
Remember me


The patient was a 27-year-old woman at 30 + weeks of gestation complicated with heart disease who underwent a caesarean section under spinal anaesthesia. The operation was successful, and a live baby boy weighing 3.5 kg was born. Postoperative intensive care unit care was given to the patient to adjust heart function and regular follow-ups were conducted after discharge. She was readmitted to hospital half a month after undergoing the caesarean section for further treatment. The patient had no history of allergic reactions to any medication or food and no history of a blood transfusion. Physical examination: The patient weighed 51.8 kg and was 162.5 cm tall, with an American Society of Anesthesiologists classification of III. Her body temperature was 36.6 °C, heart rate 117 times/min, respiration 19 times/min, and blood pressure 120/76 mmHg (1 mmHg = 0.133 kPa). Laboratory examination: white blood cells, 20.14 × 109/L, red blood cells 5.15 × 1012/L, and haemoglobin (Hb) 173 g/L; coagulation, liver, and kidney function, as well as electrolyte levels were generally normal. Five months previous, the patient had sought treatment for ‘coughing for 15 days and having chest discomfort for 6 hours’. Check echocardiography tips: The left atrium was significantly enlarged (left and right diameters 98 mm, upper and lower diameters 90 mm, left atrium area approximately 70 cm²), the left ventricle was enlarged, the right atrioventricular diameter was within normal range. Mitral valve: the anteroposterior diameter of the mitral annulus is 40 mm and the left and right diameters are 34 mm. The mitral lobe thickens, contracts, calcifies and increases echo, especially the obvious valve tip, junctional adhesion, the open diameter is about 7 mm, and the subvalvular tendon cord is thickened. Based on the limited nature of the valve opening, this area was estimated to be approximately 1.6 cm² using the cartography method, and the closure was seriously incomplete, as seen in Fig. 1. Tricuspid valve: no abnormality in morphology and structure, good opening, poor closure. Tricuspid valve: no abnormality in morphology and structure, good opening poor closure. Aortic valve: thickened lobe, good opening, open diameter 8 mm, poor closure, ring diameter 18 mm, sinus diameter 24 mm, sinus junction diameter 19 mm, ascending aorta diameter 28 mm. Pulmonary valve: structure, opening and closing are generally normal. In the systolic period, the forward flow velocity of the aortic valve increased, where Vmax = 1.9 m/s, PGmax = 15mmHg; a low-medium regurgitation signal was detected in the diastolic period, and the contractile part was 3.5 mm. In the diastolic period, the forward mitral flow velocity increased, the estimated valvular orifice area MVA (P1/2t) = 1.2 cm², and the systolic probing and probing and a large number of regurgitation signals, with a regurgitation area of 24.4 cm². Systolic detection and a low tricuspid regurgitation signal, regurgitation area of 4.0 cm².
