
Remember me


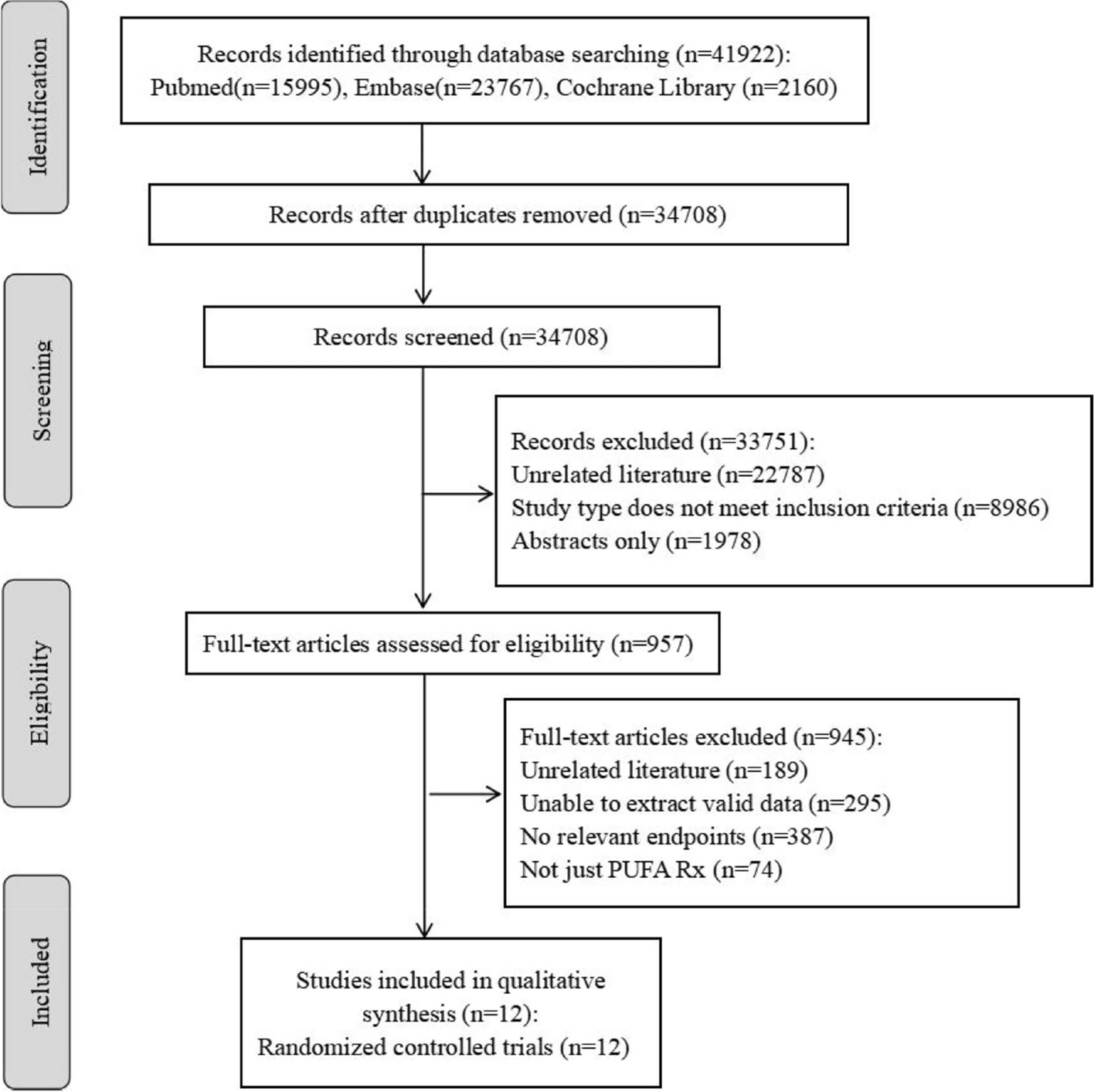

After reviewing 41,922 studies from the databases, 957 were selected for full-text review. Ultimately, 12 RCTs published between 2001 and 2019, encompassing 99,830 participants, were included in the final analysis [16,17,18,19,20,21,22,23,24,25,26,27] (Fig. 1). The mean age of the participants in the studies ranged from 59.4 to 74.0 years, and the follow-up period varied from 1 to 6.2 years. The intervention drugs were PUFA Rx capsules, with two of them being EPA-only [17, 21] and the remaining ones being EPA + DHA compounds [16, 18,19,20, 22,23,24,25,26,27]. Most of the controls were capsules filled with mineral oil or vegetable oil, one [21] was statin (the intervention was PUFA Rx + statin), and one was [22] no supplement. The daily dosage of PUFAs Rx was 1 capsule (1 g) in 8 studies and more than 1 g/d in other 4 studies. The population involved primary prevention in one study [23], secondary prevention with PUFAs Rx used for acute MI in 3 studies [20, 22, 26], and a mix of primary and secondary prevention in other studies [16,17,18,19, 21, 24, 25, 27]. The demographic characteristics of the included trials and participant information are presented in Table 1.
