
Remember me



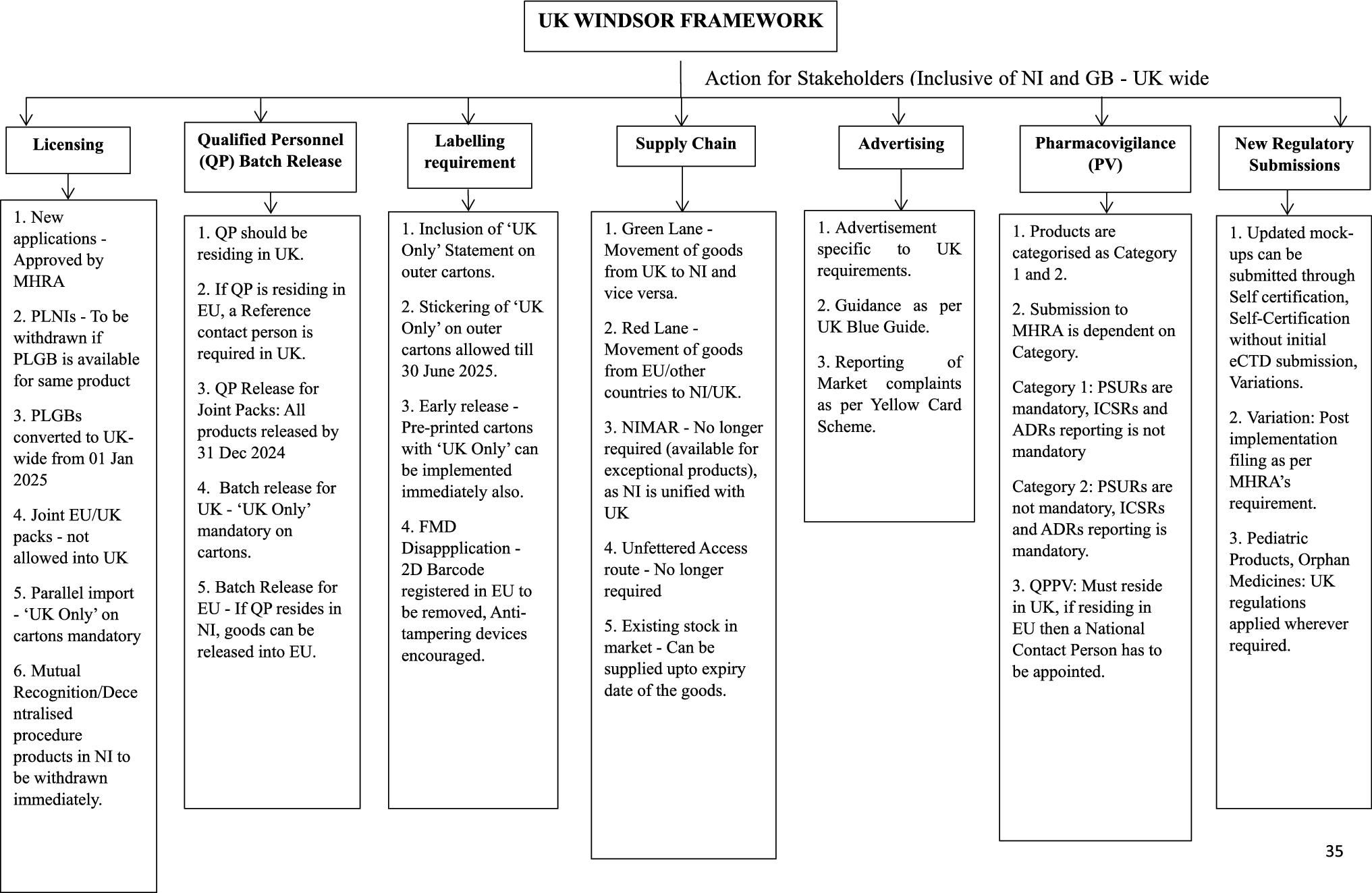




The PEBB framework in this analysis followed the steps described in Fig. 1. First, pharmacometric modeling of the exposure-response relationship of empagliflozin and linagliptin was performed based on available historical data in adults and pediatric patients with T2D. Second, these models simulated individual and placebo-corrected mean changes in HbA1c at 26 weeks in a pediatric population with baseline characteristics matching the DINAMO population in relevant covariates. Third, the prior distribution was robustified with a weakly-informative mixture component to allow for the possibility of prior-data conflict. Prior weights for the informative and non-informative components were determined in advance based on feedback from clinical experts and the U.S. Food and Drug Administration (FDA) and were constrained to yield prior distributions with effective sample sizes (ESS) less than or equal to the observed sample sizes in DINAMO. Fourth, the posterior distribution was derived, combining the prior distribution with the DINAMO results. The prior was automatically updated based on data for the posterior distribution. Fifth, the posterior distribution was summarized, providing an estimate of the treatment effect that represents the totality of evidence from both DINAMO data and historical data. Finally, sensitivity analyses were performed using alternative weights for the informative component of the prior.
