
Remember me
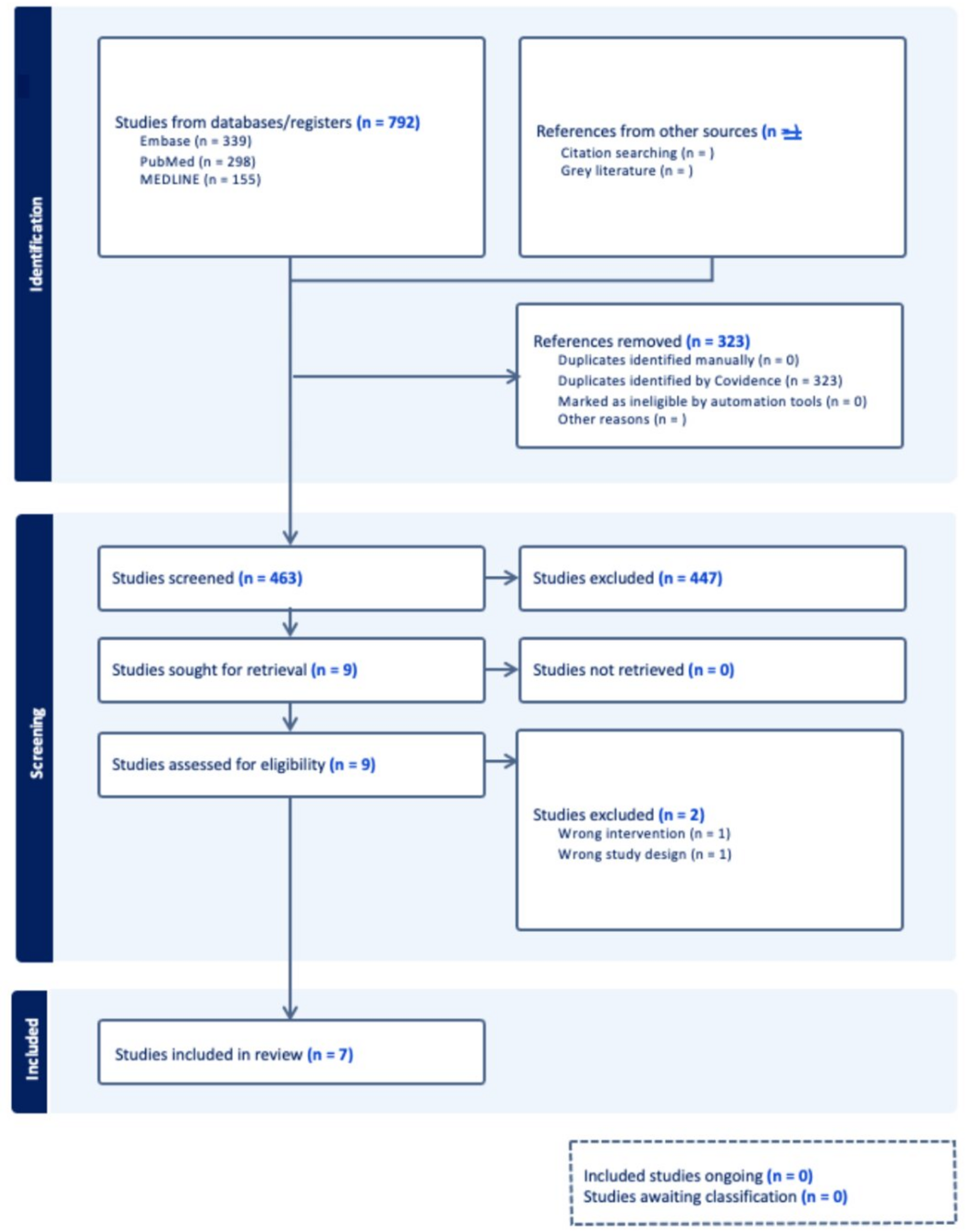
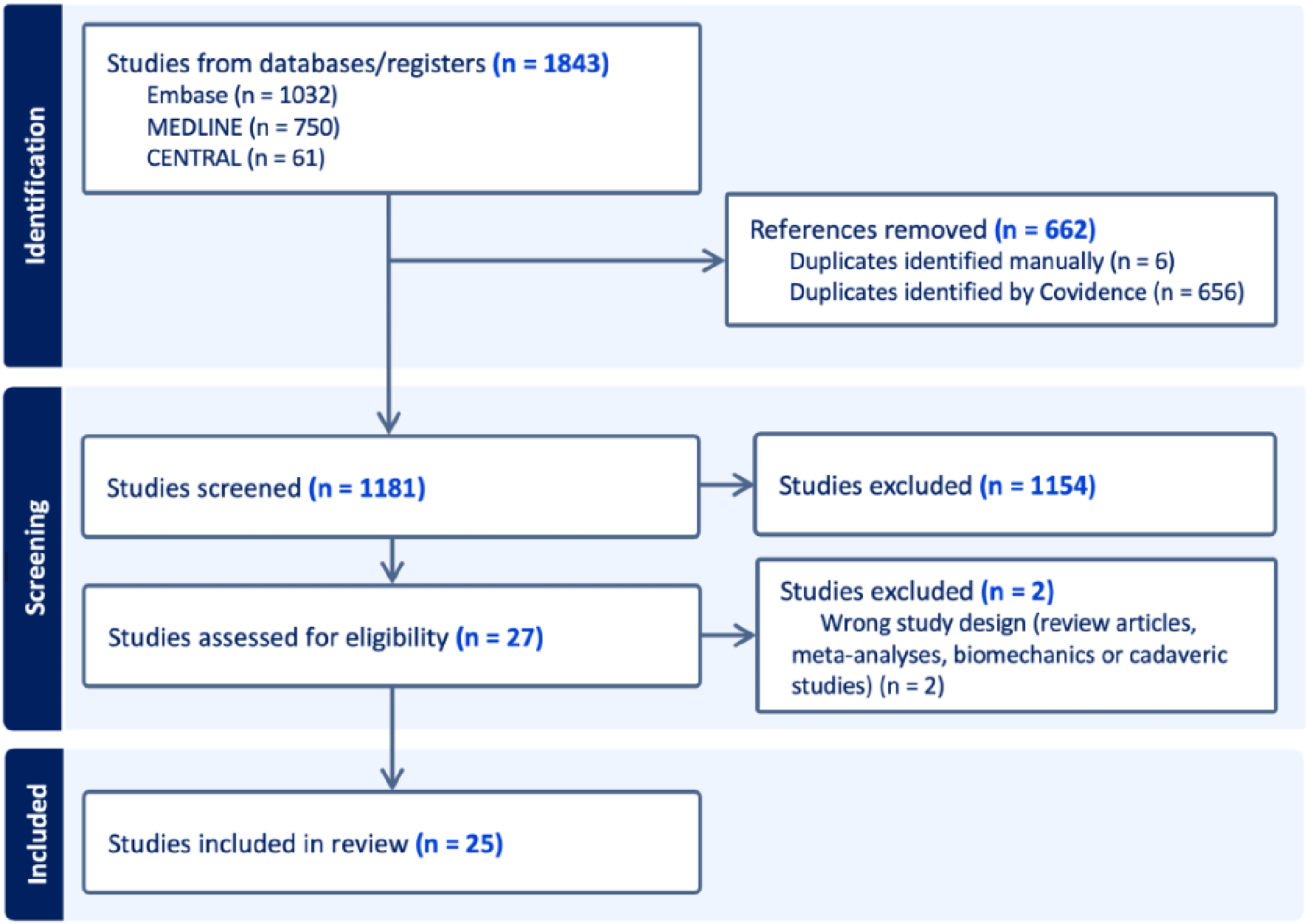


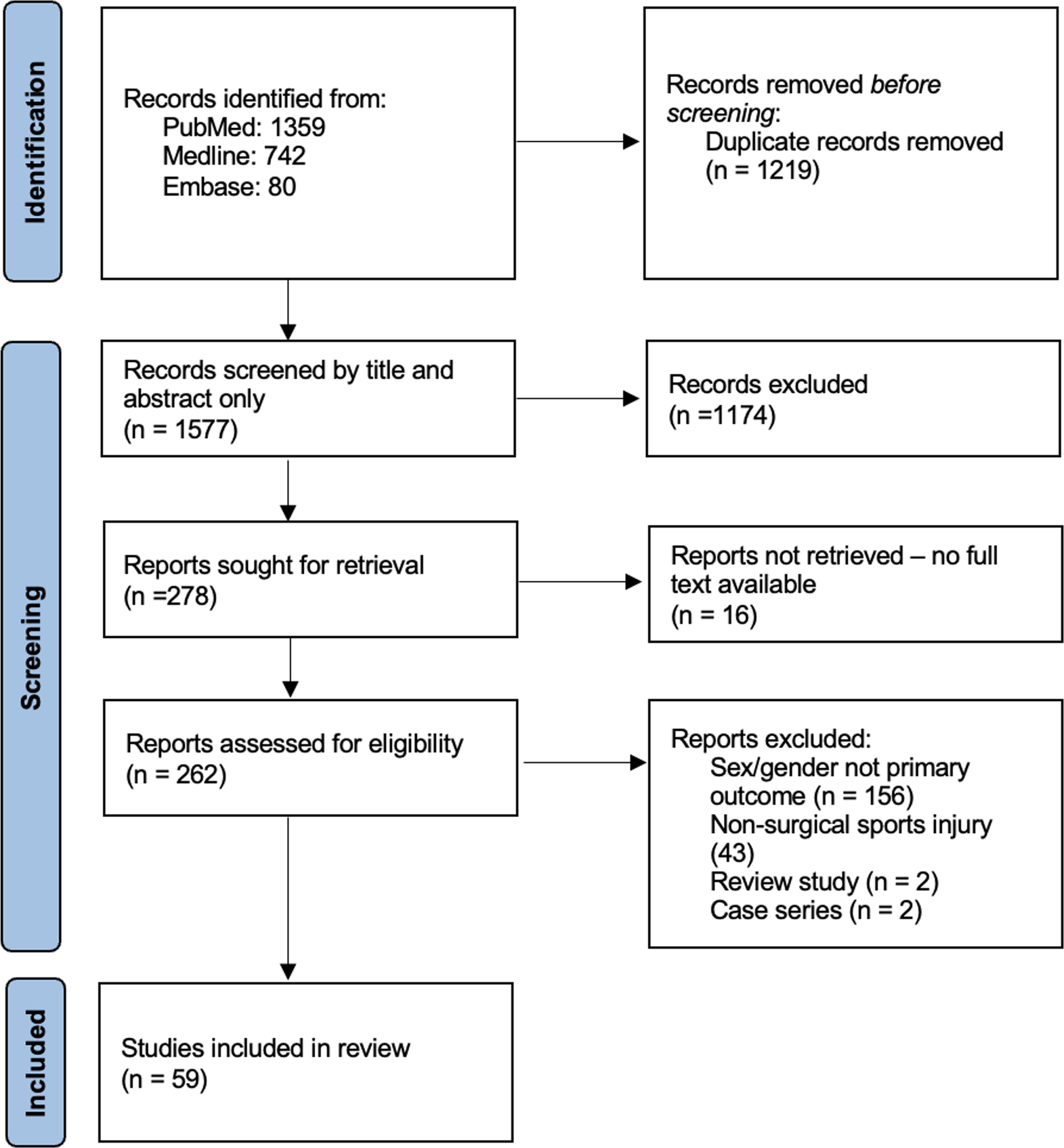



After eliminating duplicates, our initial search yielded 2276 studies. Following title and abstract screening for relevance, 336 studies remained. Subsequent full-text screening based on the specified criteria identified 66 studies that were included in our review (Fig. 1). There were 26 level I (40%), 28 level II (42%), and 12 level III (18%) studies. There were 42 studies focused on knee OA, 5 on rotator cuff tendinopathy, 3 on lateral epicondylopathy, 3 on hip OA, 3 on plantar fasciitis, 2 on patellar tendinopathy, 2 on Achilles tendinopathy, 2 on gluteal tendinopathy, 1 on glenohumeral OA, 1 on carpal tunnel syndrome, 1 on carpometacarpal joint OA, 1 on ankle OCD, and 0 for cubital tunnel syndrome. The PRP preparation and treatment protocols for each of these studies are summarized in Table 1. Platelet dosages are reported in billions and multiples of 106 platelets (1 billion platelets = 1000 × 106 platelets).
