
Remember me




The CLIMER (Clinical Dementia Rating Medical Record) study is an observational cross-sectional study. The study focused on data collected during memory consultations and as part of the MEMORA cohort [10]. The study has been carried out between 2019 and 2022 at the Memory Consultation of the Clinical and Research Memory Center of Lyon, at the Charpennes Hospital (Hospices Civils de Lyon), France. The study has been performed using the medical record of patients attending the memory center; the information were collected during routine care and from the MEMORA cohort.
Population study and sample sizeThe population study included consecutive patients attending a memory center, accompanied by their caregiver, whatever the neurocognitive etiology.
The patient’s medical records were selected consecutively over the study period, and according to the following criteria: patient of the memory center having a face-to-face interview allowing the assessment of the CDR-SB; patient with subjective cognitive decline (SCD) [11] or a neurocognitive disorders (mild cognitive impairment (MCI) or dementia) [12, 13] with an MMSE ≥ 12/30; and patients included in the MEMORA cohort. Patients or caregivers who did not want their data to be used for research purposes as part of the MEMORA cohort were not included. This research was an observational-type study (without intervention and new assessment requiring a new visit of the patient and his/her caregiver) which is part of the pathway of patients attending a memory center.
The number of subjects needed was 144 patients, estimated on the basis of an expected Cohen’s Kappa of 0.8, a standard deviation of 0.05, a proportion of patients with dementia expected at 40% during the face-to-face assessment and a similar proportion of dementia (40%) expected during the evaluation on the patient’s medical record, and an absolute precision of 0.1 (sskdlg function using Stata).
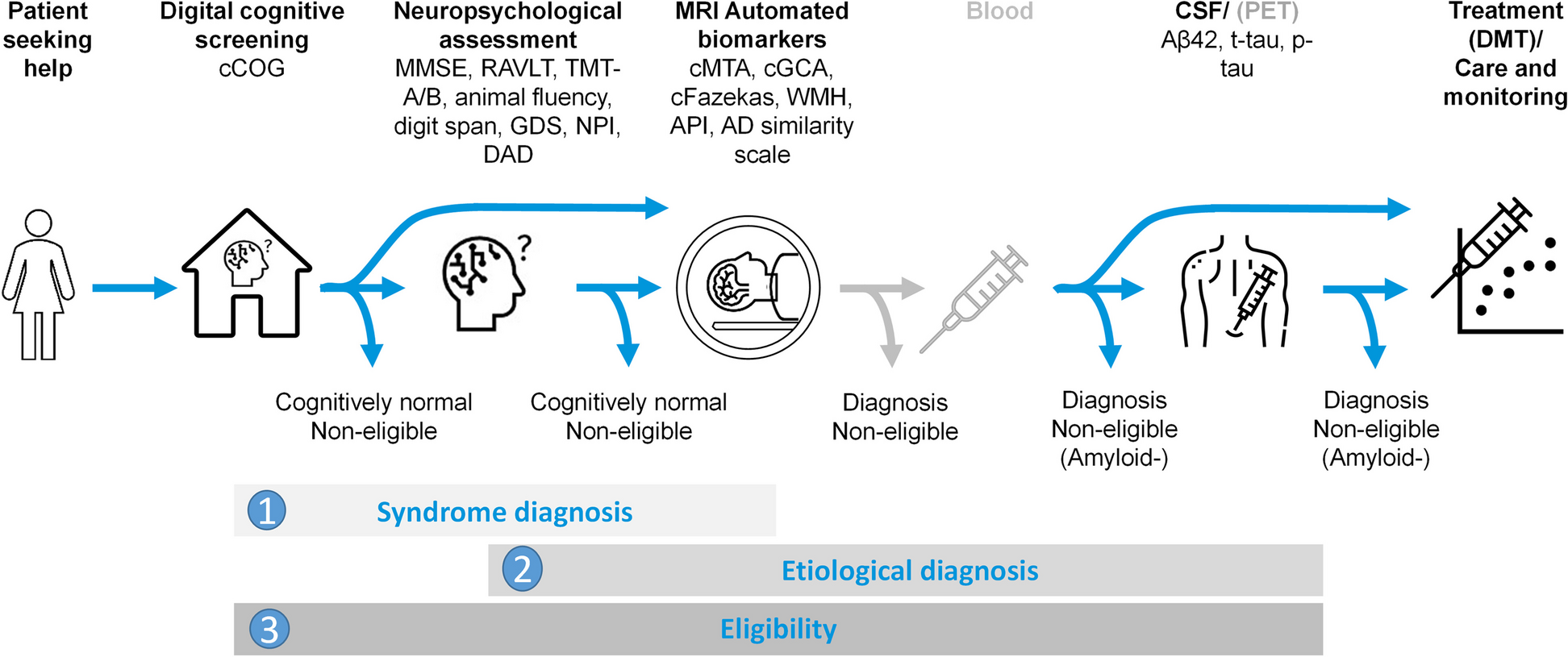
Conduct of the evaluationThe design of the study is presented in Fig. 1.