Fig. 1
Schematic workflow of Bayesian borrowing analysis
Data Sources and Primary AnalysisData used for the empagliflozin pharmacometric models included 14 phase II and III trials (Table S1). Data for the linagliptin pharmacometric models included 8 phase II and III trials (Table S2). Of these 22 trials, 20 were conducted in adults with 2 pediatric trials [15, 16], including 66 participants. In the DINAMO trial, a total of 157 participants received either empagliflozin (10 mg or 25 mg; n = 52), linagliptin 5 mg (n = 52), or placebo (n = 53) [3]. The primary DINAMO trial analysis was performed with an analysis of covariance (ANCOVA) adjusted for treatment, baseline HbA1c, and baseline age group. At week 26, treatment with linagliptin did not provide a significant improvement in HbA1c compared with placebo [placebo-adjusted treatment difference − 0.34% (95% confidence interval [CI] − 0.99 to 0.30; p = 0.29)]; however, treatment with empagliflozin was superior in reducing HbA1c from baseline versus placebo [placebo-adjusted treatment difference − 0.84% (95% CI − 1.50 to − 0.19, p = 0.012)].
Software for AnalysesSoftware details for the pharmacometric models and Bayesian borrowing analyses appear in Supplementary Materials.
Pharmacometric ModelsAll pharmacometric models were prespecified prior to unblinding of DINAMO data.
PK Sampling and Bioanalytical AssaysDetails of the blood sampling and bioanalytical methods for measurement of empagliflozin and linagliptin plasma concentrations used in PopPK models appear in Supplementary Materials and Table S3.
Empagliflozin PopPK Model DevelopmentA previously developed two-compartmental PopPK model in adults with T2D [17] was updated for use in the pediatric population. Three additional trials were included [15, 18, 19], with a fourth trial [20] providing external validation. Some structural simplifications were made regarding absorption and covariate inclusion. Observed absorption lag, evident in some participants, was modeled with a sequential zero-first-order absorption process, rather than the discontinuous absorption lag time (ALAG) parameter previously used. Given limited number of laboratory measures collected in the single pediatric PK trial [15], a limited number of covariates were analyzed (Table S4). Allometric scaling with body weight was added into the model to facilitate translation of the PopPK model between adult and pediatric groups to account for changes in clearance and volume due to potential differences in weight for pediatric patients [21]. Further information on model development appears in Supplementary Materials.
Empagliflozin PK-PD Model DevelopmentA previous pharmacokinetic-pharmacodynamic (PK-PD) model in adults [17] was updated for the pediatric population. As fasting plasma glucose (FPG) was not densely sampled in the single included pediatric PK trial [15], the updated model removed FPG which was previously an intermediary between empagliflozin exposure (AUC) and HbA1c changes. Covariate relationships were pre-specified (Table S4) with the updated model incorporating effects of concomitant medications (insulin, metformin, and sulfonylurea) commonly used in pediatric patients with T2D.
An indirect response model described the effect of empagliflozin exposure on HbA1c. HbA1c modeling used a turnover model parameterized as baseline HbA1c, HbA1c synthesis rate constant (kin), an HbA1c first-order degradation rate constant (kout), with empagliflozin inhibiting the kin parameter through a maximum inhibition (Imax) relationship. A placebo effect was also incorporated, which affected the kout parameter. Area under the concentration-time curve for a dosing interval at steady state (AUCss) producing half-maximal inhibitory effect (AUC50) for the drug effect was fixed to 703 nmol·h/L, the value estimated in a previous PK-PD model that included FPG [17]. Covariates selected for evaluation included background medications used in DINAMO participants, renal function, and baseline HbA1c (Table S4). Further information on model development appears in Supplementary Materials.