Fig. 1
Flow diagram of literature search and study selection
Table 1 Basic characteristics of the involved trialsThe majority of the studies presented high methodological quality, and all studies were double-blind. However, a few studies lacked reporting on crucial aspects such as random sequence generation, allocation concealment, and blinding of participants or outcome assessment. Two studies failed to blind the controls [21, 22]. The details are illustrated in Fig. 2.
Fig. 2
Risk of bias for eligible trials among 12 RCTs based on the cochrane risk of bias tool. A Risk of Bias Summary. B Risk of Bias Graph
Primary outcomesCardiovascular eventsEight studies reported cardiovascular events [16,17,18,19,20,21,22,23, 25], comprising 5,140 cardiovascular events among 75,929 participants. One study [16] defined cardiovascular events as cardiac arrest, MI, revascularization, stroke, abdominal aortic aneurysm surgery and peripheral vascular revascularization; two studies [21, 25] limited cardiovascular events to coronary events alone. The remaining five studies' definitions were roughly consistent, encompassing a composite of coronary heart disease (angina, myocardial infarction, coronary revascularization and coronary heart disease death) and other unanticipated cardiovascular events (heart failure, stroke, transient ischaemic accident and other circulatory problems).
Compared to the control group, PUFA Rx demonstrated a 12% reduction in the risk of cardiovascular events (RR, 0.88 [95% CI, 0.81–0.95]; P = 0.0007; I2 = 45%; tau2 = 0.00; Fig. 3; prediction interval shown in the supplementary Figure S1). Subgroup analyses (Table 2 and Supplementary Figure S8-11) showed a significant difference between PUFA Rx with EPA-only and those with EPA + DHA (P = 0.004). EPA-only reduced cardiovascular event risk by 21%, while EPA + DHA combined decreased it by 8% (EPA only: RR, 0.79 [95% CI, 0.73–0.85]; P < 0.00001; I2 = 0; tau2 = 0.00; EPA + DHA: RR, 0.92 [95% CI, 0.86–0.99]; P = 0.02; I2 = 0; tau2 = 0.00). Furthermore, long-term utilization of PUFA Rx (more than 3 years) exhibited a more pronounced effect among individuals with shorter duration of use (RR, 0.87 [95% CI, 0.80–0.95]; P = 0.001; I2 = 46%; tau2 = 0.00). The reduction in cardiovascular event risk was statistically significant for both primary and secondary prevention (primary: RR, 0.91 [95% CI, 0.83–1.00]; P = 0.04; I2 = 0; tau2 = 0.00; secondary: RR, 0.83 [95% CI, 0.74–0.94]; P = 0.003; I2 = 57%; tau2 = 0.01).
Fig. 3
Forest plot illustrating the results of the primary endpoints
Table 2 Subgroup analysis of main outcomesSecondary outcomesMACEsA total of 5,793 events occurred among 91,055 participants in eight RCTs [17, 18, 21,22,23,24,25,26]. In this meta-analysis, MACE outcomes (including fatal or nonfatal stroke, fatal or nonfatal myocardial infarction, and cardiovascular death) were extracted for each study. MACEs in one study [21] were defined as major coronary events, i.e., excluding cerebrovascular events (stroke), while another study [25] defined MACEs as all-cause mortality, coronary reinfarction and stroke.
There was no significant difference in PUFA Rx between groups regarding MACEs incidence (RR, 0.93 [95% CI, 0.83–1.03]; P = 0.17; I2 = 77%; tau2 = 0.02; Fig. 4; prediction interval shown in the supplementary Figure S2). Notably, Subgroup analyses (Table 2 and Supplementary Figure S12-14) revealed that EPA-only PUFA Rx reduced the risk of MACEs by 24% (RR, 0.76 [95% CI, 0.68–0.84]; P < 0.00001; I2 = 0; tau2 = 0.00; Table 2), while EPA + DHA showed no significant difference (RR, 0.98 [95% CI, 0.89–1.08]; P = 0.66; I2 = 58%; tau2 = 0.00; Fig. 4). No study evaluated MACEs using EPA + DHA at a dosage > 1 g/day, thus subgroup analysis was not conducted for dosage.
