In this study, we evaluated the background patient characteristics and the impact of these characteristics on patterns of anticoagulation therapy of very elderly patients with NVAF aged ≥ 80 years, in particular those newly diagnosed after age 80 years, in Japan. We found that 606,800 (47.5%) patients with NVAF were aged ≥ 80 years, of whom 365,578 (60.2%) were newly diagnosed with NVAF after their 80th birthday and approximately 60% of these patients were on anticoagulation therapy for prevention of stroke/systemic embolism despite being of advanced age. Although we hypothesized that patient background and conditions would influence anticoagulant therapy, anticoagulation patters did not differ by the factors examined in this study, including ADL, CCI, number of prescribed drugs, or comorbidities.
Japan is a super-aging country with a large number of patients with NVAF over 80 years of age. In a Japanese disease registry, the ANAFIE registry, 19.6% of patients were aged between 85 and < 90 years, 5.7% were between 90 and < 95 years, and 0.8% were between 95 and < 100 years [23, 24]. In real-world analyses conducted in Western countries, the average age of patients with AF tends to be younger than in Japan. For example, in the study by Mantovani et al. using data from the GARFIELD-AF registry study [25], an AF patient registry enrolling patients from 50 countries, the mean ± SD and median (interquartile range) age of the patients was 69.62 ± 11.48 years and 71 (63–78) years. Populations of very elderly people have been increasing in Western countries as well, and it is expected that the number of very elderly patients with AF will also increase in the future in many countries.
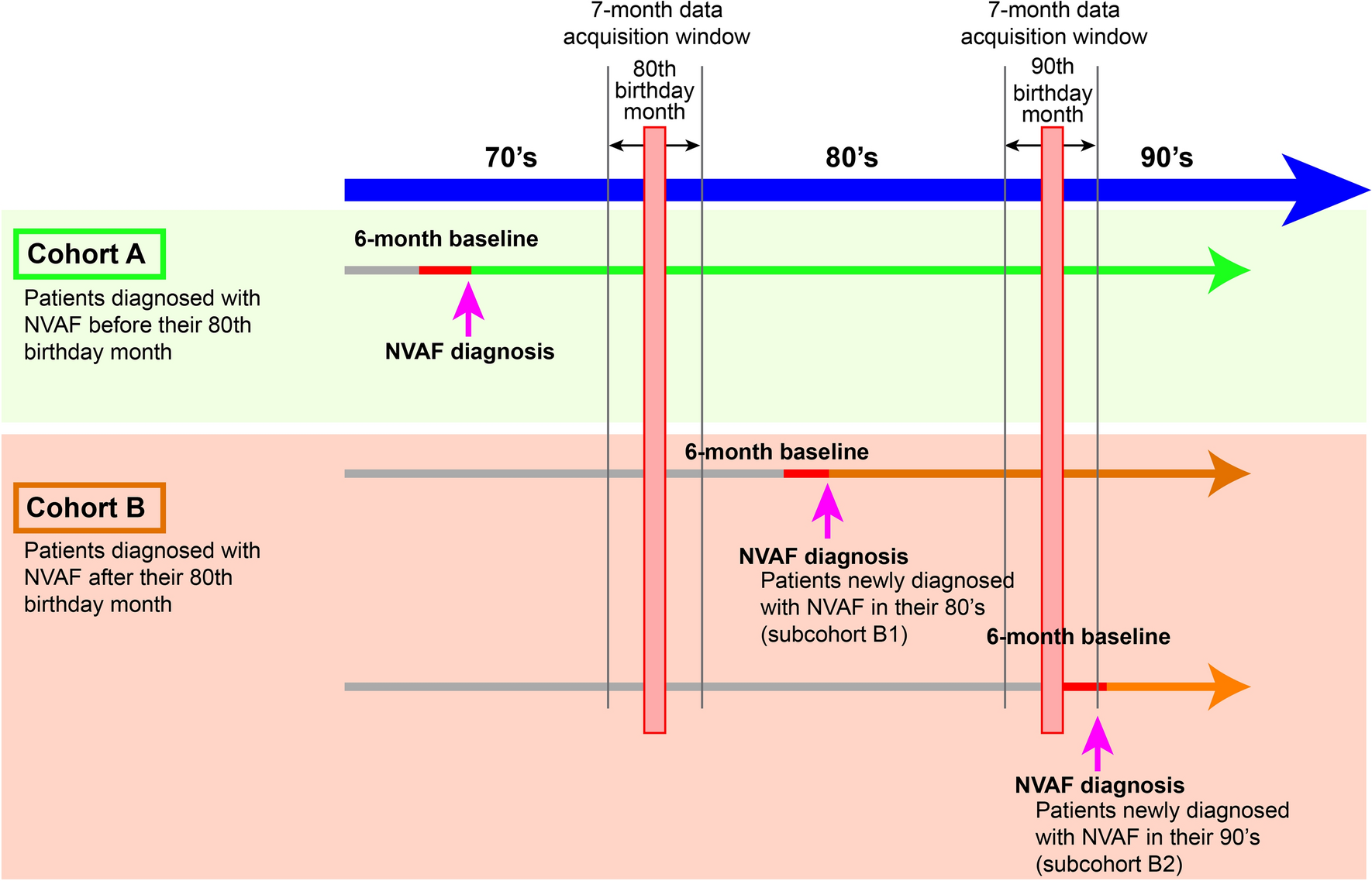
Elderly patients are generally thought to have a higher risk of stroke and bleeding. The HAS-BLED score, adopted in the 2010 European Society of Cardiology (ESC) guidelines as a predictor of major bleeding, includes advanced age as one of the risk factors [26]. Although ESC guidelines no longer recommend assessing each patient with a bleeding risk score, including the HAS-BLED score, in the 2024 revision, age and factors generally associated with the elderly, including high risk of falls, poor renal function, and cognitive impairment, are still listed as bleeding risk factors [27]. One of the major reasons why physicians may be hesitant to initiate anticoagulation therapy in the very elderly is this concern about bleeding. In this analysis, about 40–55% of the patients who were diagnosed after their 80th birthday did not receive anticoagulation therapy. Interestingly, among patients diagnosed with NVAF prior to age 80, there was a trend toward a higher percentage of patients not receiving anticoagulation therapy after their 80th birthday month. In contrast, patients diagnosed with NVAF after age 80 tended to be more likely to start anticoagulation therapy from the time of diagnosis, even if they were also over 80 years of age. The reason for this trend is unclear, but it is conceivable that there may be cases where anticoagulants were stopped at the discretion of the physician or at the request of the patient due to adverse events such as bleeding or drug costs as their use becomes more prolonged.