Fig. 1
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram
Table 1 PRP Preparation and Treatment protocolsRisk of Bias AssessmentOverall, the risk of bias was low among 40 RCTs (Fig. 2). The risk of bias was highest for blinding participants, personnel, and outcome assessors. Among the remaining studies, the main concerns for bias were due to allocation concealment and incomplete outcome data.
Fig. 2
Risk of Bias graph. risk of bias is presented as a percentage across all included RCT studies
Osteoarthritis (OA)The platelet dosage and efficacy of PRP for the treatment of osteoarthritis at 6 months, 1 year, and 2 years post-injection are summarized in Table 2.
Table 2 Summary of platelet dosage and efficacy of prp for treatment of osteoarthritis at 6 months, 1 year, and 2 years post-injectionKnee OA24 studies were included in the meta and regression analysis. 17 reported WOMAC (Figs. 3), 17 reported VAS (Figs. 4), 10 reported IKDC (Fig. 5), and 6 reported KOOS (Fig. 6).
Fig. 3
(A) Pooled Analysis of Baseline to 6 months in WOMAC for PRP vs. Control by Total Platelet Subgroups, (B) Pooled Analysis of Baseline to 12 months in WOMAC for PRP vs. Control by Total Platelet Subgroups, (C) Meta Regression Analysis for WOMAC at 6 months, and (D) Meta Regression Analysis for WOMAC at 12 months. (Platelet Dose x106)
Fig. 4
(A) Pooled Analysis of Baseline to 6 months in VAS for PRP vs. Control by Total Platelet Subgroups, (B) Pooled Analysis of Baseline to 12 months in VAS for PRP vs. Control by Total Platelet Subgroups, (C) Meta Regression Analysis for VAS at 6 months, and (D) Meta Regression Analysis for VAS at 12 months. (Platelet Dose x106)
Fig. 5
Meta Regression Analysis for IKDC at (A) 6 months and (B) 12 months
Fig. 6
Meta Regression Analysis for KOOS Sport at 6 months
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)Pooled analysis from 5 studies with a dose of < 5 billion platelets and mean latest follow-up of at least 6 months demonstrated that the PRP group had a significant difference in subjective WOMAC scores than the comparator groups (Mean Difference (MD), 6.93 [95% CI, 0.05-13.8]; p = 0.05). Analysis from 6 studies with 5–10 billion platelets demonstrated no difference between comparators (MD, -0.32 [95% CI, -4.06,3.42]; p = 0.87). Six Studies with > 10 billion platelets demonstrated a difference in favor of PRP (MD, 14.8 [95% CI, 1.47–28.12]; p = 0.03). The I2 statistic for WOMAC scores was 87%, 92%, and 99% for < 5 billion, 5–10 billion, and > 10 billion platelets respectively.
No studies with 12-month data used < 5 billion platelets. Pooled analysis from 5 studies with 5–10 billion platelets and mean latest follow-up of at least 12 months demonstrated no difference between comparators (MD, -0.11 [95% CI, -5.45-5.23]; p = 0.97). Four studies with > 10 billion platelets demonstrated a near difference in favor of PRP (MD, 9.67 [95% CI, -1.63-20.97]; p = 0.09). The I2 statistic for WOMAC scores was 98% and 99% for 5–10 billion, and > 10 billion platelets respectively.
Meta-regression analysis at 6 months showed a significant trend and demonstrated that larger decreases in WOMAC scores were seen with higher doses of platelets. At 12 months, a consistent trend of greater effect size with increasing platelet dose was seen but the slope was lower than at the 6-month time point (Appendix 2).