Fig. 4
Forest plot illustrating the results of the secondary endpoints
Cardiac deathTen studies with 4,051 deaths among 95,440 participants were included [16,17,18,19,20,21,22,23,24,25]. There was a 9% reduction in the risk of cardiac death (RR, 0.91 [95% CI, 0.84–0.99]; P = 0.02; I2 = 23%; tau2 = 0.00; Fig. 4; prediction interval shown in the supplementary Figure S3). In the subgroup analysis (Table 2 and Supplementary Figure S15-18), we found that long-term use of PUFA Rx (more than 3 years) may reduce the risk of cardiac death by 9% (RR, 0.91 [95% CI, 0.84–0.99]; P = 0.03; I2 = 32%; tau2 = 0.00), while short-term use of PUFA Rx (less than 3 years) may have no effect on cardiac death (RR, 1.00 [95% CI, 0.39–2.59]; P = 1; I2 = N/A). The secondary prevention population may experience a 20% reduction in cardiac death risk (RR, 0.80 [95% CI, 0.66–0.96]; P = 0.02; I2 = 9%; tau2 = 0.00; Table 2), while there was no significant difference in primary and mixed prevention populations (primary: RR, 0.96 [95% CI, 0.79–1.18]; P = 0.72; I2 = 0%; tau2 = 0.00; mixed: RR, 0.94 [95% CI, 0.88–1.00]; P = 0.06; I2 = 0%; tau2 = 0.00; Table 2).
All-cause mortalityAll twelve studies [16,17,18,19,20,21,22,23,24,25,26,27] provided data on all-cause mortality for 99,830 participants and 7,842 deaths for any reason. PUFA Rx was not associated with reduced all-cause death (RR, 0.97 [95% CI, 0.91–1.04]; P = 0.40; I2 = 45%; tau2 = 0.00; Fig. 4; prediction interval shown in the supplementary Figure S4). No significant differences were detected in any of the subgroup analyses (Table 2 and Supplementary Figure S19-22).
MINine RCTs with 2,716 fatal and nonfatal MI events among 94,877 participants were included [17,18,19,20,21,22,23,24,25]. PUFA Rx, compared to the control, was associated with a reduced MI risk (RR, 0.84 [95% CI, 0.73–0.96]; P = 0.009; I2 = 62%; tau2 = 0.02; Fig. 4; prediction interval shown in the supplementary Figure S5). In the subgroup analysis (Table 2 and Supplementary Figure S23-26), EPA alone reduced the MI risk by 28% (RR, 0.72 [95% CI, 0.62–0.82]; P < 0.00001; I2 = 0; tau2 = 0.00), while no significant difference was detected for EPA + DHA (RR, 0.88 [95% CI, 0.76–1.02]; P < 0.10; I2 = 58%; tau2 = 0.02). The reduction in MI risk was 18% when taking PUFA Rx for more than 3 years (RR, 0.82 [95% CI, 0.72–0.94]; P = 0.0008; I2 = 63%; tau2 = 0.02). However, similar results were not found in duration less than 3 years (RR, 1.42 [95% CI, 0.70–2.86]; P = 0.33; I2 = N/A). The primary prevention population benefited from PUFA Rx, but the effect was not seen in the mixed prevention or secondary prevention groups (primary: RR, 0.74 [95% CI, 0.61–0.89]; P = 0.002; I2 = 0; mix: RR, 0.85 [95% CI, 0.71–1.02]; P = 0.08; I2 = 69%; secondary: RR, 0.83 [95% CI, 0.65–1.06]; P = 0.13; I2 = 25%).
StrokeEight studies [17,18,19, 21,22,23,24,25] were included, reporting 2,044 stroke events among 94,577 participants. PUFA Rx showed no effect on stroke prevention (RR, 1.03 [95% CI, 0.91–1.16]; P = 0.68; I2 = 45; tau2 = 0.01; Fig. 4; prediction interval shown in the supplementary Figure S6). Similar results were observed in the subgroup analyses (Table 2).
Revascularization
Comments (0)