Fig. 1
Design of the study. In both cases, assessment was done by a trained blinded neuropsychologist. For the Clinical Dementia Rating (CDR) assessment based on medical record, nurse assessment contains information on global cognition (e.g. Mini Mental Stage Examination) and autonomy (e.g. Instrumental Activities of Daily Living), medical consultation contains cognitive screening tests (e.g. Frontal Assessment Battery, 5 words…) and comprehensive neuropsychological battery contains specific tests in cognitive subdomains
The first CDR assessment was carried out during the face-to-face interview between a trained neuropsychologist, the patient and his/her caregiver, as part of the routine care. The second CDR assessment was carried out on the patient’s medical record based on the information available and for which the date does not exceed a period of 2 months with the date of the first CDR assessment. This maximum period of 2 months was set to limit the possibility of changes in the patient’s state of health, which would make the comparison irrelevant.
The CDR assessment on patient’s medical record was performed by neuropsychologists who read and analyzed the information on the medical records based on what they deemed necessary to determine the CDR-SB scores. The neuropsychologists who assessed the CDR scale have all received a 9-hour training course aimed at standardizing practices and therefore inter-rater reliability (https://knightadrc.wustl.edu/cdr/cdr.htm).
This new assessment was performed blind to the first CDR, and the different CDR scores were also assessed by a different neuropsychologist; procedures were implemented so that the neuropsychologists in charge of analyzing the patient’s medical record did not have access to the first assessment of the CDR.
The assessment of the CDR on patient’s medical record was based on an implicit approach (based on judgment) from the information available rather than an explicit approach (based on strict criteria). The implicit approach took into account that different scales may be used to conduct the patient assessment but that they provide similar information. The implicit approach was therefore closer to the reality as the assessments, available in medical records, may vary from a patient to another. In addition, as part of the standard CDR interview assessment, the scoring appeals to the judgment of the neuropsychologist during the semi-structured interview. Nevertheless, all the information used to determine the CDR scores were collected in a specific table in order to identify whether similar scales were used systematically to evaluate the patients.
In the memory center where the study was conducted, data relating to the evaluation of neuropsychological and functional performances are collected during the memory consultation and during interviews between physicians, nurses, neuropsychologists, the patients and their primary caregivers. The data are entered in an Electronic Health Record system by nursing staff, paramedics and consultation secretaries.
Study outcomes and patient’s characteristicsThe primary outcome was the CDR-SB score (score out of 18) obtained (1) during a face-to-face interview at the memory consultation, and (2) obtained with all the information available in the patient’s medical record for the same patients (case A). This information could be results of the nurse assessment (global cognition and autonomy scales), of the medical consultation (cognitive screening tests…) as well as comprehensive neuropsychological battery.
The CDR-SB score allows to distinguish the following classes: 0 (normal cognition), 0.5-4 (questionable cognitive impairment), 0.5–2.5 (questionable impairment), 3–4 (very mild major NCD/or very mild dementia), 4.5- 9 (mild major NCD/or mild dementia), 9.5–15.5 (moderate major NCD/or moderate dementia), 16–18 (severe major NCD/or severe dementia) [14].
