The SHARE is a multi-disciplinary panel study of individuals aged 50 and older [19]. Wave 8 of SHARE, conducted in 2019 and 2020, includes device-based measurement of various activities for a subsample of respondents across ten countries [20]. Participants were instructed to wear an Axivity AX3 (Axivity, Newcastle upon Tyne, UK) tri-axial accelerometer on the thigh for eight consecutive days to monitor their everyday activities. The devices were set to a sampling frequency of 50 Hz (range ± 8 g). SHARE release 9.0.0 provides aggregate measures of accelerometer data, processed using ActiPASS version 1.61 beta [21], a software that classifies postures and activities based on thigh-worn accelerometers. ActiPASS metrics in the SHARE dataset include the time spent in various activities per day, categorized as sleep, sedentary, LPA, and MVPA. Sedentary activities are defined as sitting and lying down. LPA includes standing, moving, slow walking (cadence < 100 steps/min), and other non-periodic or periodic movements with a cadence < 100 steps/min. MVPA was defined as walking with a cadence ≥ 100 steps/min, running, cycling, stair climbing, and other periodic movements with a cadence ≥ 100 steps/min. Also, the number of steps per day was detected by ActiPASS. The time spent in intensity categories and the number of steps per day were averaged over all observation days. The ActiPASS algorithm for recognition of activities [22, 23] and steps [24] has previously been validated. Physical activity was categorized based on meeting specific recommendations. These included achieving at least 150 min of MVPA per week spending on average no more than eight hours per day in sedentary activities, and obtaining on average seven hours of sleep per night.
HGS was measured using a hand-held dynamometer (Smedley, S Dynamometer, TTM, Tokyo, 100 kg). Medical exclusion criteria included swelling or inflammation, severe pain or recent injury, and recent surgery to the hand. Respondents were instructed to press the dynamometer with their left and right hands, performing two repetitions with each hand. If a respondent had issues with one hand, measurements were only taken on the other hand. Instructions for the test required the respondent to stand upright, with the upper arm parallel to the upper body and the lower arm at a 90-degree angle to the upper arm. If necessary, the test could also be performed in a sitting position. The highest recorded value from these four measurements was used in the subsequent analysis. For this study, a low HGS was defined based on gender-specific thresholds, following the guidelines by the European Working Group on Sarcopenia in Older People (EWGSOP2), with thresholds of 27 kg for men and 16 kg for women [25].
The information about physical capacity and various diseases was obtained through a comprehensive assessment encompassing various aspects of physical function and medical conditions. This included inquiries about difficulties in performing activities of daily living, such as the ability to lift 5 kg, serving as indicators of functional capacity. Additionally, respondents self-reported several health conditions, including heart attack, hip fracture, rheumatoid arthritis, stroke, and osteoarthritis.
For inclusion in the sample, days with ≥ 23 h of valid wear time (as detected by ActiPASS) were required, and days without any detected sleep were excluded. Only respondents with at least three valid days were included in the final analysis.
Statistical analysis: We used multiple regression analyses to identify individual characteristics affecting the risk of any of the six diseases analysed. Hip fracture was excluded from the regression since there was no variation in outcome for some countries. A logit regression model was used due to the dichotomous nature of disease (either the presence or absence of disease in each respondent) by applying the following regression equation specification,
$$\:}\left( }} \right) = \beta + \beta + \beta + \cdots \: + \beta + \epsilon $$
(1)
where \( \pi \) is the risk of the disease, \(\:_,\:_,\dots\:,_\) are the k potential personal characteristics affecting the disease risk, \(\:_,_,\dots\:,_\) are the effects of those characteristics, and \( \epsilon \) is an error term.