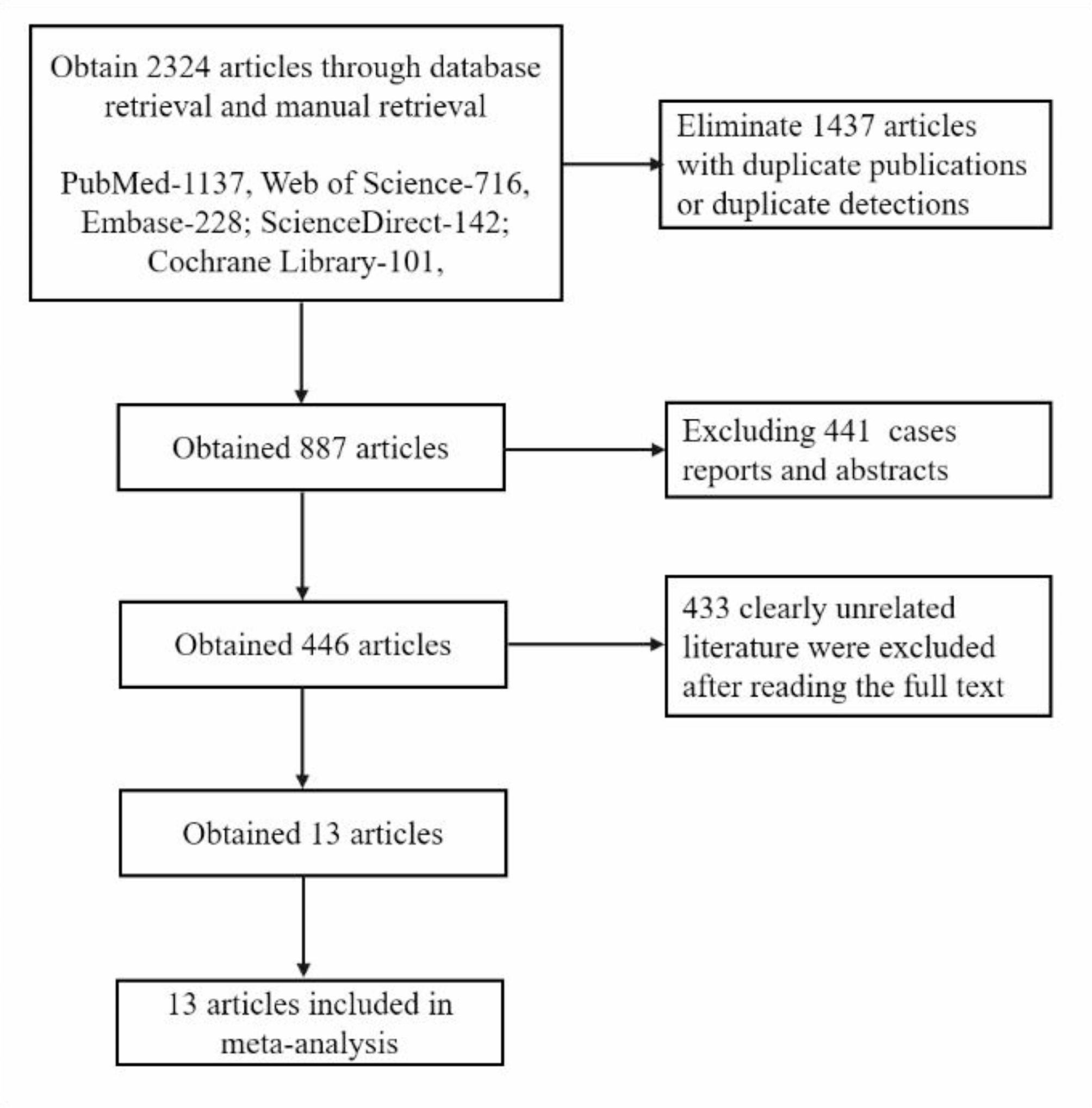
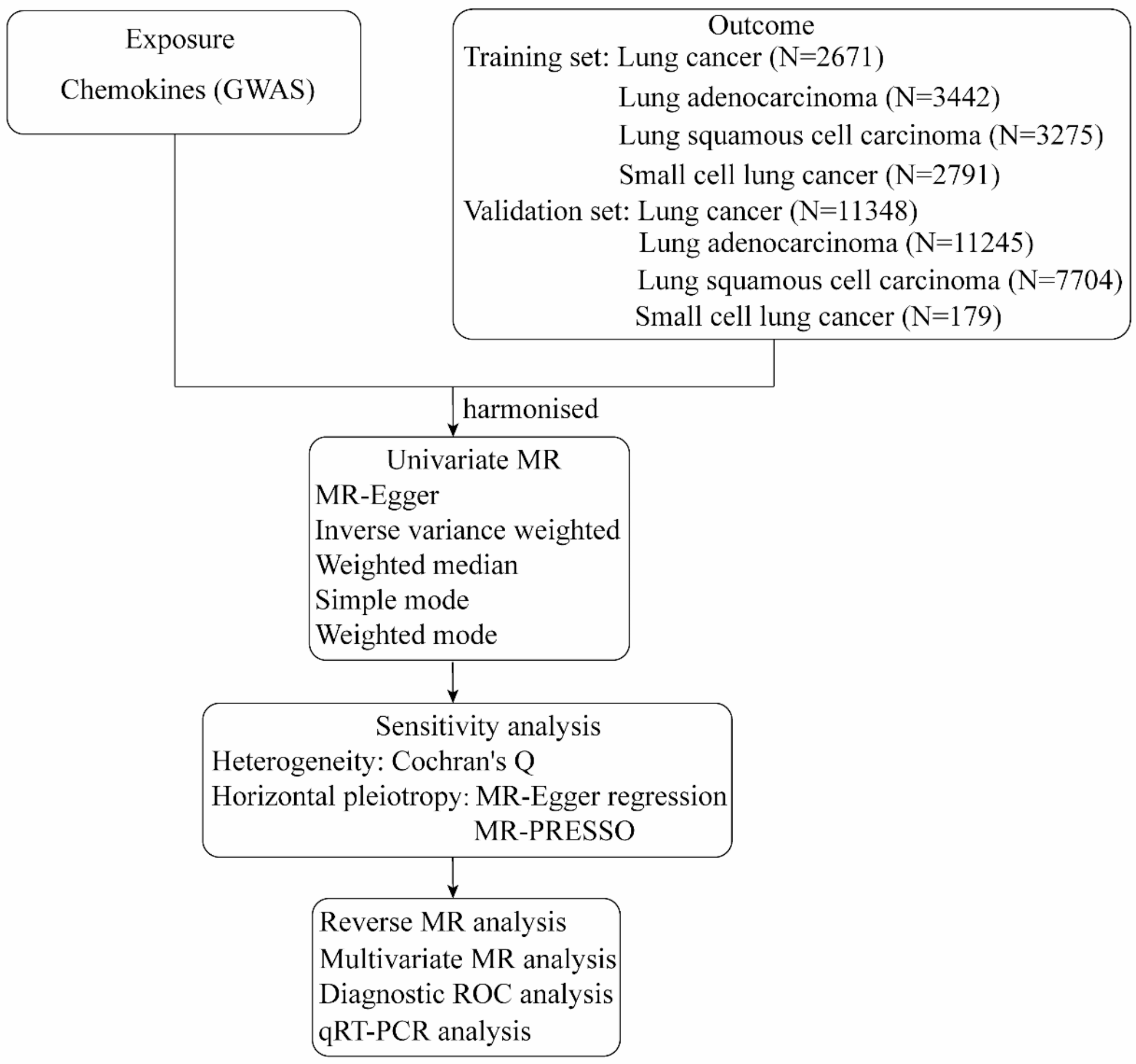
Fig. 1
Preoperative ultrasound diagnosis (mitral insufficiency). The anteroposterior diameter of the mitral ring was 40 mm, the left and right diameters were 34 mm, the lobe was thickened, contracture, calcification, and enhanced echo, especially with obvious valve tip, junction adhesion, open diameter about 7 mm, and thickened subvalvular tendinous cords. Due to the limited opening, the area of the valve opening was estimated to be about 1.6 cm² by the cartography method, and the closure was seriously unclosed
The patient was diagnosed with ‘rheumatic heart valve disease: moderate mitral stenosis with severe insufficiency, moderate aortic valve insufficiency, severe tricuspid insufficiency, severe pulmonary artery hypertension, class-II cardiac function, and atrial fibrillation’. The patient was scheduled to undergo ‘mitral valve replacement, aortic valve replacement, and tricuspid valve-shaping surgery’. Preoperative routine abstinence from drinking and eating was instigated, and communicate fully with patients before anesthesia to inform them of the nature of the surgery and the risks of surgery. Anaesthesia was induced using remimazolam at 6 mg/kg/h, remifentanil at 0.25 µg/kg/min, and rocuronium at 0.85 mg/kg. Remimazolam was adjusted by 1 mg/kg/h after loss of consciousness. A 7-cm midline chest skin incision was made. A sternal saw was used to perform a partial sternotomy from the right second intercostal space down to the xyphoid process. A 7-mm soft-flow aortic cannula was placed on the ascending aorta. Bicaval venous cannulation was performed using 22 Fr cannulas. The patient was placed on cardiopulmonary bypass