
Remember me




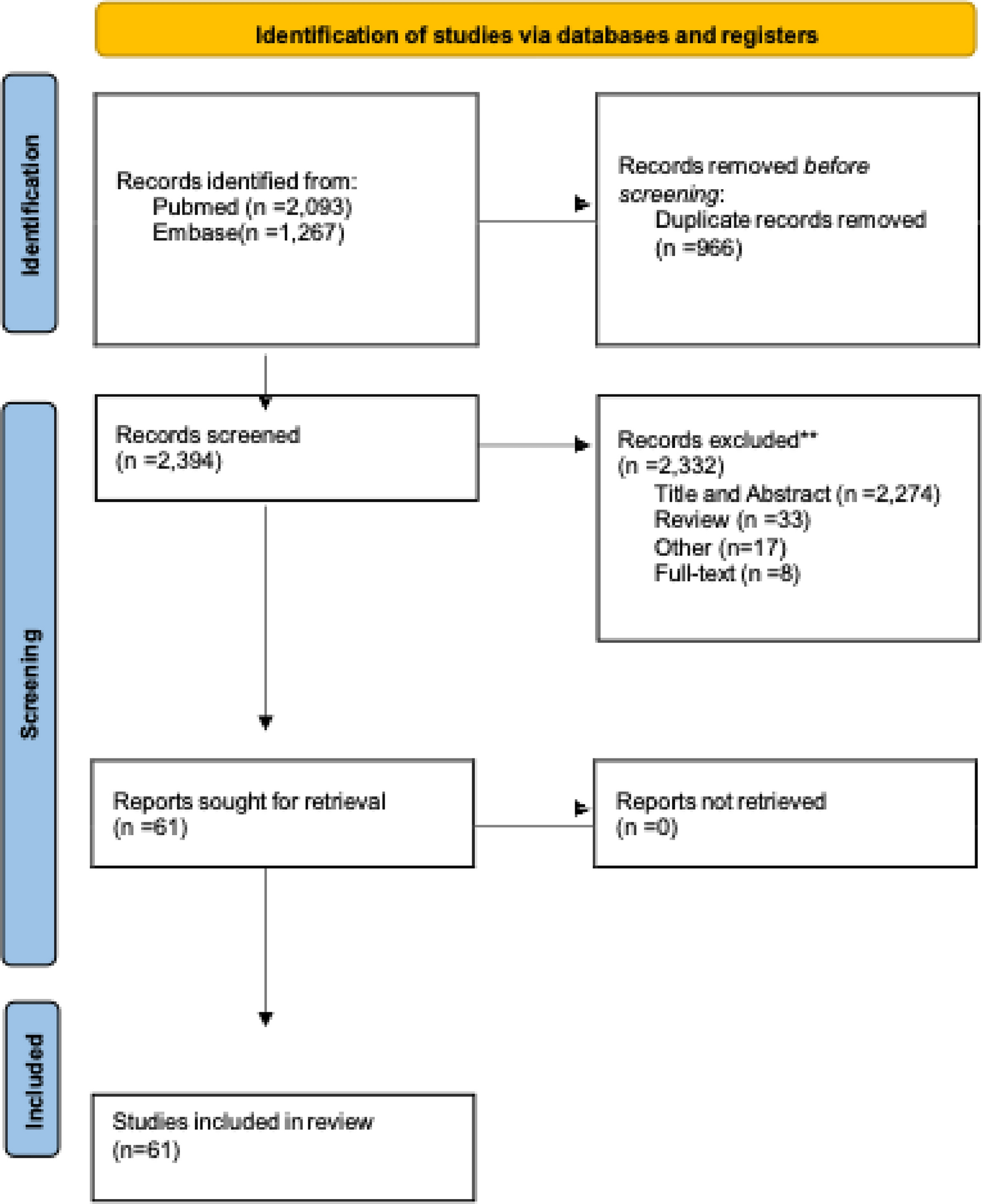
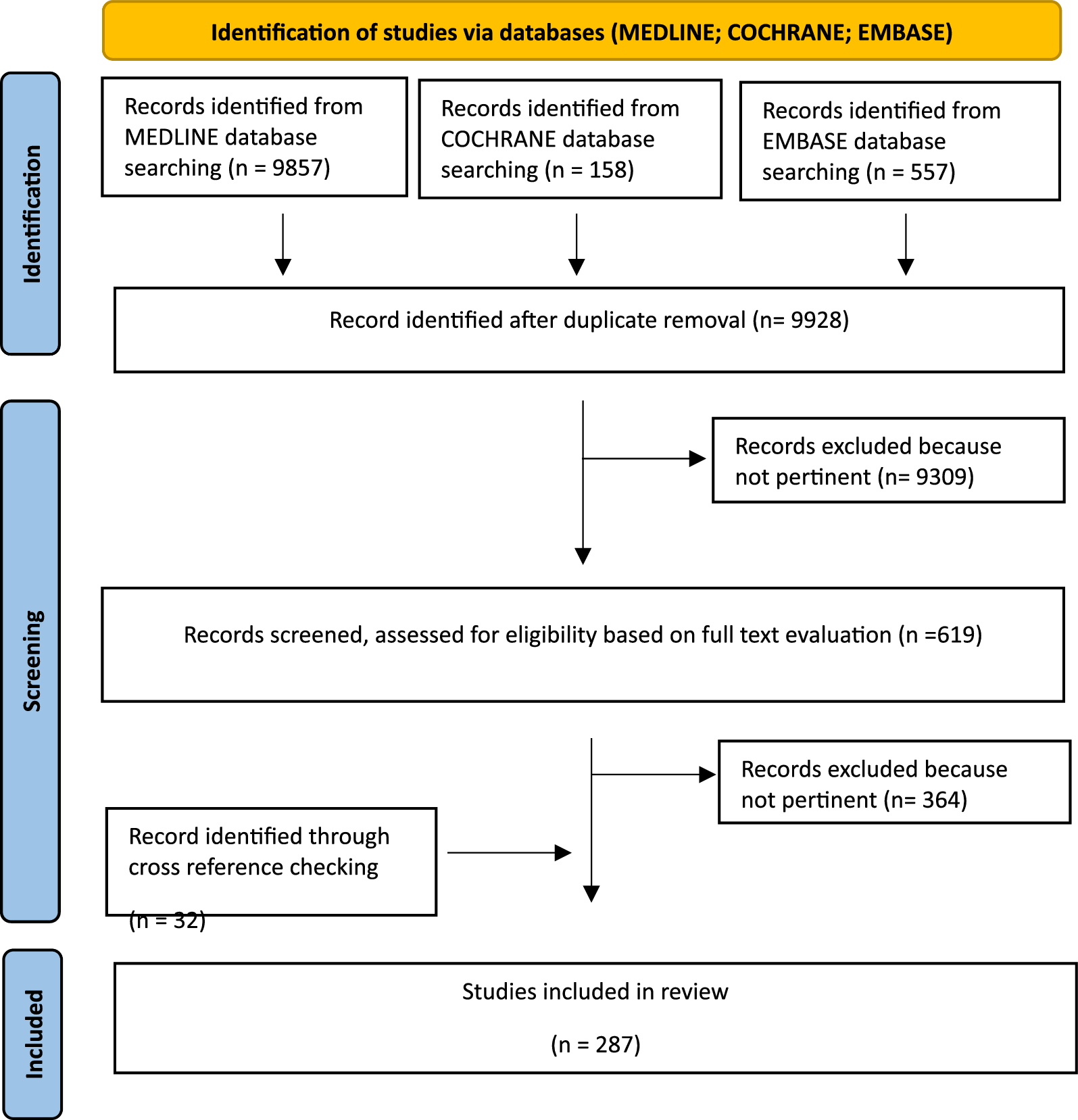


The initial search yielded 10.572 results (PubMed 9857, Cochrane 158, Embase 557). After removing duplicates, 9928 articles were screened for eligibility based on title and abstract, and 619 articles were retrieved for a full-text evaluation. After excluding 364 non-pertinent articles, a total of 287 studies were finally included in the review, including 32 articles identified through cross-reference checking (Fig. 1).
