Blunt cardiac traumas account for < 10% of all trauma admissions [3]. Such trauma is commonly caused by motor vehicle accidents, pedestrian incidents, and falls from heights [3]. Among blunt cardiac trauma cases, aortic valve injuries are the most common, followed by mitral, tricuspid, and pulmonary valve injuries [3]. Posttraumatic AR following blunt chest trauma is thought to result from a sudden pressure increase during the early diastolic phase, when the transaortic pressure gradient peaks [4]. Among the three aortic valve cusps, the noncoronary cusp is the most vulnerable because it lacks a coronary artery opening and acts as a buffer for increased intra-aortic pressure [4]. Posttraumatic AR can occur not only because of direct valve injury but also through the progression of ascending aortic wall dissection, extending to the commissural and valve attachment areas [5].
In this case, acute AR was caused by the rupture of fenestrated fibrous strands, suggesting direct aortic valve cusp injury as the primary cause. Aortic valve fenestrations are defined as the loss of tissue in aortic valve leaflets, which occurs in all age groups, and their size increases with aging [6]. They are mainly located at the free edge of the leaflet at the commissural area, which is embryologically the weakest point of leaflet tissue [6]. Lifelong hemodynamical forces, mechanical stress caused by the dilation of the aortic root, sudden trauma, and iatrogenic injury causes fenestration formation [6]. Enlarged fenestration and fibrous strand rupture can lead to massive regurgitation and result in acute left heart failure [7].
Aortic valve cusp commissural fenestrations are well-described features of Marfan syndrome because of tissue fragility. Although large fenestrations as a cause of significant AR are rarely observed because patients with Marfan syndrome tend to receive early surgery nowadays [8], AR due to spontaneous rupture of a fenestrated fibrous strand in Marfan syndrome has been reported [9]. Pathological examination in this case revealed myxomatous degeneration of the valve leaflets, which has been reported as an important pathogenetic characteristic of fenestration-related massive AR [10].
A previous study analyzing 95 cases of posttraumatic AR reported that 69% of the cases were diagnosed within 3 months of onset, and approximately 5% were diagnosed > 5 years after trauma; thus, the time span from trauma to the onset of symptoms and diagnosis varies widely [11]. Although a fibrous strand at the commissural area might have been ruptured at the time of trauma in this case, the involved aortic cusp with a ruptured site retained some compensatory coaptation zone in the diastole phase [7], and AR was not severe at the time of trauma. The hemodynamic stress increased over the involved aortic cusp with worsening AR. Cusp remodeling progressed and finally led to a remarkable cusp prolapse [12]. Generally, posttraumatic AR is primarily treated with aortic valve replacement, expecting quick and definitive treatment effects, considering the urgency of surgery based on deteriorated cardiac function [4]. Valve repair may be an option if degeneration is limited to a single cusp and the overall health condition is accepted, although caution is warranted because microscopic trauma-induced degeneration in an apparently normal valve leaflet can lead to the postoperative recurrence of AR [11].