with vacuum-assisted venous return. An aortic cross-clamp was placed, and cardiac arrest was achieved by cold-blood antegrade cardioplegia. Over 3 h into the surgery and 12 min after effecting cardiopulmonary bypass, an initial ‘test dose’ of 10 mg protamine was administered. The patient had no adverse reactions, and an injection of 400 mg protamine was used to neutralise heparin, and 1 g of human FIB (Jiangxi Boya Biopharmaceutical Group Co., Ltd., Lot No.: RX20211054) was dissolved in 50 mL of normal saline over 15 min by intravenous infusion. Roughly 2 min post-infusion, the patient experienced severe anaphylactic shock, with profuse generalised sweating, pale face, a barely noticeable skin rash, faint pulse, systolic pressure < 50 mmHg, and a heart rate of 71 beats/min. The FIB infusion, intravenous anesthesia and and the inhalation of anaesthetics were immediately stopped, as well as rapid infusions of crystalloid solution (compound electrolyte solution, 700 mL) and colloid (Polygeline, 200 mL) were administered, in addition to increasing the infusion rate of dopamine (from 0.5 to 1 µg/kg/min) and decreasing the infusion rate of milrinone (from 1.56 to 0.9 mg/h) during resuscitation. However, haemodynamics did not significantly improve. The cardiovascular collapse was initially considered to have had a surgical cause; however, no complex intracardiac complications were found upon examination by the surgeon at the surgical table or through postoperative transoesophageal echocardiography. Examination of the patient revealed skin flushing and swelling in the head and facial area; the anaesthesia machine showed an increase in peak airway pressure from 13 to 21 cm HO2, and urgent venous blood gas analysis