
Remember me

PneumoCAP is a prospective observational study conducted between 1st November 2017 and 31st December 2019, which was carried out through a network of 277 French general practitioners (GP). Investigators were selected for their ability to screen and enroll patients newly diagnosed with a CAP suspicion. CAP was clinically suspected and all patients had to fulfilled the following criteria: age ≥18 years, presence of at least one general sign of infection (fever > 38.5°C measured by the patient or GP, heart rate > 100/min, respiratory rate > 20/min, global impression of severity (global impression of the general practitioner regarding the severity of the patient’s health condition, quoted yes or no)18, muscle aches—fatigue or chills and at least one sign of lower respiratory tract infection (cough, unilateral chest pain, purulent or non-purulent sputum, auscultatory abnormalities compatible with CAP)17.
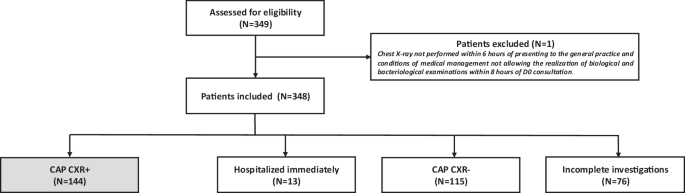
Study proceduresAccording to French guidelines1, investigators performed a CXR to all patients with CAP suspicion, as part of standard of care. After the CXR was performed, the investigators proposed to the patient to participate in the PneumoCAP study. For patients for whom it was not possible to perform a CXR as part of routine care (immediate hospitalization, or CXR not accessible), they were also proposed to participate in the study. Patients were included if they agreed to participate and signed the informed consent form.
For patients with a positive CXR, i.e. CXR compatible with a CAP according to local radiologist interpretation, clinical chemistry and microbiological tests were performed. Laboratory and microbiological samples were collected within 8 h after enrollment in local medical analysis laboratory.
For patients with negative CXR, i.e. CXR not compatible with a CAP according to local radiologist interpretation, clinical chemistry and microbiological tests were not ordered.
For patients requiring immediate hospitalization, neither the CXR nor the clinical chemistry and microbiological tests were ordered by the investigating GP.
For patients for whom all study procedures could not be completed, i.e. who did not wish to participate in the full study or for whom study procedures could not be respected (named “incomplete investigations”), the only data collected were limited to gender, age and the CRB65 score. (Fig. 4).
Fig. 4: PneumoCAP study procedures.
D0 Day 0 (date of inclusion), CAP community acquired pneumonia, eCRF online case report form.
Data collectionPatient’s demographic and clinical characteristics, medical history, information on medical conditions increasing risk for pneumococcal disease, pneumococcal vaccination status (PCV13 and/or PPV23) and influenza vaccination status according to medical record or declared by the patient, symptoms on inclusion, clinical examination data, were collected on day 0, by the investigating GP after interview and examination. All data were collected on an eCRF from day 0 until day 28 for all patients included, and up to day 90 for patients who were admitted to the hospital after enrollment.
Clinical chemistry tests included blood count, C-reactive protein (CRP), and procalcitonin (PCT) dosages were collected and performed in local medical laboratory. Microbiological testing included blood cultures, oropharyngeal swabs for multiplex real-time PCR for respiratory pathogens (Chlamydia pneumoniae, Legionella pneumophila, Mycoplasma pneumoniae, coronavirus 229E, NL63, OC43, HKU1, human metapneumovirus (hMPV), influenza A and B, parainfluenza viruses 1, 2, 3, and 4, respiratory syncytial virus (RSV), rhinovirus, enterovirus, adenovirus, bocavirus, R-GENE©, Biomerieux) and sputum Gram stain microscopy (with induced expectoration when possible). Sputum Gram stain microscopy and multiplex PCR were collected in local medical laboratory, multiplex PCR were shipped to be then performed in the same central laboratory in France. Urine sample for per-protocol testing was collected in local medical laboratory then frozen and shipped to the same central laboratory in France, then send to USA to be tested by pneumococcal urinary antigen test (PUAT) BinaxNOW S. pneumoniae® (Abbott Diagnostics), UAD serotype-specific multiplex urinary antigen detection test, UAD1, and UAD2 at Pfizer’s Vaccines Research and Development Laboratory (Pearl River, NY), identifying 1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F 23F serotypes for UAD1 and 2, 8, 9N, 10A, 11A, 12F, 15B/C, 17F, 20, 22F and 33F for UAD 222,23,24,25.
ObjectivesThe main objective was to estimate the percentage of CAP associated with SP among radiologically confirmed CAP (CAP CXR+) in outpatients in general practice. The first secondary objective was to describe the characteristics of pneumococcal CAP and non-pneumococcal CAP. The second secondary objective was to describe microbiological characteristics of patients treated in general practice for a radiologically confirmed CAP.
Case definition of “pneumococcal CAP” was as follows: a patient with CAP CXR + and at least one positive SP microbiological test (blood culture, sputum culture, PUAT [BinaxNow®], UAD1/UAD2 [Pfizer Inc®]).
Case definition of “non-pneumococcal CAP” was as follows: a patient with CAP CXR + for whom all four SP microbiological tests mentioned above were negative for SP.
Case definition of “undetermined CAP” was: a patient with CAP CXR + for whom none SP microbiological test was positive for SP and not all four pneumococcal tests were performed.
Data analysisPatient characteristics were reported by groups (radiologically-confirmed CAP, pneumococcal CAP, non-pneumococcal CAP, undetermined CAP), using frequency and percentage for categorical variables, and median and inter-quartile range values for continuous variables.
The percentage of pneumococcal CAP amongst radiologically confirmed CAP and its 95% confidence interval was estimated using the binomial distribution.
EthicsThe study was conducted as a collaboration between Pfizer and the French National Academic Council of General Practice (CNGE conseil). CNGE conseil was the study sponsor. The French health authorities (The French National Agency for Medicines and Health Products, ANSM) approved the study protocol and patient informed consent procedures. All enrolled patients provided written informed consent for inclusion. The protocol was registered in the clinicaltrial.gov website under the PNEUMOCAP acronym (NCT03322670). The Ethics Committee (Comité de Protection des Personnes, Ile de France II. Paris N° 2016-A01537-44) approved the study protocol.
Reporting summaryFurther information on research design is available in the Nature Research Reporting Summary linked to this article.
Comments (0)