Proteus mirabilis is a Gram-negative bacterium that is notorious for its ability to swarm firmly across surfaces in a striking bull’s eye pattern. Clinically, it exhibits an extraordinary lifestyle as uropathogen invading human urinary tracts. P. mirabilis was the 2nd most predominant uropathogen (5.2%) in the urine of male patients using indwelling catheters [36]. It is considered a model microorganism for urease-producing pathogens forming crystalline biofilms on indwelling urinary catheters, often leading to poly-microbial infection. Recent studies have illustrated how P. mirabilis causes all of these diseases. Especially, the discovery that this bacterium forms huge clusters in the bladder lumen forming stones, bladder tumors and several diseases mentioned some of them in our study. These clusters, and other steps of infection, require several virulence factors like urease, MR/P fimbriae, and hemolysins. To the best of our knowledge, this is the first study that investigates the virulence factors, and antimicrobial resistance and tries to evaluate the different molecular typing methods in the discrimination of P. mirabilis. In this study, 60 P. mirabilis were identified with incidence of 20%. In this study; The most prevalent diagnosis of isolated samples is Renal Stone cases as it represented 16.70% followed by Hypospadias cases (13.30%). In [37] study; 50% percent of urolithiasis cases are recurrent illnesses, leading to the loss of kidney if not properly treated. Several uropathogens are associated with the formation of bacteria-induced urinary stones but P. mirabilis is the most commonly caused (70%) among the tested uropathogens; as only P. mirabilis produced crystallization within the epithelial cells due to the increased number of intracellular bacteria and their urease activity. In Hungary; a study by [38], proved that the correlation between the existence of significant risk factors, and underlying illnesses (age, catheterization, and inpatient/outpatient status) with Proteus urinary tract infections could not be evaluated. The high-rate level of bacteriuria in elderly patients is considered an important role during isolation of Proteus.
Our isolates showed high resistance to nitrofurantoin (98.3%) and trimethoprim/ sulfamethoxazole (81.7%). They show moderate levels of resistance to ofloxacin, ciprofloxacin, amoxicillin/ clavulanic acid, cefotaxime and ceftazidime (60.0%, 58.3%, 45.0%, 41.7% and 40.0% respectively). A Low level of resistance was observed with amikacin, imipenem, piperacillin/ tazobactam and ertapenem (8.3%, 11.7%, 11.7% and 13.3% respectively). Finally; 73.33% of isolates were MDR. There is a statistically significant relation between the age of patients (15–65 years) and resistance to ofloxacin (P-value = 0.024). it was found that cefotaxime, ciprofloxacin, ofloxacin and amoxicillin/ clavulanic acid were significantly related to MDR with P-value < 0.001. Also, ceftazidime and trimethoprim/ sulfamethoxazole were significantly associated with MDR (P-value = 0.001) [39]. Reported similar results where 55.6% were MDR. MDR P. mirabilis isolates were associated significantly (P < 0.001) with resistance to penicillins (amoxicillin/clavulanic acid and piperacillin), cephalosporins (cefuroxime, ceftriaxone and ceftazidime), gentamicin, ciprofloxacin and trimethoprim/ sulfamethoxazole. These results are in agreement with the results obtained by [40]; showing that the highest resistance rate was found to trimethoprim/ sulfamethoxazole combination. A study performed by [36] showed variable resistance rates for ampicillin and amoxicillin (40%), ticarcillin (42%), gentamicin (18%), nalidixic acid (26%), norfloxacin (22%), ciprofloxacin (21%), trimethoprim/ sulfamethoxazole (32%), and fosfomycin (19%) [36].