indicated pH 7.3, pCO2 42 mmHg, PaO2 47 mmHg, haematocrit 45%, Hb 16.2 g/dl, and base excess − 5.7 mmol/L. A diagnosis of anaphylactic shock was immediately made, with adjustments to increase oxygen concentration and oxygen flow. Concurrently, 40 mg of methylprednisolone was administered intravenously, as well as 1 mg of adrenaline (Shanghai Hefeng Pharmaceutical Co., Ltd., Lot No.: 10,210,406), diluted with normal saline to 10 ml, at a concentration of 0.1 mg/ml by intravenous injection. The infusion speed was accelerated, and an additional 500 mL of Polygeline was administered. Approximately 20 min later, circulation was comparatively stabilised. During surgery, the patient was administered a total of 2,440 mL of fluids, with a blood loss of 600 mL and urine output of 1,780 mL. Post-surgery, the patient was transferred to the intensive care unit. The tracheal cannula was removed on the first day after the operation and the patient was discharged successfully on day 8. One month later, during a follow-up visit, her condition was found to be generally good. Apart from protamine, no other drugs that could cause allergies had been used before the allergic reaction. A residual heparin effect was found by conducting viscoelastic tests, and no allergic reaction occurred after using 100 mg protamine again, approximately 40 min post-correction of the anaphylactic shock. Therefore, we attribute the allergic reaction to FIB. To diagnose the allergic reaction to FIB more accurately, FIB immunoglobulin E (IgE) antibody was tested one week after the incident, and the result was positive. This case report was approved by the Ethics Committee of our hospital and the patient signed an informed consent form.
Comments (0)