Fig. 1
Shows PRISMA flow chart of Review paper
Position statementsFollowing a comprehensive literature review and the summary of current scientific evidence of SSRF, for each of the focus question, the following position statements (PS) were created. For each PS, the supporting literature, the level of evidence, and the strength of the consensus are reported. The level of evidence (LoE) is classified according to the GRADE system (https://training.cochrane.org/introduction-grade). For each statement, the consensus was assessed through a web survey open to all members of the steering committee and panel of experts and to the members of the Board of Governors of the WSES. If a statement reached < 75% of agreement, it was rediscussed, modified, and resubmitted to the experts’ vote until a consensus was reached.
1.SSRF indications
PS 1.1SSRF should be considered in all flail chest (FC) patients (LoE IIa, Grade B).
PS 1.2SSRF should be considered in non-FC patients with rib fractures, in the presence of:
Multiple (≥ 3) ipsilateral severely displaced rib fractures (LoE IIb, Grade B);
Multiple (≥ 3) ipsilateral displaced, rib fractures in ribs 3–10 in combination with respiratory failure despite mechanical ventilation or weaning failure or at least two pulmonary derangements in non-ventilated patients despite loco-regional anesthesia and multimodal analgesia: (i) respiratory rate > 20 breaths per minute, (ii) incentive spirometry < 50% predicted, (iii) numeric pain score (NPS) > 5/10, and iv) poor cough (LoE IIb, Grade B)
A chest wall deformity that significantly affects lung function (i.e. implosion chest wall injuries, “Stoved-in Chest”) or that shows mechanical instability on palpation (LoE IIb, Grade B);
A flail segment, especially if antero-lateral and with some degree of displacement (LoE IIIa, Grade B);
Severe pain non-responsive to other treatments (LoE IV, Grade C);
PS 1.3SSRF is optimal in dedicated centers with a multidisciplinary team, developing and optimizing protocols addressing NOM and SSRF for rib fractures patients (LoE V, Grade D);
Flail chest (FC)A flail chest (FC) is a clinical finding, characterized by the paradoxical movement of a flail segment with respirations, whereas a flail segment is a radiographic finding, defined as a contiguous segment of 3 or more consecutive ribs fractured at 2 or more places. This distinction was recently defined and not universally known and adopted among all clinicians, in both the research and clinical practice and these has led to misunderstandings about optimal patient management [25, 26].
Trauma patients with FC have an increased risk of respiratory failure and mortality [27]. The treatment of FC has evolved over the past half-century, with early strategies using chest wall traction and external stabilization methods, later abandoned in favor of internal pneumatic splinting using positive pressure mechanical ventilation [28]. Several authors subsequentially reported excellent results of SSRF, that has been practiced sporadically for decades and almost exclusively in patients with flail chest [29]. Randomized clinical trials (RCT) comparing SSRF with non-operative management (NOM) [30,31,32] found lower incidence of tracheostomies, pneumonia, respiratory failure and shorter mechanical ventilation and intensive care unit (ICU) stay in FC patients undergoing SSRF. Furthermore, significantly less restrictive impairments of pulmonary function were reported in the operative groups at one [30] and two months of follow-up avoiding chest wall deformity [31]. Moreover, the RCT by Tanaka et al. [30], documented a lower total medical expense per patient treated operatively and a faster return to work. Persistent chest tightness, thoracic cage pain, and dyspnea on effort were significantly more frequent complaints in patients in the internal pneumatic stabilization group at twelve months of follow-up.
Despite the added cost of surgery, Bhatnagar et al. showed that SSRF remained the most cost-effective for FC patients. The reduction in pneumonia rates, ventilator days and hospital length of stay resulted in an overall reduction in cost and improved effectiveness compared with internal pneumatic stabilization [33].
The improvement in pulmonary function tests and lower thoracic deformity and pain were confirmed in FC patients undergoing SSRF in some prospective studies [34, 35] and in an RCT by Liu et al. [36], which demonstrated lower morbidity and decreased risk of acute respiratory distress syndrome (ARDS) respect to non-operative strategies. However, in the presence of concomitant severe pulmonary contusion (PC) a shorter mechanical ventilator time and ICU stay were not observed in the operative group. SSRF for FC appeared to be most beneficial in patients with anterolateral FC and respiratory failure without severe PC, in patients with PC and persistent chest wall instability or weaning failure and non-intubated patients with deteriorating pulmonary function [37].