In our study; the antibiotic resistance patterns of the tested isolates were evaluated. The most prominent antibiotype was A13 representing 16.67% of isolates with MAR index = 0.36. Followed by A5 antibiotype pattern (15%) with MAR index = 0.64. In addition, several antibiotype (A1-A10) had MAR index > 0.5. Calculation of MAR index is useful for a proper treatment of UTI patients and limits the use of resistant antibiotics so preventing furthermore development of bacterial drug resistance. Similar results were reported by [21]. The MAR index is a good risk assessment tool and the value of the MAR index = 0.2 has been applied to differentiate low and highly risk regions where antibiotics are overused [41, 42]. This analysis gives a good idea of the number of bacteria showing antibiotic resistance in the zone of the exposure study.
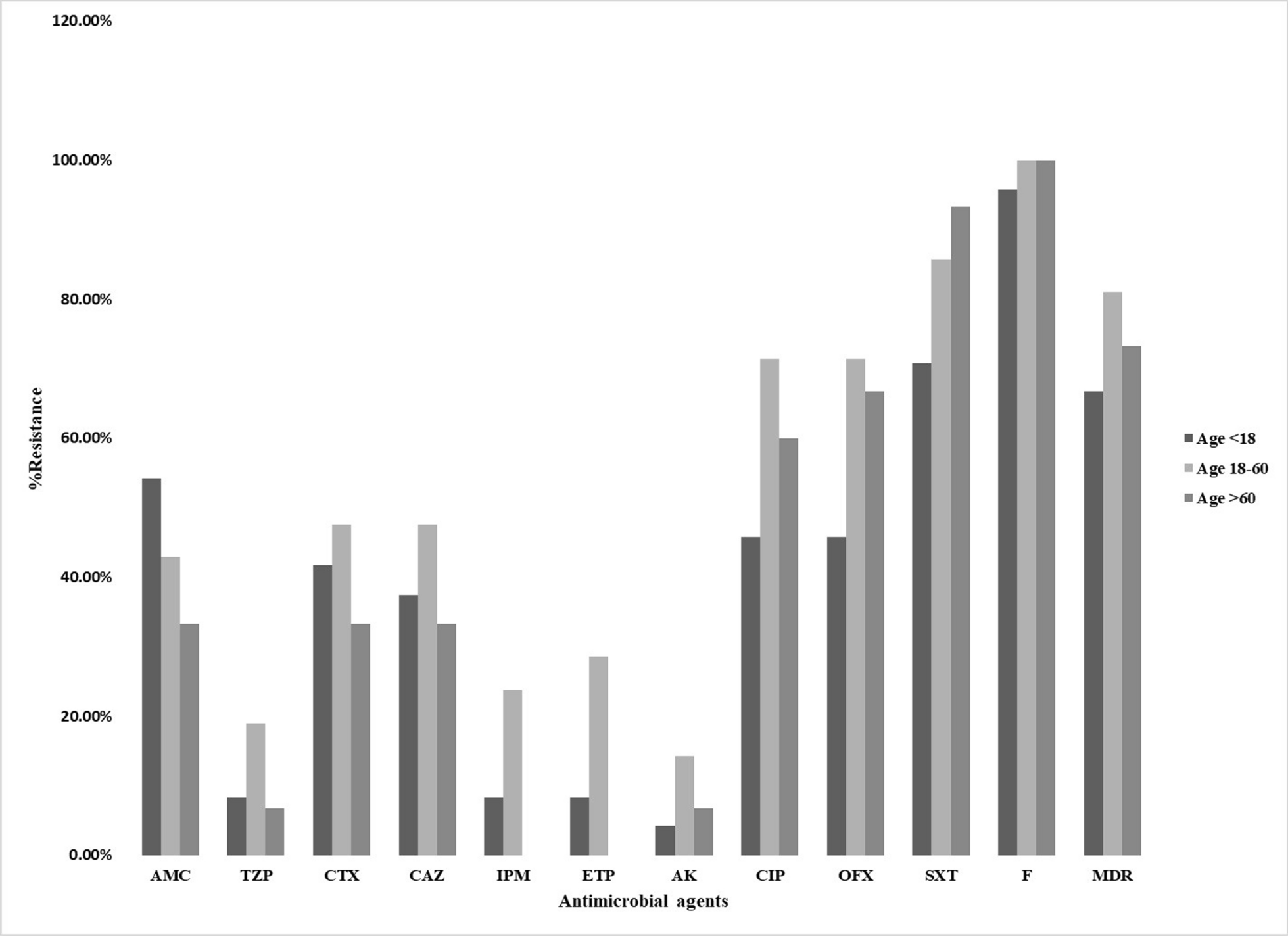
The distribution of tested antibiotics according to the age classes was studied. The elder age (3rd gp) comprised the majority of isolates resistant to nitrofurantoin and trimethoprim/ sulfamethoxazole. Moreover, it was associated with absence of resistance to imipenem and ertapenem (P-value = 0.017 and < 0.001 respectively). The median age (2nd gp) contained most of the isolates resistant to ofloxacin, ciprofloxacin, cefotaxime, ceftazidime, amikacin, piperacillin/tazobactam, imipenem and ertapenem as compared to the other two groups. The children (1st gp) contained isolates resistant to all used antimicrobials but to a lesser extent than the 2nd and 3rd groups except for amoxicillin/ clavulanic acid. [43] had reported similar results that the distribution of antimicrobial resistance between age groups was not statistically significant.
In our study; biofilm formation of isolates was achieved in 96.67% except 2 isolates (3.33%) (non-biofilm-producer). Twenty-one (35%) isolates were strong biofilm-producer, 19 (31.67%) isolates were moderate biofilm-producer and 18 (30%) isolates were weak biofilm-producer. That may be attributed to the fast growth of P. mirabilis that provides a high yield of biofilm that is vital in the host invasion [44]. [43] stated that all tested P. mirabilis isolates were biofilm-producers with 71.8% strong, 21.8% moderate and 6.4% weak biofilm-producers. [40] showed that isolates formed biofilms with very strong intensity, strong