
Remember me


Obsessive-Compulsive Disorder (OCD) follows a chronic course in the majority of patients.1,2 Moreover, it is a disabling disorder accompanied by widespread limitations in work, household activities, social relations and well-being.3 OCD also affects families of patients, as most relatives become involved in performing compulsions or in dysfunctional interactions with the patient related to the OCD.4
Cognitive behavior therapy (CBT) is a first-line, evidence-based treatment for OCD, with exposure to response prevention (ERP) being the main element in CBT treatment protocols.5–7 Treatment is most often provided in an individual format, with weekly sessions lasting 45 to 90 minutes each. However, about 40% to 55% of patients with OCD do not improve sufficiently with CBT.6,8,9 Possible causes of this nonresponse to CBT are a disturbed process of fear extinction, a lack of meaningful activities due to OCD, decreasing motivation during ERP, and dysfunctional interaction patterns with relatives related to OCD.
According to learning theory, exposure to a feared, conditioned stimulus (CS) can lead to the extinction of fear by patients perceiving that the CS is not accompanied by an aversive, unconditioned stimulus (US).10 However, a systematic review indicates that patients with OCD may have impairments in the fear extinction process, resulting in higher fear responses during extinction learning compared with healthy controls.11 This persistent fear can reinforce avoidance behavior and compulsions, thus acting to maintain OCD. To overcome these impairments, nonfear associations with CS may need to be strengthened and made available in more contexts for patients with OCD.12 It is hypothesized that this may be achieved through longer exposure sessions and consecutive sessions over a shorter period, with fewer interruptions from confrontations with the CS in daily life. One possible approach is a brief, intensive outpatient format of ERP, which involves substantially longer and more concentrated sessions than in a regular outpatient format. Examples are the Bergen 4-day treatment, which includes 25 hours of ERP in only 4 days,13,14 and a 5-day intensive treatment for children.15 Although research into such brief, intensive ERP is scarce, the available studies suggest it is a feasible and effective treatment approach.16,17 However, little is known about the effectiveness of brief intensive ERP for individuals who have not responded to regular ERP. A recent randomized controlled trial in anxiety disorders, excluding OCD, demonstrated that brief, intensive exposure was as effective as regular CBT in reducing symptoms and disabilities.18 Moreover, the concentrated approach resulted in a lower dropout rate and a faster treatment response compared with weekly exposure.18 A meta-analysis by Remmerswaal et al16 of studies involving brief, intensive exposure-related therapies in patients with anxiety disorders and OCD showed that brief, intensive exposure-based treatments did not differ significantly from regular treatments in terms of posttreatment outcomes. Brief intensive exposure-based treatment also led to quicker effects due to the shorter lead time.16 However, interpretation of the findings was challenging due to the limited studies available and their designs and quality.16 In an open trial of an intensive, family-based CBT in youths who did not respond or only partially responded to at least 2 medication trials, Storch et al19 found that 80% showed improvement after intensive CBT with a mean reduction of obsessive-compulsive symptoms of 54%.
Nonresponse to CBT may also be due to causes other than a disturbed process of fear extinction, such as a lack of meaningful daytime activities due to OCD. Although increasing activities with behavioral activation has been found to be effective in major depressive disorder,20 it has scarcely been studied in the context of OCD. A study published in 2017 found that improvements in functioning were related to a reduction in OCD symptom severity in patients with OCD treated with ERP and psychotropic medication.21 A 2018 study found that, after a 4-week intensive ERP treatment, the level of general functioning in patients with OCD was also associated with obsessive-compulsive symptom severity.22
Another reason for treatment nonresponse may be decreased motivation due to fatigue from exposure treatment.23,24 In addition, dysfunctional interaction patterns with family members with regard to OCD can be a reason for nonresponse, as patterns of accommodation (adapting, participating) and antagonism (opposing, criticizing) are related to poorer treatment outcomes.25
OBJECTIVESThis pilot study had 2 goals. Our first goal was to evaluate the effects and the feasibility of a multifaceted, brief, intensive ERP treatment that was specially developed for patients with OCD who had not achieved adequate improvement through the first step of CBT. The treatment, which addressed several possible factors that may contribute to maintaining OCD, consisted of lengthy sessions of ERP in quick succession (to enhance fear extinction), sustaining motivation, resumption of meaningful activities, and improvement of family interaction patterns. To reduce the burden on family members, the treatment also involved broadening the social network of the patient. The study evaluated several factors such as obsessive-compulsive and comorbid symptoms, functioning, quality of life, family interaction patterns, patient and family satisfaction, therapist satisfaction, feasibility of the organization of the treatment, and dropout rates. A secondary aim of this study was to get an impression of the impact of the treatment on the course of OCD through consecutive case series using trajectories of day-to-day improvement.
