Subjects and study design
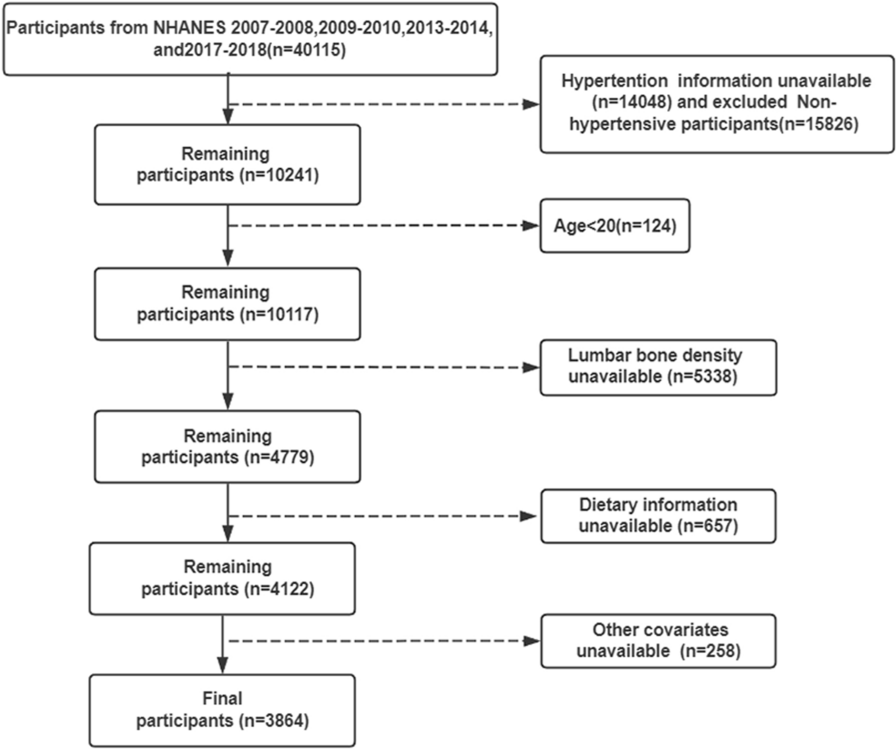
A total of 5829 subjects with metabolic syndrome were enrolled in a cohort study. All subjects were recruited from a single specialized healthcare center, Vilnius University Hospital Santaros Klinikos, as part of the LitHiR program. The LitHiR program aimed to recruit both women (aged 50–65 years old) and men (aged 40–55 years old) without a history of cardiovascular disease [16].
The exclusion criteria were as follows:
Proven (clinically evident) coronary heart disease (CHD), including myocardial infarction or unstable angina, angina on effort with positive stress test results, coronary pathology identified on coronaroangiography or multi-slice computed tomography angiography, coronary artery bypass grafting, or angioplasty, as well as acute coronary events in the past;
Proven cerebrovascular disease, comprising acute cerebrovascular events in the past or proven stenosis in the carotid arteries;
Proven peripheral artery disease, encompassing acute ischemic syndrome, proven chronic ischemia in limbs, and aortic aneurism;
End-stage oncological disease;
Any other end-stage somatic disease.
Subjects diagnosed with metabolic syndrome following the initial assessment were referred to Vilnius University Hospital Santaros Klinikos for further evaluation. Metabolic syndrome was diagnosed according to the revised National Cholesterol Education Program Adult Treatment Panel III (NCEP ATPIII) definition [17], wherein the presence of three or more of the following criteria established the diagnosis:
Waist circumference ≥ 102 cm for men, ≥ 88 cm for women;
Triglyceride level ≥ 1.7 mmol/l;
High-density lipoprotein cholesterol level < 1.03 mmol/l for men, < 1.29 mmol/l for women;
Blood pressure ≥ 130/85 mmHg or ongoing antihypertensive treatment for a subject with a history of arterial hypertension;
Fasting plasma glucose level ≥ 5.6 mmol/l.
The prospective longitudinal study was conducted in accordance with the principles of the Declaration of Helsinki, received approval from the Regional Ethics Committee (Permission No. 2019/3-1104-603) and the need to obtain informed patient consent was waived.
Clinical assessment
Before inclusion in the study, all subjects underwent physical examination, during which anthropometric data were recorded, including height in meters, weight in kilograms, waist circumference in centimeters, and body mass index (BMI), calculated as weight divided by the square of height. Cardiovascular risk factors such as smoking, familial cardiovascular disease, and arterial hypertension were assessed. Smoking was defined as smoking at least one cigarette per day, and familial CVD was considered if CV events had occurred among first-degree relatives (men ≤ 45 years, women ≤ 55 years old). Additionally, all subjects underwent a 12-lead electrocardiogram, with heart rate recorded, and blood pressure measurement. Blood pressure was measured, using an oscillometric semiautomatic device (Schiller Argus VCM) with a standard bladder (12–13 cm long and 35 cm wide), validated with a standardized mercury sphygmomanometer. Blood pressure was measured twice on the right arm after 5 min of rest, with the higher value being recorded. Mean arterial pressure was automatically calculated using the applanation tonometry system (SphygmoCor System) by obtaining the total area under the pressure curve and dividing this value by the duration of the time interval.