No study bias was seen in the Begg and Egger statistics, and a jackknife analysis leaving out each study and recalculating the results showed no change in the overall summary effect sizes.
Visual Analog Scale (VAS)Pooled analysis from 6 studies with a dose of < 5 billion platelets and mean latest follow-up of at least 6 months demonstrated that the PRP group had no difference in subjective VAS scores than the comparator groups (MD, 0.18 [95% CI, -0.71-1.08]; p = 0.69). Analysis from 5 studies with 5–10 billion demonstrated a difference that favored PRP to the comparators (MD, 0.31 [95% CI, 0.06–0.57]; p = 0.01). Six studies with > 10 billion platelets demonstrated a difference in favor of PRP (MD, 1.32 [95% CI, 0.13–2.50]; p = 0.03). The I2 statistic for VAS pain scores was 78%, 0%, and 95% for < 5 billion, 5–10 billion, and > 10 billion respectively.
One study with a dose of < 5 billion platelets and latest follow-up of at least 12 months demonstrated that the PRP group had no difference in subjective VAS scores than the comparator group (MD, 0.5 [95% CI, -0.22-1.22]; p = 0.17). Pooled analysis from 4 studies with 5–10 billion demonstrated no difference between PRP and the comparators (MD, 0.51 [95% CI, -0.35-1.37]; p = 0.24). Four studies with > 10 billion platelets demonstrated a near difference in favor of PRP (MD, 1.58 [95% CI, -0.11-3.27]; p = 0.07). The I2 statistic for VAS pain scores was 75%, and 97% for 5–10 billion, and > 10 billion platelets respectively.
Meta-regression analysis demonstrated a slight trend at 6 months with increasing effect (as measured by VAS) with an increasing number of platelets. No trend was seen at the 12-month evaluation (Appendix 2).
IKDCThere were insufficient studies to run meta-analysis by dosages for the IKDC. Meta-regression analysis at 6 and 12 months for IKDC revealed a significant trend of increased effectiveness with an increasing number of total platelets (Appendix 2).
KOOSThere were insufficient studies to run meta-analysis by dosages for the KOOS. Meta-regression analysis at 6 months for KOOS Sport revealed a trend in significantly decreasing symptoms with an increasing number of total platelets (Appendix 2).
Other Knee OA Studies.
18 knee OA clinical studies were not included in the meta and regression analysis. Out of 4 studies that administered PRP with a dose > 10 billion platelets, 3 reported positive outcomes for the PRP group at 6 months post-injection [12,13,14], and 2 reported positive outcomes at 1 year post-injection [13, 15]. 7 studies had a total PRP dose between 5 and 10 billion platelets. Six of these studies reported positive outcomes for the PRP group at 6 months post-injection [14, 16,17,18,19,20]. Li et al. reported outcomes for the PRP group that were significantly superior to the comparator group at 6 months and 1 year follow-up. Additionally, positive outcomes for the PRP group were reported at 1-year post-injection for 4 studies [16, 18, 19, 21], and at 2 years post-injection for 1 study [16]. The remaining 9 studies administered PRP with a total dose of < 5 billion platelets. 6 studies reported positive outcomes for the PRP group at 6 months post-injection [22,23,24,25,26,27], and 3 studies reported positive outcomes at 1 year post-injection [21, 26, 28]. Two studies reported outcomes for the PRP group that were significantly superior to the comparator group at 6 months follow-up [22, 29].
Hip OAThree studies examined the effect of PRP on hip osteoarthritis. A high-quality RCT compared the effectiveness of three treatment arms: HA, leukocyte-poor PRP (LP-PRP), and the combination of HA with LP-PRP [30]. Every group received 2 injections separated by 2 weeks. The PRP group had a total platelet dosage of 14,020 × 106. All three groups showed significant improvement in total WOMAC scores at 6 months post-injection (p < 0.001). The authors found a significant difference in total WOMAC scores favoring PRP to HA (p = 0.022), as well as favoring the combination of PRP with HA to HA alone (p = 0.007). There was, however, no statistical difference when comparing the combination of PRP with HA to PRP alone.