intensity, and moderate intensity (73.2%, 25.7% and 1.1% respectively. We found that biofilm was associated significantly with MDR (P-value = 0.017); where 36.4% of either strong and weak biofilm-producers and 27.3% of moderate biofilm-producers were MDR while non-biofilm-producers were NMDR. [44] reported that stronger biofilm-producers were also MDR P. mirabilis.
In this study, all of the tested isolates produced urease, protease and β hemolysins. Similar results were reported by [43]. Weak biofilm-producers were mainly in age groups 1–40 years old [43]. Similar to our results, [45] showed that all P. mirabilis isolates generated strong production of urease and β-hemolytic action. Al- Mayahi showed that 89.5% were hemolysin producers and 100% were positive urease producers [1].
Regarding the detection of virulence genes by PCR, zapA and ureC recorded the highest percentage of the tested virulence genes as they were harbored by all isolates (100%), followed by rsbA (95%), ureA & flaA (93%), hpmA (91.7%) and mrpA (73.3%). It was found that hpmA was significantly related to strong biofilm-producers with P-value < 0.001. the mannose-resistant Proteus-like adhesion (mrpA), P. mirabilis fimbriae (pmfA) and uroepithelial cell adhesion (uca play a crucial role in the catheter-associated biofilm formation, and the bladder and kidney colonization, respectively. zapA, hpmA, hpmB and ureC are engaged in the immune system evasion and/or iron acquisition, with zapA also involved in the swarmer cell differentiation and swarming behavior [44]. Sun et al. 2020 study showed similar results as biofilm formation was significantly related to the expression of atfA, ureC, pmfA, zapA, rsmA, mrpA, and hmpA with P-value < 0.05 [46].In addition, it reported that 92.05% of the P. mirabilis isolates were biofilm-producers and 38.27%, 48.15%, 13.58%, and 7.95% were strong, moderate, weak and non-biofilm-producers respectively. A study conducted in Brazil showed that all isolates were positive for (atfA, ptA, pmfA, ireA, zapA, mrpA, and hpmA) virulence genes [40]. Ali and Yousef, 2015 reported that zapA, hpmA and ureC were represented by 100% of isolates while ureA and flaA were found in 96.66% and 86.66% of isolates, respectively [30]. Another study showed that mrpA and rsbA were found in 35%, and 53% of isolates; respectively [47].