METHODS Participants and ProcedureAdult participants (≥18 y of age) with a principal DSM-5 diagnosis of OCD who had experienced no significant improvement after at least 1 recent CBT treatment for OCD, including weekly ERP, plus at least 1 pharmacological treatment (except for 3 patients who refused medication), and who had a score on the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS)26,27 of at least 16 (indicating at least moderately severe obsessive-compulsive symptoms), were recruited between 2017 and 2021 from a mental health outpatient clinic specializing in OCD. Participants were included if they had a family member who agreed to participate in the treatment. Concomitant use of psychotropic drugs was allowed. Patients were on stable doses of medication at pretreatment. Before enrolling in the intensive exposure program, participants’ motivation was evaluated to ensure their willingness to engage in the treatment. Motivation was assessed on the basis of completion of preparatory homework (see below) and preparedness to engage in anxiety-provoking exercises without major reservations. OCD was diagnosed using the Structured Clinical Interview for DSM-IV (SCID-I).28 This pilot study was approved by the Medical Ethics Committee of the VU-University Medical Centre. All participants and their family members gave written informed consent.
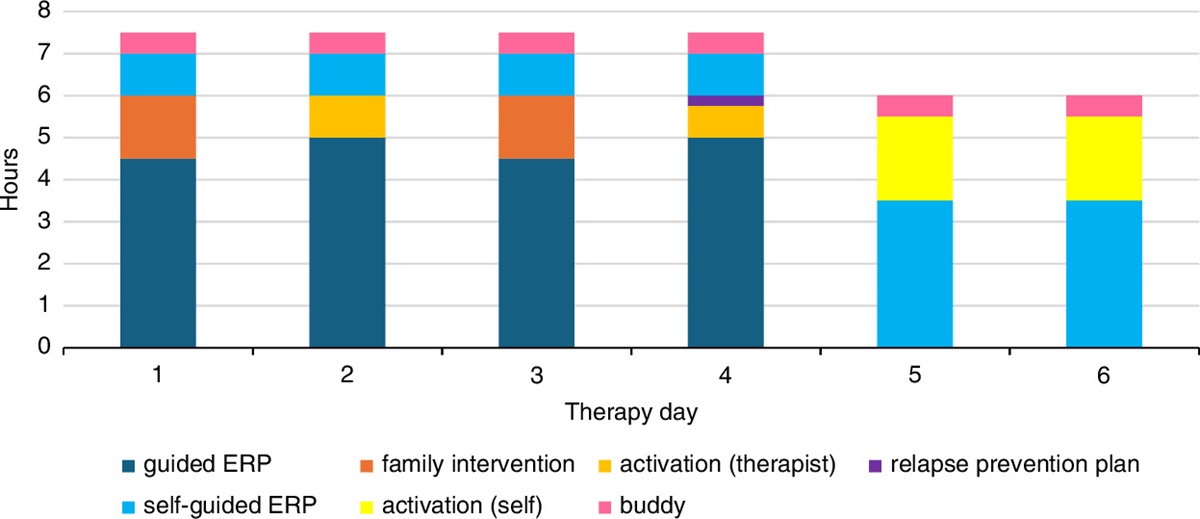
Multifaceted, Brief Intensive Exposure Treatment at HomeThe treatment consisted of 6 days with a total of 24 hours of therapist-guided therapy at the homes of the patients, consisting of 19 hours of ERP, 3 hours of family interventions, and 2 hours discussing activities. In addition, there were 12 hours of self-guided ERP, plus 3 follow-up sessions. For a schematic layout of the treatment, see Figure 1. The 6 treatment days were planned in 3 blocks of 2 consecutive days with breaks on the weekend and a day in between. Thus, the treatment had a 9-day lead time. The ERP-free days were scheduled so that the patient was able to recover from the intensive treatment days. The participants were instructed to engage in pleasurable activities while maintaining the results achieved.