A retrospective study compared leukocyte-rich PRP (LR-PRP) to a combination injection of both LR-PRP and HA [28]. The total platelet dosage in the PRP injections was 1850 × 106. At one year’s follow-up, there was no significant improvement in Harris hip score (HHS) in either group when compared to baseline scores (p > 0.05).
The last study was a low-quality double-blinded RCT [31]. The authors found that the LP-PRP group (total platelet dosage of 3517 × 106) had significant improvement in the WOMAC scores at 1 year (p < 0.01), however, there was no difference in scores when compared to the HA group at 6 months or 1-year post-injection (p = 0.95 and p = 0.27 respectively).
Glenohumeral OAOne double-blinded RCT of 70 patients with a low risk of bias compared a single injection of PRP with a dose of 4081 × 106 platelets to HA [32]. Improvement was noted in both groups at 2, 3, 6, and 12 months after injection but there was no statistically significant difference between the two. The improvements were observed regardless of osteoarthritis severity.
Carpometacarpal OAOne retrospective cohort study of 19 patients who received a single injection of PRP with a total platelet dosage of 1967 × 106 reported moderate or excellent symptomatic improvement in 68.8% of patients [33]. The mean reported duration of benefit was 15.6 months. The concentration factor for the platelets in the study was 8.8 (+/-4.9).
TendinopathyThe platelet dosage and efficacy of PRP for treatment of tendinopathy at 6 months, 1 year, and 2 years post-injection are summarized in Table 3.
Table 3 Summary of platelet dosage and efficacy of prp for treatment of tendinopathy at 6 months, 1 year, and 2 years post-injectionLateral EpicondylopathyThree articles studied the use of PRP in lateral epicondylopathy and all of them utilized the VAS as the primary outcome measure. In a single-center, prospective RCT, physical therapy was compared to a single injection of LR-PRP [34]. The PRP had a total platelet dosage of 9450 × 106. The authors found improvement in VAS and functional scores as well as MRI severity grade at 6 months follow-up for the PRP group. Additionally, there was a statistically significant difference between the two treatment groups favoring PRP (p < 0.05). Another RCT compared landmark-guided CSI to LP-PRP (total platelet dosage 2469 × 106) for the treatment of chronic refractory lateral epicondylopathy [35]. At one year post-injection, the PRP group significantly outperformed the CSI group in terms of reduction in VAS scores (p = 0.024).
A retrospective study comparing LP-PRP to extracorporeal shock wave therapy (ECSW) found significant improvement in VAS scores at 2 years post-injection for the PRP group (p < 0.001) [36]. However, there was no difference in results as compared to the ECSW group (p > 0.05). The PRP group in this study received four injections for a total platelet dosage of 7200 × 106.
Rotator Cuff TendinopathyFive studies investigated the role of PRP in the treatment of rotator cuff tendinopathy. One prospective cohort study investigated the effects of subacromial PRP injections administered to 50 adults with chronic rotator cuff tendinopathy that was refractory to conservative management [37]. The LR-PRP had a total platelet dosage of 5020 × 106 per injection and was injected via anatomical landmarks. A second PRP injection was administered for 6 (12%) patients at the 3-month follow-up if there was no significant improvement in pain and functional scores, and new injuries were ruled out by MRI. At 12 months follow-up, there was a significant improvement in VAS, Constant, and the American Shoulder and Elbow Surgeons (ASES) scores (p < 0.001 for all).
One RCT compared exercise therapy to PRP for the treatment of subacromial impingement. Patients in the PRP group received two injections of LR-PRP (total platelet dosage of 7200 × 106) that were spaced one month apart [38]. A portion of each PRP injection was injected intra-tendinous under ultrasound guidance, while the remainder of the injectate was directed at the subacromial space using landmark guidance. The PRP group achieved a significant reduction in VAS pain scores at 6 months post-injection (p < 0.01), however, there was no difference between treatment arms.