Four metanalyses [38,39,40,41] have demonstrated benefits of SSRF in reducing the duration of mechanical ventilation, pneumonia/ tracheostomy rates, ICU stay and costs compared to NOM. Mortality rates and total hospital stay were also significantly lower in the surgical groups, besides other outcomes mentioned above, in some metanalysis, case–control and prospective cohort studies [42,43,44], confirming that SSRF in FC patients results in improved clinical outcomes and is a cost-effective intervention. The latest guidelines and consensus papers regarding surgical treatment of traumatic rib fractures state that SSRF should be performed in patients with FC [45,46,47,48,49].
Non-FC rib fracturesThe vast majority of patients with severe chest wall injuries do not have a FC. Accordingly, limiting SSRF to FC patients will address only the great minority of severe chest wall injuries. The number and displacement of fractures are recognized predictors of mortality and pulmonary complications, such as pneumonia, ARDS and need for tracheostomy in thoracic trauma patients, independent of the presence of FC [50,51,52,53]. Evidence regarding the effectiveness of SSRF in patients with some non-FC rib fractures has progressively emerged. However, definitions and injury classification are unclear and inconsistent between clinical trials. The heterogeneity of inclusion criteria and taxonomy of rib fractures, especially regarding the degree of displacement, makes it difficult to draw conclusions [25].
An interdisciplinary collaboration between the Chest Wall Injury Society (CWIS) and the American Society of Emergency Radiology (ASER) recently addressed chest wall injury nomenclature. Non-displaced ribs were defined as having ≥ 90% cross-sectional overlap, offset rib fractures < 90% cross-sectional overlap, and displaced rib fractures have no cross-sectional overlap. The term “cross-sectional overlap” is easy to understand and provides better correlation of the degree of displacement accounting for both the cortical and cancellous bone on axial and multiplanar reformats of the chest CT [26].
Considering the available evidence, which is presented below, we think that the following rib fracture displacement classification can further improve communication between health care providers and help to direct future research on chest wall injuries:
Non-displaced: > 90% cross-sectional overlap
Offset: 50–90% cross-sectional overlap,
Displaced: > 0 to < 50% cross-sectional overlap
Severely displaced: no cross-sectional overlap or overlapping ribs
In a recent retrospective analysis [54] and two prospective studies comparing SSRF to NOM in patients with non-FC chest wall injuries [55, 56], the authors concluded that rib fixation did not appear to provide benefits in short and long-term outcomes (QoL or pain up to 6 months). However, the only inclusion criteria in the first prospective cohort study was the presence of “three or more ipsilateral rib fractures”. No degree of displacement or baseline pulmonary physiologic derangements or pain were required for inclusion in the study and these variables were not even reported in the results. Regarding the second prospective study, approximately half of the patients enrolled had displaced fractures, and had a median of one fracture with an unreported degree of displacement. These studies underscore the importance of patient selection for SSRF.
Pieracci et al. included a wide variety of fracture patterns, with the most common being three or more severely displaced fracture (defined as bicortical displacement), in a 2-year prospective controlled clinical evaluation of chest trauma patients [57]. SSRF, as compared with the best medical management, was independently associated with a 76% decreased likelihood of respiratory failure and an 82% decreased likelihood of tracheostomy as well as 5-day decreased duration of mechanical ventilation and significantly improved spirometry readings among extubated patients. Additional inclusion criteria of the study were the presence of a flail segment, ≥ 30% volume loss of the affected hemithorax, or severe pain/respiratory failure despite optimal medical management.
An RCT by Wu et al. [58] including trauma patients with at least three displaced rib fractures (defined as frame fracture dislocation > 50%) confirmed the benefits of SSRF, compared to NOM, in decreasing acute chest pain, reducing the duration of mechanical ventilation, lowering the incidence of pneumonia, shortening the ICU and total hospital length of stay, also alleviating the forward chest wall discomfort.
