Patient selection
From April 2021 until April 2022, all consecutive patients with a recent primary breast cancer diagnosis or patients with a recurrent breast cancer diagnosis requiring further imaging evaluation as part of their diagnostic work-up according to the current national breast cancer guideline, in terms of locoregional (breast MR) and distant staging ([18F]FDG WB PET-MR), were included in the current study. According to the Dutch breast cancer guideline in 2018, distant staging with [18F]FDG examination can be considered in recently diagnosed breast cancer patients with tumor size larger than 50 mm (i.e., clinical tumor status (cT) 3–4), presence of axillary lymph node metastasis (i.e., clinical nodal status (cN) 1–3) with the potential of neoadjuvant systemic therapy or recurrent breast cancer [9].
Breast cancer diagnosis was confirmed with core-needle biopsy, to obtain histopathologic information including receptor status (estrogen (ER), progesterone (PR) and Human Epidermal growth factor Receptor 2 (HER2)). In the case of suspicious axillary lymph node findings, the core-needle biopsy was performed to confirm axillary lymph node metastases. In the case of suspicious distant metastases on imaging findings, the biopsy was performed to confirm distant metastases of at least one suspicious lesion.
Medical ethical approval was obtained for this single-center feasibility study (METC 2022-3121). The necessity to acquire informed consent from study subjects was waived by the local medical ethics committee.
Conventional imaging
Conventional imaging consisted of FFDM performed on a Senographe Essential (GE Healthcare, Chalfont St Giles, UK). In addition, breast and axillary ultrasound (US) was performed on an RS80A ultrasound system (Samsung Medison Co., Ltd., Seoul, South Korea) with a 3–12 MHz linear array transducer.
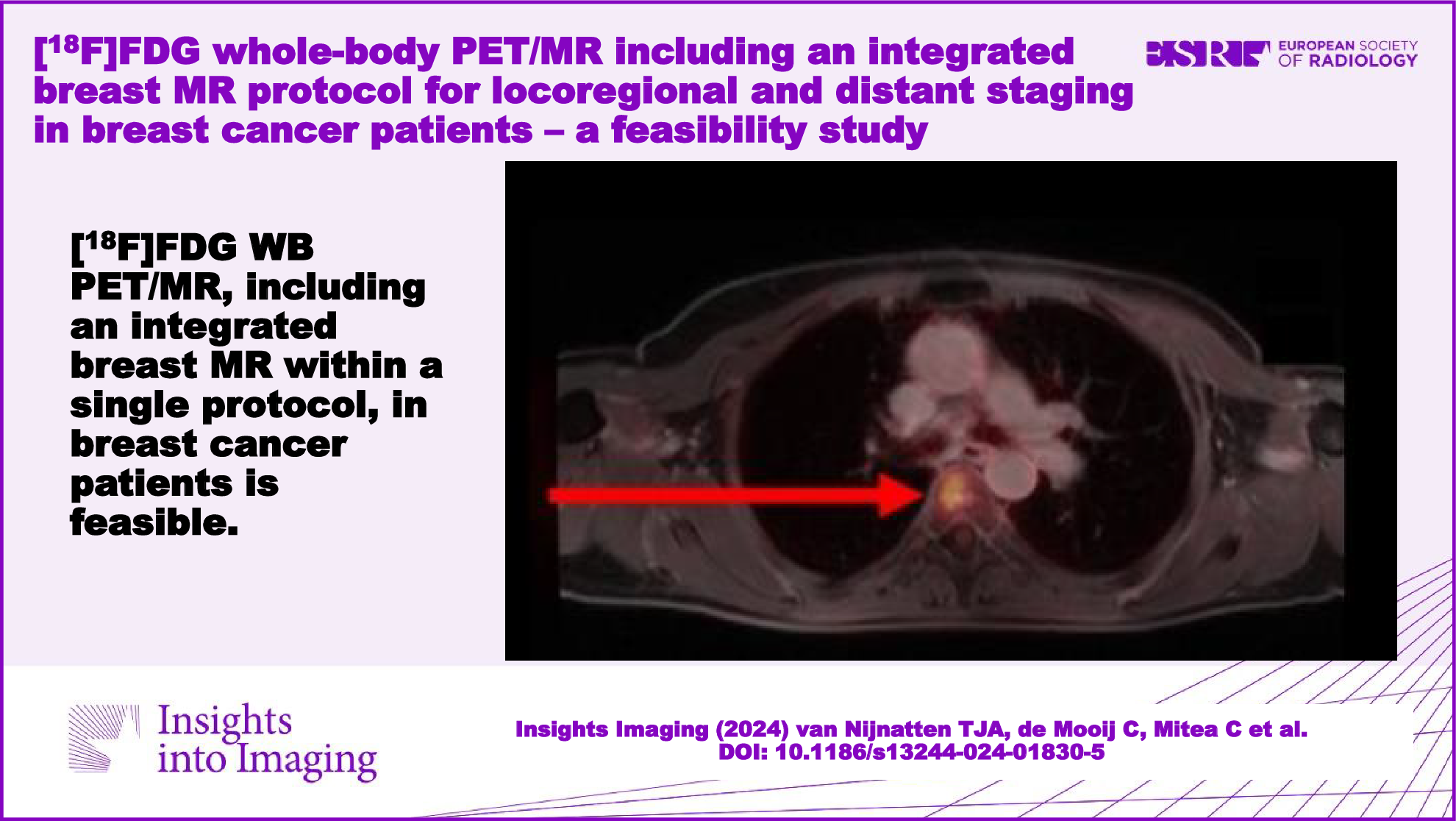
Imaging protocol: [18F]FDG WB PET-MR including integrated breast MR
Before administration of the tracer 3 MBq/kg bodyweight [18F]FDG, patients fasted for at least four hours. Blood glucose levels were verified to be lower than 11 mmol/L. All exams were performed on a 3.0-T PET-MR system (Biograph mMR; Siemens Healthineers, Erlangen, Germany).
After a resting period of 30 min after administration of [18F]FDG, patients were placed on the PET-MR system in a prone position with elevated arms, using a 16-channel breast coil (Rapid Biomedical, Rimpar, Germany) to perform the breast MR. The breast MR protocol consisted of a two-dimensional T2W turbo spin-echo sequence without fat suppression, diffusion-weighted imaging (DWI) with fat suppression (B-values 50, 150 and 800, respectively) and, after injection of the gadolinium-based contrast agent Gadobutrol (Gadovist®, Bayer Health Care, Berlin, Germany), a dynamic contrast-enhanced (DCE)-T1W sequence with fat suppression, in accordance with the reported breast MR protocol preferences of the European Society of Breast Imaging [4] (Table 1).