In a double-blinded RCT, patients were randomized to receive 4 weekly injections of either normal saline, sodium hyaluronate, LP-PRP, or the combination of sodium hyaluronate with PRP [39]. The total platelet dosage after 4 injections was 16,000 × 106. All injections were completed under ultrasound guidance into the subacromial space. The sodium hyaluronate, PRP, and the combination sodium hyaluronate with PRP groups all had significant improvement in ASES, Constant, and VAS scores at 3, 6, and 12 months when compared to baseline (p < 0.05 for all). The PRP and the combination of sodium hyaluronate with PRP groups both showed significantly greater improvements in these pain and functional scores over the same follow-up time intervals as compared to normal saline and sodium hyaluronate groups (p < 0.01 for all).
Two RCTs compared LP-PRP injections to CSIs into the subacromial space. In one double-blinded study, the PRP had a total platelet dosage of 3956 × 106. At 6 months follow-up, the Constant score improved significantly above baseline in the PRP group, however, there was no difference between the two treatment arms [40]. In the other RCT, the PRP had a total platelet dosage of 3924 × 106 [41]. The reduction in pain severity as measured by the Neer Pain score was not statistically different between the two treatment arms at 6 months or 1-year post injection (p = 0.155 and p = 0.081 respectively). There was, however, a significant difference in improvement of shoulder abduction at 12 months follow up favoring the PRP group (p = 0.012).
Gluteal TendinopathyTwo RCTs assessed the efficacy of PRP in gluteal tendinopathy. One RCT of 80 patients with some concern for risk of bias compared a CSI to a single injection of PRP with a platelet dose of 6266 × 106 [42]. The PRP group improved significantly in the Modified Harris Hip Score (MHHS) from baseline (53.77; SD, 12.08) to 12 (74.05; SD, 13.92), 24 (77.6; SD, 11.88), 52 (78.18; SD, 14.53) and 104 weeks (82.59; SD, 9.71) versus the CSI at 24 weeks (65.82; SD, 15.28). In this study, there was a crossover group for which 27 patients were deemed to have failed CSI with an exit score of 59.22 (SD,11.54). The crossover group improved with the LR-PRP: from 59.22 (SD, 11.22) at baseline to 75.55 (SD, 16.05) at 12 weeks, 77.69 (SD, 15.30) at 24 weeks, and 77.53 (SD, 14.54) at 104 weeks. Another RCT of 48 patients with a high risk of selective reporting bias compared a single injection of PRP with a dosage of 6161 × 106 to normal saline [43]. There was a reduction in worst, average, and least pain over time, but no difference between the two groups at 3,6, or 12 months. The injections in this study were done without the use of image guidance.
Patellar TendinopathyTwo RCTs examined the outcomes in patients with patellar tendinopathy after receiving PRP. In both studies, the primary outcome was the Victorian Institute of Sport Assessment for Pain (VISA-P). One RCT studied single-dose LR-PRP versus LP-PRP versus saline injections [44]. Platelet dosages used in this study were 3059 × 106 and 2384 × 106 in the LP-PRP and LR-PRP groups respectively. Though VISA-P scores improved at 6 months and 1-year post-injection in both PRP groups, the authors found no difference in mean change in VISA-P scores among all treatment groups (p > 0.05 for all outcomes). In the other RCT, which was double-blinded, outcomes were compared between those who received two injections of LP-PRP (total platelet dosage 6756 × 106) versus bone marrow mesenchymal stem cells [45]. The PRP group experienced significant improvement in VISA-P scores from baseline (47.00, SD 9.83) to 6 months post-treatment (72.90, SD 17.34; p = 0.0009), however, there was no statistical difference in scores between the two treatment arms (p = 0.6776).