All P. mirabilis isolates were distributed into nine different virulence gene patterns. The most abundant patterns were V1 and V2 in 38 and 13 isolates respectively.
Molecular epidemiology stresses the role of environmental and genetic aspects that affect at molecular levels the disease process. It results in the determination of disease etiology, penetrance and distribution pattern in families and population. It investigates the molecular mechanisms and specific genes involved in disease risk, which aids in understanding disease pathogenesis. Molecular epidemiology gives a new way to better explain the disease processes and the recommendations needed for disease prevention and care. Molecular epidemiology should not be regarded as just another method or tool, but as an established control in epidemiology that can progress our knowledge about these diseases in ways that were impossible in the past [48].
Various techniques have been used in molecular epidemiology such as restriction endonucleases of genomic and plasmid DNA, southern hybridization, pulsed gel electrophoresis (PFGE), PCR-based approaches for plasmid and chromosomal profiling, microarray, and the most recent revolution, whole genome sequencing. In our study various molecular PCR-based typing techniques, such as RAPD, ISSR, ERIC-PCR, BOX-PCR and rep-PCR for P. mirabilis have been developed used. Various approaches have been utilized to characterize Proteus mirabilis. An important aspect is how a single method or a combination of methods can offer insights into parameters such as discriminatory index (DI), typeability, and ISD of the isolates. Comparing these methods enables researchers to select the most appropriate technique [15, 34, 49].
RAPD detects genetic variation by randomly amplifying segments of target DNA with a short oligonucleotide random sequence [15, 50]. In this study, two primers of RAPD have been used for the characterization of 60 P. mirabilis isolates. The two primers gave low typeability% (46.67% and 48.33%) and moderate ISD% (46.67% and 43.33%). In addition, they gave total bands of 9 and 6 bands with %MB equal 66.7% and PB% equal to 33.3%. when investigating the discrimination index, they showed low SID (0.72 and 0.735) below the acceptable level (0.95). OPZ19 classified the isolates into 28 clusters at 70, 80 and 80% cutoff, while OPX13 classified them into 20 clusters at 70% cutoff. In contrary [14], showed that RAPD markers had high discrimination index such as OPA19 (SID 0.847), and OPX13 (SID 0.921). Regarding that Three primers used (OPA11, OPX13 and OPZ8) provided a high level of discrimination among all P. mirabilis isolates. The effectiveness of RAPD markers for Proteus fingerprinting has been reported previously [51]. The relatively low reproducibility of RAPD typing limited its application to large-scale in laboratory studies.
Four intergenic single sequence repeats (ISSR) primers were used in this study. The best marker used was ISSR 2 where its typeability was 90%, ISD% was 68.33 and gave 38 clusters at 90% cutoff. Its MP% and PM% were equal to 50% with EMR = 1.5. The SID was high (0.983) with the highest number of patterns (57). The other primers were different in efficiency. ISSR1 was the best in typeability (85%) and SID (0.955). While ISSR6 was best at PM% (60%), ISD% (60%), SID (0.934), gave 36 clusters at 90% cutoff with 36 pattern and EMR = 1.8. ISSR 3 was the best marker showing the similarity between isolates as its ISD% (23.33), typeability (55%), number of clusters at 90% cutoff was 14 and its SID was 0.776. A study conducted by Michelim et al. showed ISSR primers gave a higher number of bands with PM% = 77.5%. In contrast to our result, the best marker was ISSR 6 as its SID was 1 followed by ISSR 1 and ISSR 2. ISSR 3 was the last one in discrimination between isolates as its SID was 0.458 [14].