 FIGURE 1:
FIGURE 1:
Schematic layout of treatment components.
The multifaceted, brief, intensive ERP had 4 main objectives. The first goal was to reduce the obsessive-compulsive symptoms of the patient through the use of ERP. The intensive ERP was delivered by 4 therapists who each provided treatment at the homes of the participants for a day (or at other places where the symptoms of OCD were most evident). The therapists shared their experiences with the therapist who was scheduled to work with the patient the following day. ERP included a total of 19 hours of therapist-assisted ERP and an additional 12 hours of self-controlled ERP. In addition, in the evenings after each treatment day, patients performed additional self-controlled ERP exercises besides the 12 hours mentioned above. The self-guided ERP exercises were designed to expand the number of situations in which the individuals developed a nonfear association, thereby preventing therapists from becoming “safety signals.” The content of the initial ERP exercises was based on the patient’s predominant compulsion and secondarily on other rituals practiced. ERP was delivered without hierarchy29 and conducted as behavior experiments. Thus, before ERP was started, the participant determined the feared consequence of the planned exercise. After ERP, the therapist and patient discussed whether the anticipated consequence had occurred and, if not, whether the obsession’s credibility had changed. Where the obsession could not be changed (eg, a “not just right” feeling after ERP that remained), the participant learned to resist responding to this obsession with compulsions. The second goal of the treatment was to normalize interactions related to OCD with the relatives closest to the patient, typically the partner or parents. There were 2 sessions of 90 minutes each with the patient and 1 or more family members to reduce accommodation and antagonism toward the patient’s obsessive-compulsive symptoms.30 In addition, patients purposefully contacted a buddy from their social network on a daily basis to discuss treatment and get support. This strategy can help increase understanding of OCD within the patient’s social circle, potentially reducing the burden and antagonizing behavior of family members. The buddy was instructed on how to support the patient, including psychoeducation on accommodation and antagonism, during a brief call with the therapist and the patient. The third goal of the treatment program was to help patients regain roles in daily life and society. Two sessions of 60 minutes each were spent discussing and planning (daily) activities and pleasurable activities, including those on the ERP-free days. The last goal was to prevent relapse. Patients created a personal relapse prevention plan, which was then reviewed and practiced in 3 follow-up sessions and through email correspondence.
After completing the 6 intensive ERP days at home, patients attended the first follow-up session of 45 minutes with the senior therapist who set up treatment. In this session, the therapist discussed the self-controlled ERP exercises with the patients and motivated them to continue practicing ERP exercises in the subsequent weeks. Their personal relapse prevention plan was also discussed. Furthermore, the patients were informed that they could contact the therapist in the case of relapse or crisis. After this, patients sent an email every 3 weeks with an update on their exposure exercises and symptoms. Two more follow-up sessions were scheduled with the patient and their family member at 1 and 3 months after the last session.
Before the start of the intensive treatment, several preparatory activities were conducted. Participants and a family member were invited for two 1-hour sessions with a senior therapist to determine the content of the intensive treatment. The participants received a patient manual which included instructions for making a case conceptualization and a list of exposure exercises. Patients also made an inventory of daily activities to resume after treatment. To remain motivated, the participants created a collage of their life without OCD and placed it in a central location in their home. In addition, participants asked someone from their social network to serve as a buddy to provide support and encouragement during the treatment period.
To ensure treatment integrity, a detailed day-to-day protocol was developed, and therapists underwent 2-hour training sessions. During the training, the treatment protocol was thoroughly discussed and therapists were trained in family interventions. This allowed for consistency in the application of the treatment across different therapists and ensured that patients received the same level of care and attention throughout their treatment.