Achilles TendinopathyTwo studies investigated the efficacy of LP-PRP in Achilles tendinopathy using the Victorian Institute of Sport Assessment for Achilles (VISA-A) as the primary outcome measure. A retrospective study investigated the difference in patient outcomes in those with insertional Achilles tendinopathy who received either two injections of LP-PRP (total platelet dosage 3980 × 106) or three sessions of ECSW [46]. The PRP group experienced significant improvement in VISA-A scores at 6 months (82.0, SD 18.1) as compared to baseline (52.8, SD 14.2; p < 0.001), but there was no statistical difference in improvement when compared to the ECSW group (p = 0.368). Similarly, in an RCT comparing LP-PRP to adipose-derived stromal vascular fraction (SVF) injection, there was no statistical difference between groups at 6 months post-intervention (p > 0.05), though VISA-A scores improved significantly from baseline (p < 0.001) [47]. The platelet dosage used in this study was 3252 × 106.
Plantar FasciitisThe efficacy of PRP in plantar fasciitis was investigated in three studies. All three studies utilized the VAS as the primary outcome measure. Two of the three studies were RCTs that compared single landmark-guided PRP injection to CSI, and both RCTs injected PRP with a total platelet dosage of 3000 × 106 [48, 49]. In one of the RCTs, not only did the PRP group report improvement in VAS scores at 6 weeks, 3 months, and 6 months post-injection, but there was also a significant difference in VAS scores between the two treatment arms at all three-time intervals (p < 0.007, p < 0.001, p < 0.001 at 6 weeks, 3 months, and 6 months respectively) favoring the PRP group [48]. The PRP group also had a significant reduction in plantar fascia thickness as assessed by ultrasound 6 months post-injection when compared to the corticosteroid group (p < 0.0003). The authors of the second RCT found similar results though their study was of lower quality evidence. Both PRP and CSI groups found improvement in VAS scores at 6 weeks, 3 months, and 6 months post-injection [49]. When compared between the two groups, there was a significant reduction in VAS scores that favored the PRP group at all time intervals. Moreover, the PRP group experienced a larger sonographic reduction in plantar fascia thickness at 6 months post-injection as compared to the CSI group (p = 0.0001).
One retrospective study compared PRP to ECSW among athletes and non-athletes [50]. The PRP group received 3 injections, with a total platelet dosage of 5400 × 106. At 2 years follow-up, the PRP group reported statistically decreased VAS scores (p < 0.001) in both the athlete and non-athlete subgroups, however, there was no difference in VAS score improvement when compared to those who received ECSW (overall population: p = 0.485, athletes: p = 0.433, nonathletes: p = 0.064).
Other MSK ConditionsThe platelet dosage and efficacy of PRP for treatment of other MSK conditions at 6 months, 1 year, and 2 years post-injection are summarized in Table 4.
Table 4 Summary of platelet dosage and efficacy of prp for treatment of other msk conditions at 6 months, 1 year, and 2 years post-injectionCarpal Tunnel SyndromeOne prospective cohort study examined the effects of LP-PRP versus corticosteroid injection in treating carpal tunnel syndrome [51]. The platelet dosage used in this study was 3064 × 106, and the injection was done by landmark guidance. At 6 months post-intervention, there was no significant improvement on the Boston Carpal Tunnel Questionnaire (BCTQ) for the PRP group (2.41, SD 0.36; p = 0.724 and 1.91, SD 0.18; p = 0.601 for the symptom severity and functional status respectively). Additionally, there were no statistical differences in BCTQ scores at 6 months follow-up when compared to the corticosteroid group (p = 0.645 and p = 0.861 for the symptom severity and functional status respectively).
Ankle Osteochondral Defect (OCD)One retrospective cohort study of 49 patients compared 3 injections of PRP for a total dosage of 12,084 × 106 to prolotherapy (PrT) [52]. The average lesion size for these patients was 1.54 cm2 in the PRP group and 1.64 cm2 in the PrT group respectively. Both groups improved at 21 days, 3 months, 6 months, and 12 months with no difference between the two. The average lesion size was significantly lower in patients with excellent or good outcomes (1.43 ± 0.68 cm2 and 1.42 ± 0.63 cm2 for PrT and PRP groups, respectively) compared to patients with fair or poor outcomes (2.6 ± 1.21cm2 and 2.25 ± 0.2cm2 for PrT and PRP groups, respectively).
Comments (0)