Additionally, a venous blood sample was collected after a 12-hour fast for the evaluation of total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglyceride levels. Glycated hemoglobin, fasting plasma glucose, and insulin levels were also assessed, along with plasma glucose and insulin levels after an oral glucose tolerance test.
The assessment of arterial markers
Arterial markers of subclinical atherosclerosis were assessed for all subjects using non-invasive means, which involved measuring endothelial function, arterial stiffness, wave reflection parameters, and wall parameters of the common carotid artery. Subjects were instructed to abstain from smoking and physical activity for at least 2 h before the examination. Vascular assessment was conducted after the subjects had rested for 10 min in a supine position.
Endothelial function was assessed using the endothelium-dependent flow-mediated dilatation (FMD) test, performed with a high-resolution ultrasound system equipped with a 12 MHz linear-array transducer and echo-tracking mode (Prosound α-10, Aloka, Japan) on the brachial artery. The diameter of the brachial artery was measured twice: first at rest and then after 5 min of ischemia introduced by inflating a pneumatic tourniquet placed on the forearm to 100 mmHg above the systolic blood pressure. Endothelium-dependent vasodilatation was automatically calculated as the maximum change in arterial diameter from the baseline during the first two minutes of the post-occlusive reactive hyperemia.
To evaluate arterial stiffness and wave reflection parameters the following tests were conducted:
Pulse wave velocity (PWV) and wave reflection were assessed using an applanation tonometry system (SphygmoCor, AtCor Medical, version 8.0, Sydney, Australia) with a high-fidelity micromanometer (Millar Instruments, Houston, Texas). This system was placed on the skin surface at the projection of the carotid and femoral arteries to obtain pulse pressure wave curves. Brachial blood pressure was recorded, and the direct distance between the common carotid artery and the femoral artery was measured. This data, together with the simultaneously recorded electrocardiogram, enabled the system to compute the main parameter of arterial stiffness, aortic (carotid–femoral) pulse-wave velocity (aPWV) [18, 19].
The ankle-brachial index (ABI) and cardio-ankle vascular index (CAVI) were measured using the VaSera VS-1000 (Fukuda Denshi Co. Ltd., Tokyo, Japan). After the subject had been stabilized in the supine position for 5 min, blood pressure at the posterior tibial and brachial arteries was measured. ABI was calculated as the ratio between systolic blood pressure measured at the ankle and systolic blood pressure measured in the arm. A value less than 0.9 was interpreted as indicating lower-limb arterial occlusion while the value greater than 1.3 was interpreted as indicative of lower-extremity arterial calcification and stiffness, with values in between interpreted as normal.
Four blood pressure cuffs were placed on the four extremities to evaluate the CAVI. Electrocardiography electrodes were attached to both arms, and a microphone was positioned on the sternum in the second intercostal space. After the subject had been stabilized in the supine position for 10 min, electrocardiography and phonocardiography were monitored. CAVI was calculated using Bramwell-Hill’s equation [20]: \(\:\text\text\text\text=\text\text\frac}\text}\text\text\left(\frac\text}\text}\right)\text\text\text}^+\text\), where ‘Ps’ represents systolic blood pressure; ‘Pd’ represents diastolic blood pressure; ‘ΔP’ represents the difference between systolic and diastolic blood pressure; ‘PWV’ represents the cardio-ankle pulse wave velocity; ‘ρ’ represents blood viscosity; and ‘a’ and ‘b’ are constants used for converting the CAVI value to a value obtained using the Hasegawa method.
Common carotid intima-media thickness (cIMT), cross-sectional carotid artery distensibility (both measured in µm), and the nondimensional index Quality Carotid Stiffness of the common carotid artery were assessed using high-resolution echo-tracking technology (Art. Lab, Esaote Europe B.V., Maastricht, the Netherlands). Measurements were taken 1 cm proximal to the carotid bifurcation along a 4 cm arterial segment. Quality Carotid Stiffness and cIMT were measured on both the right and left sides of the common carotid artery, and mean values of these measurements were used in the statistical analysis [21].
Follow-up and clinical outcomes
All the subjects were followed up for cardiovascular death for an average of 6.35 ± 2.99 years. Outcome data were retrieved from the Lithuanian National Death Registry. CV death was defined as death caused by myocardial infarction or stroke (including both ischemic and hemorrhagic strokes), or sudden cardiac death.
Statistical analysis
Statistical analysis was conducted using jamovi, and the R statistical computing environment (version 4.2.3; R Core Team 2023). If not indicated otherwise, continuous variables are presented as medians along with interquartile ranges, instead of mean values with standard deviations, to account for the large dataset lacking evidence of normal distribution, as well the presence of numerous outliers.