AssessmentsComplete assessments were conducted pretreatment, posttreatment, and at 3-month follow-up; these included assessor-ratings by treatment-independent research nurses and self-ratings by patients and involved family members. Functioning and participation in society were assessed only at pretreatment and follow-up. In addition, daily self-report measures on the severity of OCD were completed by the patient during the 9-day lead time of the treatment and on the day before and the day after treatment. Finally, a questionnaire was completed by therapists at posttreatment. A detailed description of the instruments used is provided in online supplemental content, Supplemental Digital Content 1 (https://links.lww.com/JPP/A72).
Demographic and Clinical CharacteristicsData on the following demographic characteristics were gathered: age, gender, partner (yes, no), duration of relationship, children (yes, no), educational level, employment (yes, no), duration of OCD, presence of comorbid mental disorders, type and dosage of psychotropic medication, and number of previous treatments.
The severity of OCD was assessed using the original interview version of the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS).26,27 A self-report version of the Y-BOCS (Y-BOCS-SR) was constructed for daily measurements that ask about the severity of obsessive-compulsive symptoms in the previous day. The number and content of the items of the original Y-BOCS were preserved as much as possible; only the requested time period was adjusted. The Y-BOCS-SR was used solely to study how the severity of symptoms changed day to day throughout treatment, while the original Y-BOCS was used to assess treatment outcomes. Also, the Padua Inventory-Revised (PI-R)31 self-report severity scale was filled out by the patient. Insight into OCD was measured by the Overvalued Ideas Scale (OVIS), a self-report questionnaire.32
Comorbid anxiety and depressive symptoms were measured using the Beck Anxiety Inventory (BAI)33 and the Beck Depression Inventory (BDI).34
Several measures were used to evaluate patients’ functioning and quality of life. The World Health Organization Disability Assessment Schedule-II (WHODAS)35 was employed to evaluate daily functioning, while the EuroQol 5-dimensional questionnaire (EQ-5D)36 was used to assess quality of life. In addition, objective and subjective participation in society was measured using the Utrecht Scale for Evaluation of Rehabilitation–Participation (USER-P).37
Relationship Between Person With OCD and Partner/Family: Measurements in PatientsTo assess the perceived level of criticism by the family member, the Perceived Criticism Measure in the patient (PCM) was used.38 The Level of Expressed Emotion (LEE) was used to investigate the perceived level of expressed emotion from family members.39 Relationship satisfaction was measured using the Relationship Assessment Scale (RAS) only in those patients with a partner relationship.40 To assess the overall atmosphere at home, patients were asked to rate it on a visual analog scale ranging from 0 to 100, with higher scores meaning a more positive atmosphere.
Measurements in Partner/FamilyThe degree of accommodation to OCD by the partner/family members was measured using the Family Accommodation Scale–Interview version (FAS).41 Perceived level of criticism by the patient (PCM), relationship satisfaction (RAS), and atmosphere at home were also assessed. In addition, feelings of rejection toward the patient were measured using the Patient Rejection Scale (PRS).42 Daily functioning in the family member was measured using the WHODAS and quality of life with the EQ-5D.
Feasibility and Treatment SatisfactionDropout was defined as terminating treatment at any moment after completing the preparatory sessions. The level of satisfaction with the treatment among patients and their family members was assessed using a visual analog scale with values from 0 to 100, with higher values indicating more satisfaction. In addition, an interview consisting of 9 open-ended questions was conducted, which included questions such as “How did you experience the brief intensive ERP? What did you like/dislike about the program? How did you feel about dealing with multiple therapists?” The therapists’ satisfaction with the treatment was assessed using a questionnaire consisting of 7 open-ended questions, such as “How did you like working with this treatment? What did you think went well/not well?” The feasibility of the organization of the treatment was assessed by recording problems that arose in planning and organizing treatment (eg, problems in arranging therapists, unused scheduled treatment days).