Table 1 Overview of breast MR and ([18F]FDG) WB PET-MR protocolsApproximately 55 min after administration of [18F]FDG, patients were switched from a prone position to a supine position in order to perform the [18F]FDG WB PET-MR. The protocol consisted of WB fat-suppressed contrast-enhanced T1W sequence, WB T2W sequence, and DWI of the liver region (B-values 50, 800 and 1400, respectively) (Table 1), by using the primary WB coil of the PET/MR system.
Three-dimensional iterative reconstruction was performed for the PET images of the PET-MR system, with automatic attenuation correction by implementation of a four-compartment model attenuation map (Dixon-based μ-map).
Image evaluation
All breast MR exams were evaluated according to the fifth edition of the BI-RADS lexicon in consensus by two readers, a final-year resident in breast imaging (T.v.N.) and a breast radiologist (J.H.) with more than 15 years of breast imaging experience, by using software on a Sectra Workstation IDS7 (version 23.1.10, Sectra Group, Linköping, Sweden). The total number of suspicious regional lymph nodes on breast MR was based on previously described criteria, including irregular margins, inhomogeneous cortex, perifocal edema, absence of the fatty hilum, asymmetric lymph nodes as opposed to the contralateral side, and absence of chemical shirt artefacts [10].
All [18F]FDG WB PET-MR exams were evaluated according to the recommendations of the Society of Nuclear Medicine and Molecular Imaging for oncological [18F]FDG PET/CT and recent consensus recommendations on [18F]FDG WB PET-MR for oncology in consensus by two readers, a final-year resident in nuclear medicine (T.v.N.) and a nuclear medicine physician (C.M.) with more than 10 years of experience in nuclear medicine, by using a dedicated post-processing environment including state-of-the-art software (Syngo.via 6.4 as software, Siemens Healthcare, Erlangen, Germany) [11, 12]. The total number of suspicious regional lymph nodes on [18F]FDG WB PET-MR was based on the number of hypermetabolic lymph nodes.
Statistical analysis
Findings on [18F]FDG WB PET-MR, including integrated breast MR, were compared to conventional imaging findings (i.e., FFDM and US) in terms of clinical tumor size (cT), clinical nodal status (cN) and distant status (cM), according to the 8th edition of TNM classification. Descriptive statistics were performed using SPSS software (version 27, IBM Corp., Armonk, NY, USA).


Comments (0)