ERIC-PCR typing method gave the highest efficiency in all aspects used as typeability (90 and 98.33%), ISD% (85 and 95%), number of clusters at 90% cutoff (51 and 57), PM% (77.77 and 66.67%), EMR (5.4 and 5.3), and SID (0.989 and 0.999). So, it was the best method used for the discrimination of isolates. ERIC-PCR gave PM% equal 90% and SID = 0.97 in a study of [14].The study of [52] showed that ERIC-PCR classified 98 E. coli isolates into six clusters proving that ERIC-PCR had high discriminatory power in genotyping strains. [53] reported that ERIC-PCR completely typed the 60 P. mirabilis isolates with high reproducibility. In addition, ERIC-PCR was reported as the best method for discrimination of P. aeruginosa isolates as compared to other PCR-based typing methods[15].
In this study, Box-PCR gave 70% for typeability, 63.3% for ISD%, 55. 56% for PM%, 0.911 for SID and 38 clusters at 90% cutoff. ERIC-PCR and BOX markers allowed separate the 29 Proteus isolates into several groups [14]. BOX-PCR and ERIC-PCR gave highly comparable efficiency in evaluating the genetic relatedness of 29 pathogenic Leptospira strains representing higher discriminatory index using ERIC-PCR 0.826 than BOX-PCR 0.809 [54].
REP-PCR in this study gave high typeability % (88.3 and 98.3%), PM% (57.14 and 60%) and SID (0.985 and 0.84). Although REP-PCR 21R has a high percent of typeability (98.33%) similar to the typeability percent of ERIC2 but has the lowest ISD (25%) value compared by different typing methods as ERIC and REP-PCR. So, the Index of Strain Diversity percentage gave more accurate results for the comparison of different typing methods. Twenty-nine P. mirabilis, showed that all 29 P. mirabilis isolates used were separated in various groups by using BOX-PCR and ERIC-PCR. This study shows resemble results with all primers used except for REP-PCR1R and 2I primers where they showed low discriminatory power (SID = 0.621).
By comparing the five different PCR-based typing method, ERIC was the best typing method in all of the studied parameters followed by REP-PCR, BOX-PCR, ISSR then at last RAPD-PCR which gave lower results than other methods. [14] reported that RAPD, ERIC-PCR and BOX-PCR markers with a high discriminatory power for typing clinical P. mirabilis isolates. ERIC-PCR is a cheap, easy-to-be-done, reliable and rapid method besides its high discrimination ability [15].
The probability that pairs of isolates assigned to the same type by one typing method are also typed as identical by the other is indicative of the congruence between typing methods. The congruence obtained by Rand’s coefficient indicated that ISSR2 was best predicted by ERICIR, ISSR1, ISSR2, ISSR6 and ERIC 1R were best predicted by ERIC 2 and ISSR2, ERIC1R and ERIC2 were best predicted REP-PCR 1R. the evaluation of the congruence using Wallace coefficient revealed that REP-PCR 21R and ERIC1R, OPZ19, ISSR2, ISSR6, REP-PCR1R, REP-PCR21R and ERIC2 showed moderate congruence (0.579 and o.5, respectively). While a complete congruence between ISSR3 and ERIC2 was found (W = 1). No or poor congruence occurred with the other typing primers signifying that they clustered the isolates in different methods.
In conclusion; we evaluated the antibiotic resistance, the virulence factors, biofilm production and the molecular typing methods for the differentiation of P. mirabilis isolates. The phenotypic methods used couldn’t discriminate between isolates. The best discrimination was achieved by PCR-based typing methods (ERIC-PCR, BOX-PCR, REP-PCR, RAPD and ISSR). ERIC-PCR was the best method that differentiated P. mirabilis isolates followed by REP-PCR. The other methods gave medium to high discriminatory efficiency in P. mirabilis. In addition, by evaluating the congruence between typing methods, ERIC-PCR was the best method giving high values for Rands and Wallace coefficients with other typing methods.
Thus; the ERIC-PCR method is recommended for use in future epidemiological studies of clinical isolates from various microorganisms isolated from infectious diseases.







Comments (0)