Linagliptin PopPK Model DevelopmentA previously developed two-compartmental PopPK model in adults with T2D [22,23,24] was updated to be more parsimonious and enable accommodation of PK data from pediatric participants. Due to the non-linear PK of linagliptin, there was difficulty in modeling all available linagliptin PK data (early and late phase studies). This was overcome by using a subset of data (the analysis-model dataset) from 5 well-controlled, early-phase trials [16, 25,26,27,28] to characterize the structural model and for parameter estimation.
A limited number of covariates were analyzed in the analysis-model dataset (Table S4), with the final model using a greater number of covariates to generate maximum a posteriori (MAP) Bayes parameter predictions for a broader dataset that included another 3 linagliptin trials [29,30,31] (known as the empirical Bayes estimates (EBE)-model dataset) to obtain exposures for HbA1c modeling. Further information on model development appears in Supplementary Materials.
Linagliptin PK-PD Model DevelopmentAs a starting point, the exposure-response relationship between HbA1c lowering and linagliptin exposure used a turnover model for HbA1c. AUCss provided the exposure response relationship; with sequential modeling of placebo and exposure responses implemented as necessary (See Supplementary Materials for further details).
Data from all trials was used in model development except in those where HbA1c was not collected [25]. Covariates selected for evaluation included background medications (metformin, insulin) in anticipation of the DINAMO sample (Table S4).
Model Selection and EvaluationStandard model selection and discrimination criteria were used in the development of pharmacometric models (see Supplementary Materials for further details). Models providing best description of data without any unacceptable trends in goodness-of-fit (GOF) plots were used [32]. Final pharmacometric model parameter estimates were reported with an estimation measure of uncertainty including 95% credible intervals (CDIs) from the posterior parameter distributions of Bayes runs and 95% CIs derived from asymptotic standard error estimates or non-parametric bootstrap.
The final PopPK and PK-PD models were qualified by inspection of longitudinal visual predictive checks (VPCs) [33], prediction-corrected VPCs (pc-VPCs) [33], and by NPDE [34] plots (see Supplementary Materials for further details). The impact of covariates on PopPK and PK-PD models was assessed by examining forest plots of changes in apparent clearance after oral dosing (CL/F) and HbA1c change from baseline, respectively.
Model SimulationsWe conducted 5,000 simulations using the developed PopPK and PK-PD models for empagliflozin and linagliptin in an iterative manner for a total of 5,000 iterations. In each iteration, 5,000 patients (empagliflozin and linagliptin) were resampled without stratification using blinded demographic and background medication data from DINAMO (158 randomized participants). The simulations mimicked the design specifications of DINAMO (treatment groups and re-randomization at week 14) and generated placebo-corrected mean changes from baseline for HbA1c (%) to serve as prior information for the Bayesian borrowing analyses. Further details about simulations appear in Supplementary Materials.
Bayesian Borrowing Analysis Based on Exposure-Response ModelPrior CalculationBayesian inference compared the mean change in HbA1c from baseline to week 26 between empagliflozin and placebo, as well as between linagliptin and placebo. This is referred to as the placebo-corrected treatment effect of empagliflozin and linagliptin, respectively. Partial exchangeability of relevant historical, mostly adult clinical trial data informed the treatment comparison and increased the precision of estimates.
To minimize bias of partial exchangeability, the PK-PD models described above in adults generated a covariate-adjusted mean prediction of HbA1c responses in a pediatric population using the participant characteristics of DINAMO. This was considered acceptable based on the confidence in describing differences in exposure after allometric scaling by weight and previous comparable responses for short-term markers of efficacy (e.g. urinary glucose excretion [UGE] for empagliflozin [Boehringer Ingelheim, data on file], and DPP-4 inhibition for linagliptin [35]) in pediatric patients with T2D relative to adults.