The Shapiro–Wilk test was employed to assess normality. Continuous variables were compared using the Wilcoxon rank-sum test, while categorical variables were compared using the χ2-test or Fisher’s exact test, as appropriate.
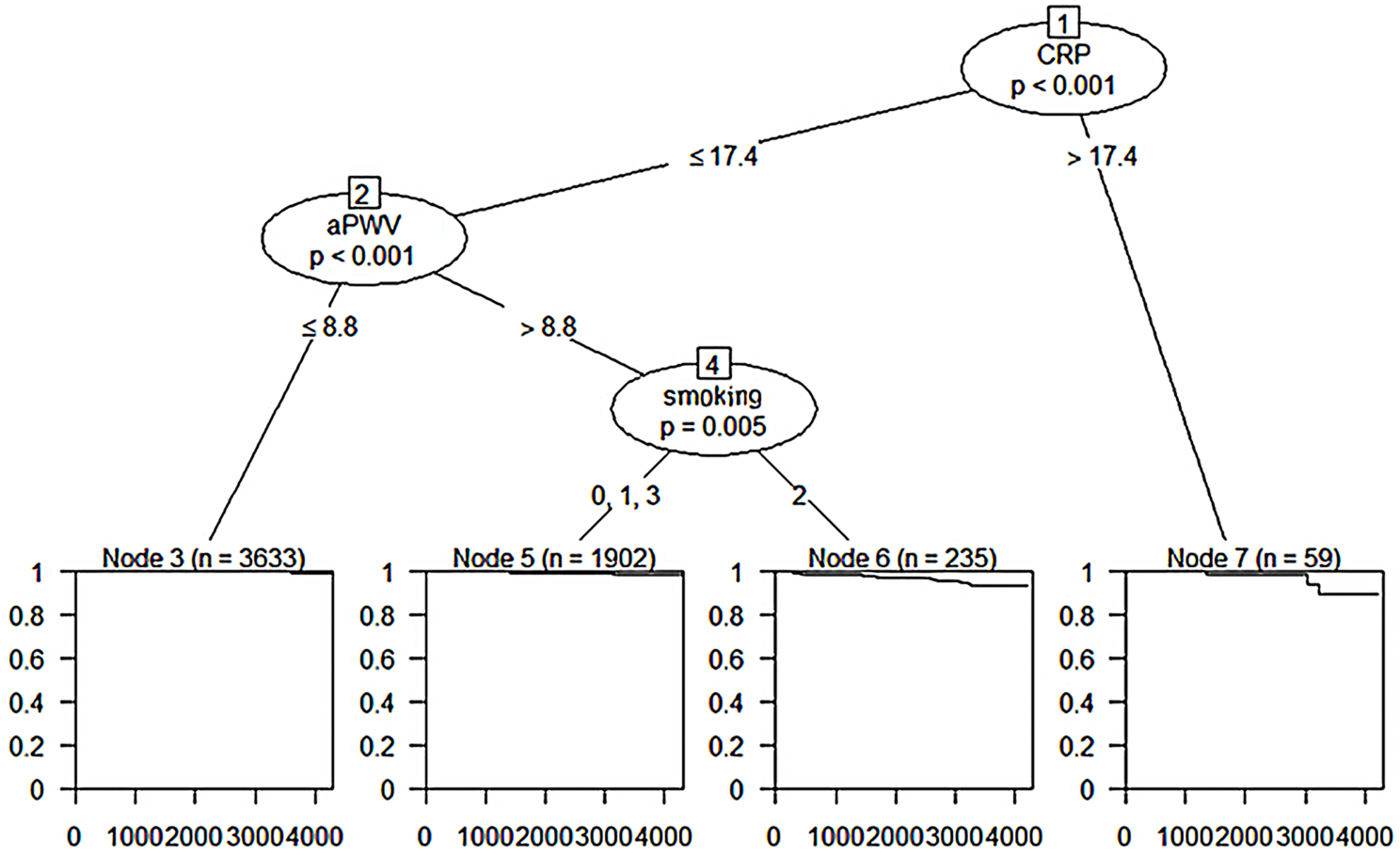
The Cox regression model was utilized to compute both unadjusted and adjusted relative risks for CV death during follow-up, estimated as the hazard ratio (HR) with the corresponding 95% confidence interval (CI). Schoenfeld’s residuals were employed to evaluate the proportional hazard assumption. The weighted predictive mean matching method was employed for imputing missing values. Furthermore, two-level survival trees were constructed to identify the main predictive variables. In order to identify sets of variables having the optimal predictive value, survival tree analysis utilizes recursive binary partitioning of a predefined covariate space. These variables are referred to as “nodes”. In order to distinguish the highest homogeneity of observations cut-off points for all “nodes” are estimated.
All p-values were 2-tailed, and the level of significance was set at 0.05.





Comments (0)