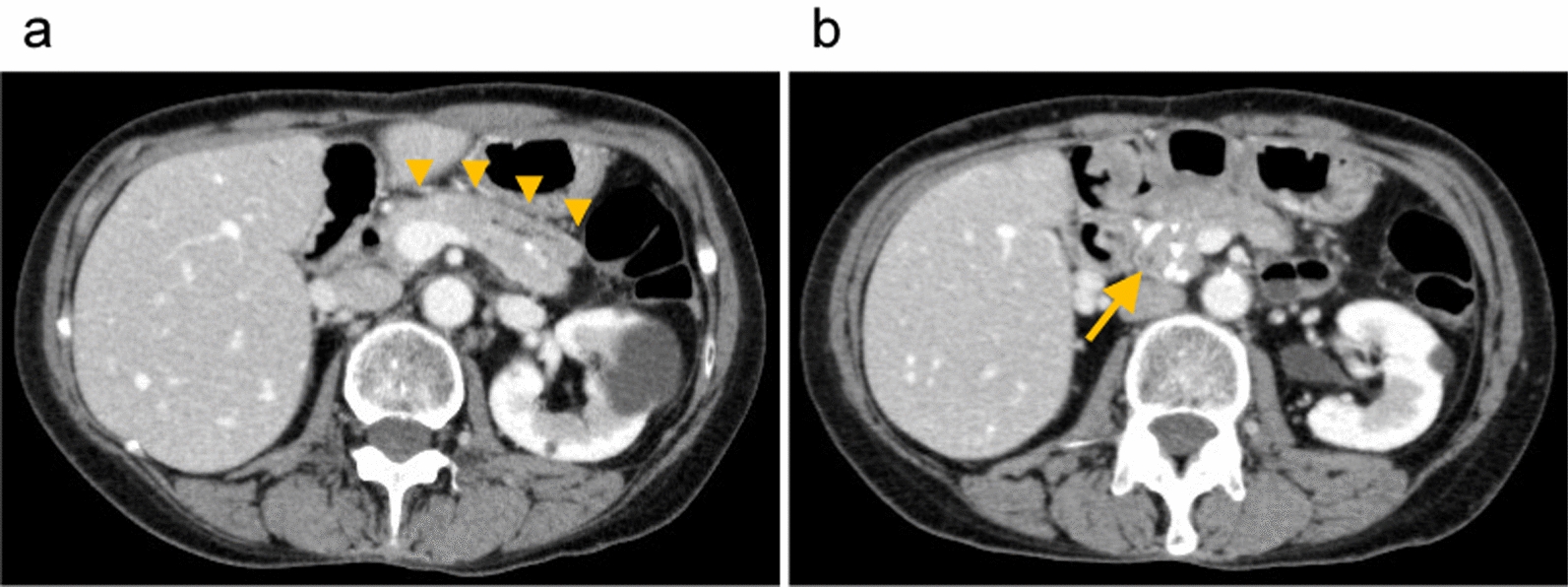
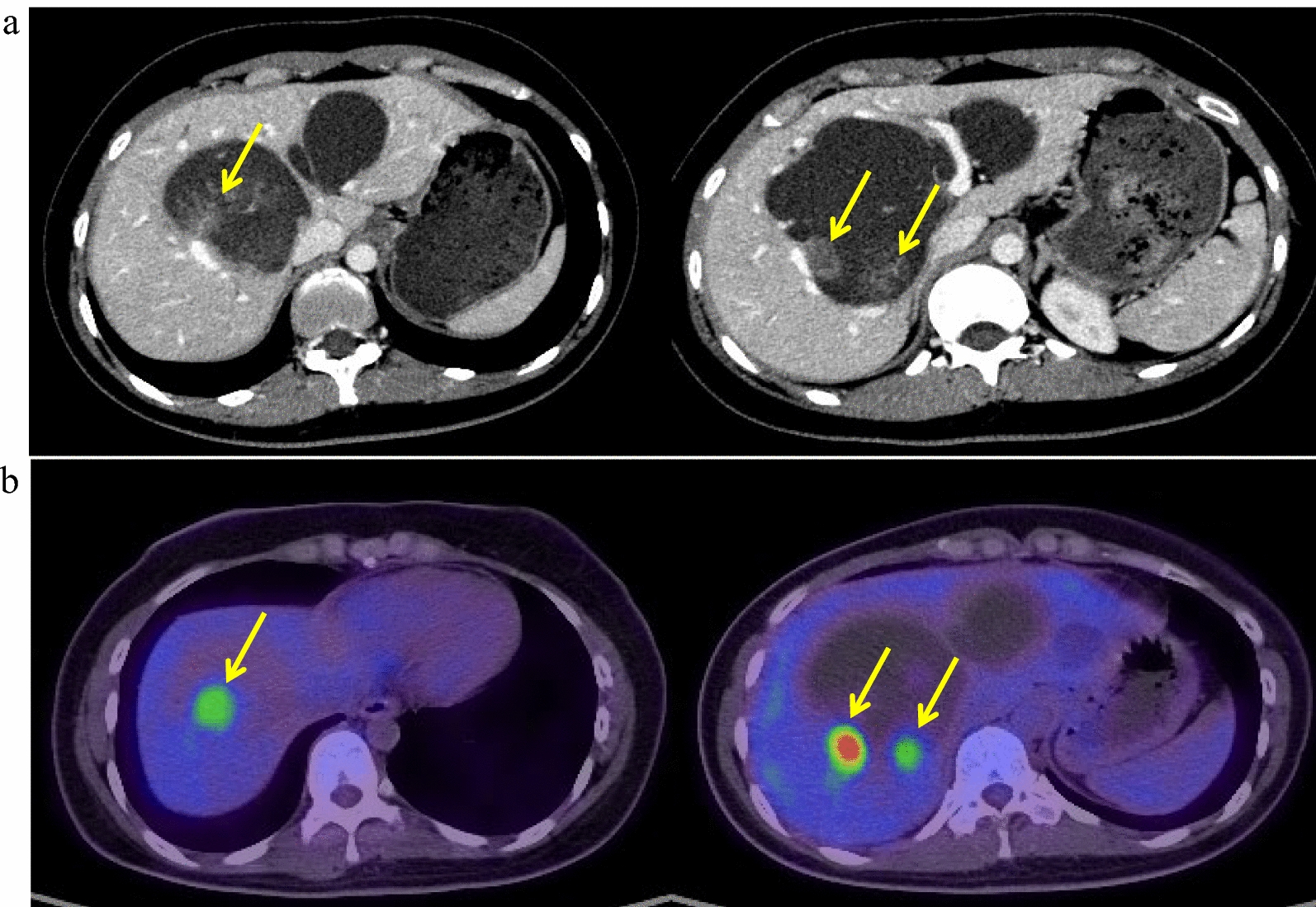
Blunt aortic injuries tend to be a fatal condition, with 80% of patients dying before presentation and diagnosis, and they most commonly occur in the aortic isthmus and ascending aorta [2, 13]. These injuries result from mechanical factors, such as shear, torsion, pinch, stretch, and hydrostatic forces, acting on the aortic wall [2, 14]. Blunt aortic injuries can cause pseudoaneurysms depending on the injured aortic tissue conditions and past aortic surgeries [2, 14]. Pseudoaneurysms are anatomically classified into four grades based on the aortic wall layers: intimal tear (Grade I), intramural hematoma (Grade II), pseudoaneurysm (Grade III), and rupture (Grade IV) [15]. Grade I and II cases may be managed nonoperatively through blood pressure control and imaging surveillance [16]. In Grade III cases, urgent or emergency surgeries may be required, depending on the patient’s condition and associated injuries. Grade IV cases require emergency surgeries, considering both surgical and endovascular interventions [2, 16]. The pseudoaneurysm of the aortic root in this case corresponded to Grade III. Pathologically, the pseudoaneurysm site exhibited evidence of the loss of tunica media elastic fibers in the aortic wall, which is consistent with the pathological features of Marfan syndrome. Aortic root replacement or repair is highly recommended for the emergent surgery for type A dissection in patients with Marfan syndrome because supracoronary ascending replacement is associated with a high need for root reintervention because of aortic insufficiency and root aneurysm [17]. However, in our case, we did not select aortic root replacement during the initial surgery because Marfan syndrome was recognized after the first surgery by genetic testing. Moreover, the false lumen of the aortic root was sealed with BioGlue® during the first surgery. Because BioGlue®-induced tissue toxicity has been reported [18], it could also have contributed to the formation of pseudoaneurysms in the aortic root in addition to the traumatic impact. Previously, pseudoaneurysms of the ascending aorta caused by fractured sternal wires have been reported [19]. In our case, although no evidence of sternal wire fracture was observed, the wire was positioned adjacent to the pseudoaneurysm orifice. Thus, the sternal wires may have contributed to adventitial injuries and intimal tears of the aortic root during trauma.
The simultaneous occurrence of severe AR and aortic root pseudoaneurysm following blunt trauma is extremely rare [20]. To the best of our knowledge, a case of the simultaneous occurrence of severe AR and aortic root pseudoaneurysm in a patient with Marfan syndrome has never been reported.









Comments (0)