Random samples of the predicted placebo-corrected treatment effect distributions informed the prior distributions for Bayesian analysis. To reduce the impact of potential discrepancies between historical and new HbA1c predictions and prevent prior-data conflict, the prior distribution was robustified by adding a weakly-informative mixture component to the calculated prior [36]. The robust component of the prior dynamically down weights the informative component of the prior (i.e., that derived from adult pharmacometric models) in cases of prior-data conflict. Separate analyses were performed for empagliflozin and linagliptin.
Since pharmacometric model predictions were based on predominantly adult participants with limited pediatric data, there was uncertainty about the information content in the pharmacometric model predictions. Expert input from members of the DINAMO steering committee helped to assess the ESS of the prior and weight of the informative part of the prior. The experts determined that an ESS of at most 100 participants per treatment group reflected a consensus degree of confidence in the covariate-adjusted pharmacometric model predictions. If the ESS implied from the pharmacometric simulation was greater than 100, then the variance of the informative prior would be down-weighted accordingly to correspond to an ESS of 100. This was in line with recommendations to derive priors that give the data a chance to influence the outcome of a trial in a pediatric setting where adult data may otherwise outweigh the pediatric data [37].
Based on feedback from the FDA, the maximum number of effective borrowed patients as determined by the calculated ESS of the prior distribution (as opposed to the ESS for the informative component) was adjusted to be no more than the sample size of each treatment group of DINAMO (~ 52 patients per treatment group). To fully utilize the informative part of the prior up to the limit defined by FDA, the (pre-specified) weight for the informative part of the prior was set to 0.65 (with a non-informative weight 0.35), resulting in an approximate overall ESS of the prior of 51 patients per treatment group (i.e., less than the total number of enrolled participants in each treatment group). Sensitivity analyses were conducted using a full range of alternative weights.
ESS was calculated with the expected local information ratio (ELIR) method [38]. Further details and key equations for this section appear in Supplementary Materials.
Posterior Calculation and Decision RuleThe posterior distributions were used to describe and evaluate the placebo corrected treatment effects for empagliflozin and linagliptin, separately, and to perform statistical inference. The posterior distribution of the treatment effect was calculated from the prior and the observed placebo-corrected treatment effect in DINAMO.
The pre-specified decision rule to determine efficacy of each treatment was based on comparison of the 97.5% quantile of the posterior treatment effect with 0. If the decision criterion was met (i.e., posterior distribution value for 97.5% quantile was less than 0), then there was evidence of superior efficacy of each treatment in the DINAMO sample (See Supplementary Materials for further details).
Operating CharacteristicsThe frequentist operating characteristics (i.e., power and type I error) for the Bayesian borrowing analysis were calculated for a set of scenarios with varying assumptions about the true placebo-corrected treatment effect in the DINAMO trial. They were also calculated for alternative choices of the informative prior part weight and ESS to assess robustness of the choice of weight and ESS [39]. As shown in Table S5, using prior means for empagliflozin (\(\:_\)) and linagliptin (\(\:_\)) equal to − 0.55, an informative part ESS of 100 per treatment group and informative prior weights for empagliflozin (\(\:_\)) and linagliptin (\(\:_\)) equal to 0.65, a good trade-off is obtained between power gains through borrowing and the need to limit the type I error inflation. With these operating characteristics, the probability of meeting the decision criterion with evidence level of 97.5% is 79.3% for empagliflozin and 76.9% for linagliptin (scenario 10 in Table S5). This scenario corresponds to the placebo-corrected treatment effect assumed in the sample size calculation of DINAMO. This represents a considerable improvement over the 40.1% (empagliflozin) and 37.7% (linagliptin) probability at the 97.5% evidence level where a weakly informative prior (\(\:_\) = \(\:_\) = 0) is used (scenario 18 in TableS5). The use of the informative prior increases also the false positive decision probability. For example, there is a 19.0% (empagliflozin) and 18.5% (linagliptin) probability of falsely meeting the decision criterion when there is no treatment benefit (scenario 12 in Table S5). This increase beyond the significance level chosen in the DINAMO protocol was considered acceptable (See Supplementary Materials, Tables S5/S6 and Figures S2/ S3 for further details).
Sensitivity AnalysesWe performed a tipping point sensitivity analysis with alternative prior weights (range 0 to 1) for the informative component [40] (see Supplementary Materials for further details). In sensitivity analyses for the posterior, inference was also performed with lower decision rule thresholds (95% and 90% quantiles).
Comments (0)