Statistical AnalysisResults were analyzed using the Statistical Package for Social Sciences, version 28.43 Missing values at posttreatment (n=2), at follow-up (n=5), and at the daily Y-BOCS-SR measurements (between n=4 and n=9) were imputed with multiple imputation, 50 times. Pooled results were reported. The baseline characteristics of the sample were described through means, SDs, numbers, and percentages. Results from pretreatment, posttreatment, and follow-up were analyzed using related-samples Wilcoxon signed-rank tests. If a value of P<0.05 was found in a majority of the imputed data sets, we considered the effect to be significant. Effect sizes ‘r’ were calculated by dividing the standardized test statistic by the square root of the number of observations, with 0.3 considered a medium effect size and 0.5 considered a large effect size.44 Jacobson and Truax’s method45 was used to determine reliable change on the Y-BOCS (≥4.5 decrease in score) and clinically significant recovery (CSR; reliable change and post-test Y-BOCS ≤18.9) at posttreatment and follow-up, using data from Frost et al46 and Kim et al.47 Furthermore, to examine differences in Y-BOCS outcomes in patients with and without posttreatment CSR, post hoc analyses were performed. Daily measurements of OCD severity were analyzed using linear mixed models (LMM) to examine whether improvement in OCD severity coincided with treatment days by comparing relative improvements from the previous day. This analysis was performed on the original, not the imputed, dataset, as LMM accounts for missing values.
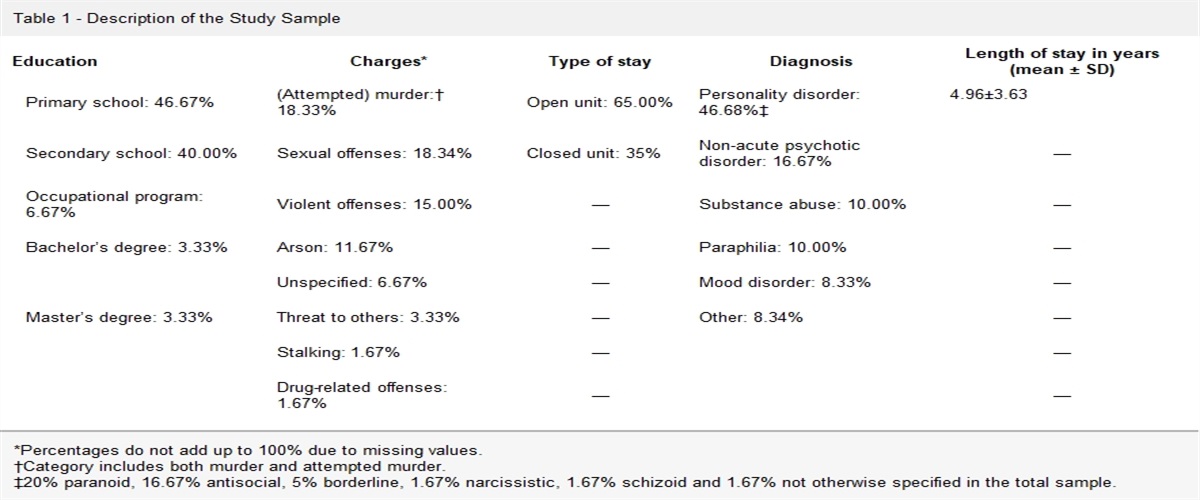
RESULTS ParticipantsTable 1 shows the baseline characteristics of our sample. A total of 22 participants (15 female; 68%) were included in this pilot study, with a mean age of 37.2 years (SD=13.6 y) and a mean duration of OCD of 17.5 years (SD=11.9 y). Patients were well educated: 10 (45%) had finished general secondary education or secondary vocational education and 12 (55%) had finished higher professional education or university.