The central right-hand side variables are 24-hour movement behaviours as defined above. Those four activities always sum to 24 h for any given person. Also, there is co-dependence between the four behaviours, e.g., when one activity changes than one or more activities will necessarily change as well. We thus have perfect collinearity, which means all four behaviours did not enter the regression equation in parallel. Instead, isometric log-ratio (ILR) transformations of the time-use composition were used as explanatory variables, and the health indicators as response variables [18, 26]. Through the approach, the relationship of each movement behaviour with the health indicator is measured correctly relative to the other three behaviours through log-ratios in accordance with the mentioned co-dependence between the corresponding four amounts of time derived from the 24-hour constraint. More specifically, ILR coordinates are used such that through a sequence of four ILR transformations of the complete time-use composition, the importance of each movement behaviour component relative to the geometric average of the remaining ones is isolated in turn in the first pivot coordinate to assess its association with the health indicator by logit regression analysis. Effectively, this leads to three pivot coordinates, each from a four-component time-use composition. For instance, the following specification is required to estimate the effect of the disease of sleep versus all other movements, respectively. The effect of light physical activity on MVPA,
$$\:_=il_=\sqrt\!\left/\:\!\raisebox\right.}\cdot\:ln\left(\frac}\right)$$
(2)
$$\:_=il_=\sqrt\!\left/\:\!\raisebox\right.}\cdot\:ln\left(\frac}\right)$$
(3)
$$\:_=il_=\sqrt\!\left/\:\!\raisebox\right.}\cdot\:ln\left(\frac\right)$$
(4)
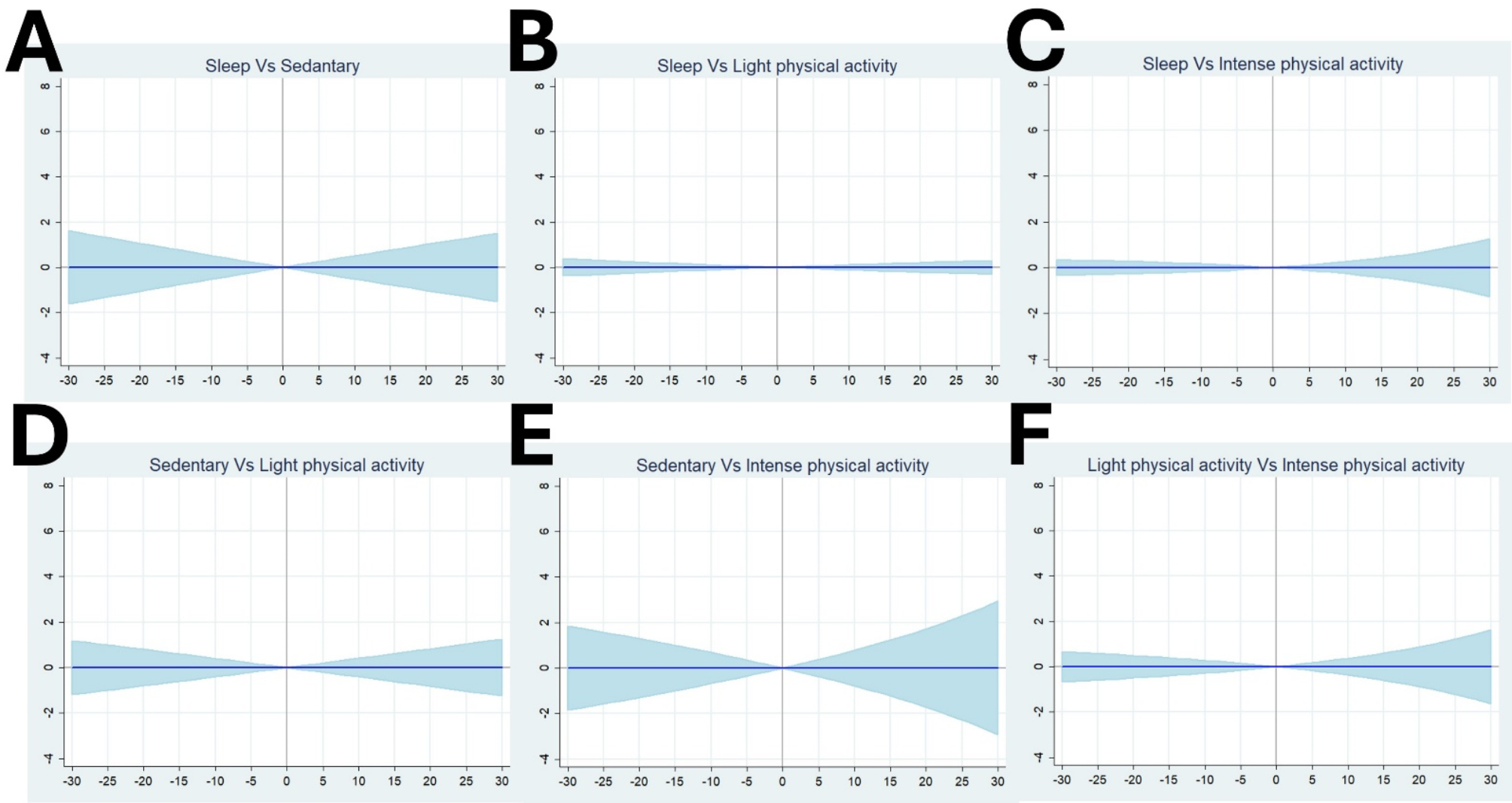
where SLP is sleep, SED is sedentary, LPA is light physical activity, and MVPA is moderate to intensive physical activity, while SLP + SED + LPA + MVPA = 24, and ln is the natural logarithm. These pivot-coordinates are used in the regression [1] above. The estimate (\(\:_\)) for the first pivot-coordinate in [2] is presented in Table 1, while the estimate (\(\:_\)) for the effect of the third pivot-coordinate is used to calculate the effect of changes of times between the two activities on the right-hand side of [4], which are displayed in Figs. 1, 2, 3, 4, 5 and 6. The activity changes were between Δ=-30 to Δ = 30 with 1-minute increments, evaluated at the means of all four activities. We can see from [4] that these effects depend non-linearly on a given activity (SLP, SED, LPA, and MVPA). Applying permutations of SLP, SED, LPA, and MVPA, we can estimate \(\:_\) for any of the four activities, as well as \(\:_\) for any combination of two of the four activities. The STATA software package 18.0 SE Standard Edition was used for the statistical analysis (Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC).
Table 1 Associations between changes in 24-hours movement behaviors (first ILR pivot coordinate) and changes in prevalence of a disease




Comments (0)