In a recent multicenter prospective RCT, Denghan et al. [59], randomly assigned 207 patients with unstable chest wall injuries, defined by the presence of: ≥ 3 fractures with a severe displacement (defined as > 100%) or overriding (by minimum 15 mm each) or protrusion into lung parenchyma, to undergo operative or nonoperative management. Additionally, patients with a flail segment (with at least 3 of the rib fractures involved with some degree of displacement.), or ≥ 25% hemithorax volume loss were also considered as having unstable chest wall injuries and were included in the study. SSRF was associated with decreased mortality (0% vs. 6%; p = 0.01), and improvement in ventilator-free days and decreased length of hospitalization in the subgroup of patients who were undergoing mechanical ventilation at the time of randomization. However, only small benefits from surgical intervention were documented in non-ventilated patients, which constitute a much larger cohort of patients seen in trauma centers. Evidence regarding the benefits of surgical intervention in non–ventilated patients without FC were not described. The authors did not report the results of their analysis on meaningful outcomes in these patients such as pleural space complications, chronic pain and disability. Additionally, no mention was made about detail of the surgical approach and the time from injury to fixation. Of note, in the majority of patients, pelvic fixation plates were utilized for stabilization of fractured ribs, a surgical option that has been abandoned in SSRF.
However, Pieracci et al. [60], in a multicenter prospective clinical trial including non-FC, non-ventilator dependent trauma patients with ≥ 3 displaced rib fractures, found that SSRF, compared to NOM, was associated with lower pleural space complication rates, lower pain scores/respiratory disability and improved quality of life at two week follow up. The patients who were included had at least 3 ipsilateral, but not necessarily consecutive, displaced fractures of ribs 3–10 (displacement ≥ 50% of rib width measured on axial CT chest imaging) without flail segment (defined as ≥ 2 consecutive ribs each fractured in ≥ 2 places on CT chest). In addition, at least 2 of the following pulmonary derangements measured after initiation of loco-regional anesthesia were present: (i) respiratory rate > 20 breaths per minute, (ii) incentive spirometry < 50% predicted, (iii) numeric pain score (NPS) > 5/10, and (iv) poor cough. Therefore, these patients with persistent pain despite medical treatment and respiratory impairment should be considered for SSRF. The use of pain severity score as a criterion for fixation remains a matter of debate due to its subjectivity and variability from patient to patient [61], but rib fracture long-term morbidity is well documented in patients with chronic pain, deformity, respiratory compromise, reduced QoL for up to 2 years postinjury and associated poor return to work rate [14, 62].
Marasco et al. in a recent RCT [63] compared SSRF and NOM in non–ventilated trauma patients with at least 3 painful or displaced rib fractures. The authors were unable to document improvements in pain or QoL at 3 and 6 months after SSRF. However, return-to-work rates improved between 3 and 6 months, favoring the operative group. Other case series and retrospective studies have shown improvements in long term pain and QoL of patients who underwent SSRF [64,65,66,67].
In a prospective single center study involving 118 patients that had almost exclusively two or three rib fractures, Khandelwal et al. [68] stratified the management of all patients based on pain severity. Patients with mild to moderate pain received NOM, while patients with severe pain underwent SSRF. The result showed that SSRF reduced pain to a greater extent and shortened the time of disability and the time to return to work.
Several systematic reviews and meta-analyses have attempted to quantify the benefits of multiple rib fractures fixation compared to NOM. Most of these meta-analyses also examined a significant number of patients with flail injuries [69,70,71,72,73,74,75], but in many cases it was unclear whether it was a radiological or clinical flail, making results difficult to interpret. However, all meta-analyses found decreased pneumonia rates, reduced ICU length of stay, decreased duration of mechanical ventilation [69, 71,72,73,74,75], lower total hospital days [69, 71,72,73], decreased mortality [69,70,71, 73, 74], decreased tracheostomy rate [69,70,71,72,73,74], less chest wall deformity [69, 72] and less dyspnea [69] following SSRF.
A meta-analysis by Wijffels et al. [76] excluding studies in which the proportion of patients with FC or flail segment was > 50%, found a significant reduction in pneumonia rates, mortality, and hospital length of stay in patients who underwent SSRF compared to NOM, even without effects on the duration of mechanical ventilation and ICU stay.
A recent metanalysis included only studies focused on the management of patients with non-FC fracture patterns in the Asian population [77]. He et al. found that patients who underwent SSRF had a shorter duration of mechanical ventilation, ICU and hospital length of stay and lower risk of atelectasis and pneumonia with better pain scores at 4 weeks, although no clear mortality benefit was reported.
There are a number of retrospective and prospective observational studies that also support other indications for SSRF, including symptomatic non-union [78,79,80,81] and thoracotomy for other reasons such as retained hemothorax [82,
Comments (0)