TABLE 1 - Description of Sample at Baseline (N=22) Mean±SD or n (%) Sociodemographic characteristics Age (y) 37.2±13.6 Gender, female, n (%) 15 (68) Partner, yes, n (%) 15 (68) Duration partner relationship (y) 12.7±13.7 Child(ren), yes, n (%) 7 (32) Education, n (%) General secondary education/secondary vocational education 10 (45) Higher professional education/university 12 (55) Working (paid job), yes 12 (55) Clinical characteristics Duration of OCD (y) 17.5±11.9 Comorbid disorders, yes, n (%) 14 (64) Psychotropic medication, yes, n (%) 17 (77) Number of previous treatments Psychotherapy 3.2±2.4 Psychotropic medication 2.1±2.3One participant (5%) reduced the dose of antidepressants during the intensive treatment phase of the study due to adverse effects. During the follow-up period, 16 patients (73%) continued to follow the protocol of the brief intensive home-based ERP and had no medication changes, while 6 patients (27%) required additional treatment or a medication change: 3 patients received psychotherapy and psychotropic medication because of depressive symptoms, 1 participant received group sessions for OCD, 1 patient increased the dose of medication, and 1 patient stopped medication.
The baseline assessments (Table 2) suggest that the sample under study had severe obsessive-compulsive symptoms (Y-BOCS mean score of 28.7, SD=5.1) with fair insight (OVIS mean score of 4.9, SD=1.2). All measured OCD subtypes were present. In addition, participants scored moderately high on comorbid anxiety and depressive symptoms. The participants in our sample had a relatively poor quality of life, and they had a higher level of disabilities than 90% of the general population. Participants experienced many restrictions in participation in society and were not satisfied with their level of participation, although the frequency of their activities was found to be comparable to that of a reference group of rehabilitation outpatients who were physically or cognitively independent. Although the patients in the current study reported a moderate general level of expressed emotion in the relationship with the family member closest to them, they perceived the family members as critical. The atmosphere at home was adequate. Those with a partner (n=15) were satisfied with their relationship.
TABLE 2 - Treatment Outcome of Intensive ERP at Home in a Pilot Sample of 22 Participants with OCD Nonresponsive to Previous CBT Mean±SD P-range Wilcoxon S-R Tests*Follow-up after 3 months.
†Y-BOCS: higher scores indicate greater severity of symptoms.
‡P<0.05 in >25 imputed data sets.
§PI-R: clinical cut-off ≥53.
∥Subscales of the PI-R.
¶OVIS: ≥6 indicates poor insight.
#BAI: higher scores indicate more severe anxiety.
**BDI: higher scores indicate more severe depression.
††WHODAS: higher scores indicate more disabilities.
‡‡EQ-5D: assesses health status/quality of life; 1 indicates best possible health status.
§§User-P—Frequencies: higher scores indicate greater levels of participation in life activities.
∥∥User-P—Restrictions: higher scores indicate lower levels of limitations in daily life.
¶¶User-P—Satisfaction: higher scores indicate greater satisfaction with activities and life.
##PCM: higher scores indicate greater levels of criticism.
***LEE: higher scores indicate higher levels of expressed emotion.
†††RAS: higher scores indicate more satisfaction in the relationship.
‡‡‡Higher scores indicate a more positive atmosphere.
§§§Higher scores indicate greater satisfaction.
BAI indicates Beck Anxiety Inventory; BDI, Beck Depression Inventory; EQ-5D, EuroQol 5-Dimensional Questionnaire; LEE, Level of Expressed Emotion; NA, not applicable; OVIS, Overvalued Ideas Scale; PCM, Perceived Criticism Measure; PI-R, Padua Inventory-Revised; RAS, Relationship Assessment Scale, n=15; User-P, Utrecht Scale for Evaluation of Rehabilitation–Participation; WHODAS, World Health Organization Disability Assessment Schedule 2.0; Y-BOCS, Yale-Brown Obsessive-Compulsive Scale.
Family members (Table 3) accommodated the obsessive-compulsive symptoms to a moderate degree. Significant antagonism toward and rejection of the patient were present, as assessed by the Perceived Criticism Measure and the Patient Rejection Scale. Despite this, partners were satisfied with the relationship with the patient and experienced the atmosphere at home as rather good. The functioning and quality of life of family members were at the level of the general population.
TABLE 3 - Treatment Outcome of Intensive ERP at Home in a Pilot Sample of 22 Family Members of Participants with OCD Nonresponsive to Previous CBT Mean±SD P-range Wilcoxon S-R tests
Comments (0)