Several studies have shown that anticoagulation therapy is either not implemented in elderly patients with AF or, if implemented, is underdosed [26, 28, 29]. Our findings also show that most patients treated with DOACs were prescribed lower (reduced) doses, especially those newly diagnosed with AF over 80 years of age. Unfortunately, as data on body weight and renal function are not available in the MDV database for all patients, we could not determine whether the DOAC dose reductions were in accordance with the instructions in the package inserts or whether the underdosing was due to bleeding concerns or other reasons. Furthermore, information on prothrombin time-international normalized ratio (PT-INR) values in patients taking warfarin is available for some, but not all, patients, hence it is not known whether the PT-INR values were maintained in the appropriate guideline-recommended range. Based on the ANAFIE registry study and other previous reports, it is likely that many patients are underdosed (no anticoagulation therapy or receiving reduced doses not in accordance with the instructions in the package insert). There is no evidence that very elderly patients should be prescribed lower doses for safety reasons, and the present results by no means suggest lower doses for the very elderly patients. Further analyses using other data sources such as electronic medical record–based databases are needed to clarify the reality of inappropriate dose reduction.
In this study, we hypothesized that a patient’s clinical condition would influence the prescription of anticoagulants in very elderly patients with NVAF, and compared the CCI, Barthel Index (ADL), and number of medications (polypharmacy) between patients on and off anticoagulants to confirm our hypothesis among patients diagnosed with NVAF after age 80. Unexpectedly, there were no significant differences between the two groups with regard to the aforementioned factors. The reasons for this lack of difference are unclear, although there are several possibilities. First, in actual clinical practice, it is possible that the prescribing strategy is decided based on the age of the patient rather than the detailed background of the patient. Treatment strategies should be decided comprehensively based on the patient's background, but the lack of clear evidence and criteria regarding what factors should be considered and weighted may have contributed to this result. Second, apart from the patient's background and condition, factors such as the patient's financial status, environment, and cognitive level may have a greater impact on treatment strategy decisions. In the future, it is necessary to conduct analyses that consider the economic situation of the patients, the environment in which the patients receive care, and the background of patients who could not be examined in this study due to the lack of availability of their data in the MDV database.
In addition to anticoagulation, rate control and rhythm control strategies are also important treatment options in patients with AF. Although there is evidence that rate control is effective in terms of quality of life and prognosis [30, 31] and guidelines recommend it [31], evidence regarding its efficacy and safety in elderly patients has not yet been established [32, 33]. Despite the evidence and guideline recommendations, rate control is not always implemented in clinical practice, which poses a challenge for the management and treatment of AF [34]. Unfortunately, in this study, the percentage of patients who received rhythm control with antiarrhythmic drugs or catheter ablation could not be analyzed due to technical difficulties. The actual status of rhythm control in elderly patients with AF, the kind of patients who receive rhythm control in clinical practice, adherence to guidelines, and the relationship with anticoagulation therapy are issues to be addressed in the future.
Notably, elderly patients are also at a high risk for developing stroke as well as hemorrhage. Therefore, treatment should more carefully balance the risk of both hemorrhage and stroke (i.e., risk–benefit balancing). Further studies are needed to determine which patients should be treated with anticoagulation therapy, as well as the type of anticoagulation regimen that should be used.
Limitations
This study has some limitations that must be acknowledged. First, data were obtained from a claims database containing medical information provided by hospitals using a flat-fee payment system, which are large hospitals responsible for acute care. Therefore, a significant number of the patients included were likely in poorer health compared with the average population, possibly having more comorbidities and a higher risk of stroke/systemic embolism and bleeding. Second, determination of AF and other complications was based on ICD-10 codes assigned for insurance claims, which may differ slightly from the terminology used by physicians in the electronic medical record. Third, this was a descriptive study based on a survey of the real-world status of very elderly patients with AF. Therefore, the prognosis of the patients included in this study was not evaluated. Although an outcome study has been planned in the future, the relationship between anticoagulation therapy and prognosis needs to be evaluated in detail, as it will provide insights on an important clinical question pertaining to which patients should be treated and with which therapy. Fourth, the proportion of patients with a low Barthel Index was a lot higher than in the general very elderly population over 80 years of age. Although the exact reason for this is not clear, the following factors may play a role: (1) ADL is usually recorded by the physicians or nurses upon admission to the hospital as a part of DPC data. The condition of patients is evaluated at the time of admission when the patients are in poor condition. (2) As the patients included in this analysis are from acute care hospitals, the analysis may include patients transported from nearby nursing homes or chronic care facilities because of acute exacerbation of the illness. Not knowing the normal condition of each patient is one of the limitations of this study.







Comments (0)