KL, Scammell BE: Do smokers have greater risk of delayed and non-union after fracture, osteotomy and arthrodesis? A systematic review with meta-analysis. BMJ Open 2016;6:e010303. 37. Campbell PG, Yadla S, Nasser R, Malone J, Maltenfort MG, Ratliff JK: Patient comorbidity score predicting the incidence of perioperative complications: Assessing the impact of comorbidities on complications in spine surgery. J Neurosurg Spine 2012;16:37-43. 38. Lee MJ, Konodi MA, Cizik AM, et al.: Risk factors for medical complication after cervical spine surgery: A multivariate analysis of 582 patients. Spine 2013;38:223-228. 39. Khan O, Badhiwala JH, Akbar MA, Fehlings MG: Prediction of worse functional status after surgery for degenerative cervical myelopathy: A machine learning approach. Neurosurgery 2021;88:584-591. 40. Hilibrand AS, Fye MA, Emery SE, Palumbo MA, Bohlman HH: Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am 2001;83:668-673.
Comments (0)