In the CDR scale, the patient’s abilities are assessed based on the information available in six different areas: three areas reflect cognitive abilities: memory, orientation and judgment skills and problem solving, the other three areas reflect the actions of everyday life: outdoor and social activities, domestic and leisure activities, as well as personal care.
The secondary outcomes included:
The CDR-SB score evaluated on file using all the information available in the patient file, except the comprehensive neuropsychological assessment (case B);
The CDR-SB score assessed on file using all the information available in the patient file, except the comprehensive neuropsychological assessment, and the medical doctor’s clinical examination, including cognitive screening tests (case C) ;
The 5-point scale CDR with the five classes: 0: normal, 0.5: very mild dementia, 1: mild dementia, 2: moderate dementia, and 3: severe dementia.
The CDR sub-scores for each of the six cognitive and functional areas evaluated in the CDR carried out in face-to-face interview and on patient’s medical record (memory, guidance and judgment, participation in community life, home and leisure occupations and personal care) were considered.
The possible correspondence between the domains of the CDR and the data used to evaluate the CDR with the patient’s medical record was described before the evaluation (supplement Table 1), nevertheless the neuropsychologists remained free to use the information available and that were relevant for them.
In addition to the information used from the patient’s medical record to assess the CDR-SB scores and CDR sub-scores, the others data collected from the MEMORA cohort were: sociodemographic data (age, sex, education), the current living situation of the patients, the diagnostic stage and probable etiology if determined by the physician in charge of the patient, the global cognitive assessment (MMSE, score/30 [15]), the functional assessment (IADL, score/8 [16], DAD-6, score /18 [17], a scale assessing the caregiver burden (mini-Zarit burden interview, score/7 [18]), and the assessment of behavioral and psychological symptoms (score from the Neuropsychiatry Inventory (NPI, score/144 [19]).
Statistical analysesThe characteristics of the study population were described globally.
The degree of agreement between the CDR-SB scores assessed by face-to-face interview or with the patient’s medical record according to the different cases A, B and C was measured using: the intra-class coefficient (ICC) ((“two-way mixed effects, absolute agreement, and multiple raters/measurement” form). The level of agreement based on the ICC was considered poor with ICC was < 0.5, moderate when ICC was between 0.5 and 0.75, good when ICC was between 0.75 and 0.9, and excellent when ICC was ≥ 0.9 ; and the Bland and Altman method including the Bland and Altman plots for each comparison [20].
The degree of agreement between the face-to-face interview and the patient’s medical records to evaluate the 5-point scale CDR and the CDR sub-scores (for each of the 6 areas) was measured using: the intra-class coefficient (ICC) ((“two-way mixed effects, absolute agreement, multiple raters/measurement” form), and the linearly weighted Cohen’s Kappa coefficient [21]. The degree of agreement using the Kappa coefficients was interpreted as for a coefficient < 0: disagreement, 0.1–0.2: very weak agreement, 0.21–0.4: weak agreement, 0.41–0.6: moderate agreement, 0.61–0.80: strong agreement, ≥ 0.8-1: almost perfect agreement.
The information used by the neuropsychologists in the patient’s medical records was also described by domains.
To evaluate the feasibility of evaluating CDR using the patient’s medical record, the duration of evaluation of the CDR (in minutes) was compared between the methods of assessment using paired t-test. The proportions of evaluation of the CDR scale using the patient’s medical records were described for each case (A, B and C), as the information was not always available to evaluate the CDR in each case.
An alpha level of 0.05 was used for statistical significance; all tests were bilateral. Statistical analyses were performed with SPSS software (version 20, SPSS Statistics Inc.).
A sensitivity analysis was performed to ensure that the agreement between the two methods of evaluation of the CDR-SB assessed by ICC remained similar when removing from the analysis the patients who had evaluation of the CDR conducted twice at different time of their care pathway.
Comments (0)