Our study investigated students’ learning behaviour and their most used tools. The results have to be interpreted in light of the recent covid-19 pandemic, which had a significant impact on educational practices around the world [1]. According to our data, study habits of German medical students are mainly characterised by resource management learning strategies like effort (internal resource) and use of external sources of information and learning environment (external resources) combined with the predominant use of certain tools (lecture material, previous local exam questions, and commercial digital tools). The least used learning strategies were found to be the internal resource management strategy time followed by the cognitive strategies critical review and organisation. Regarding the difference between preclinical and clinical years, the strongest effect was found for the use of textbooks or other literature which was much less prevalent in clinical years. At the same time, students in their clinical years showed a significantly lower use of the cognitive learning strategy repetition, i.e. learning content by heart, compared to students in their preclinical years.
A notable aspect of the most used strategies is the high prevalence of resource management strategies such as external sources of information. As mentioned earlier, the items belonging to this scale can be interpreted in a wider sense than solely researching literature. Hence, this finding does not contradict the fact that working with textbooks or other literature was not among the most used tools, especially in the clinical years. More precisely, it supports the idea that commercially available digital tools gain popularity and may even replace conventional tools such as textbooks. Our results suggest that students use material provided by the medical school (i.e. lecture and seminar handouts, previous exam questions) to the same extent as commercially available products that are not aligned to the local curriculum.
The lower mean on the scale organisation, i.e. a rarer use of this cognitive strategy that is related to the in-depth work with and preparation of learning material, indicates less willingness to contribute something themselves and instead preferring to use premade material (e.g. summaries). A possible reason for this could be a lack of time in a full schedule, but it might also hint at the fact that medical students focus on performance goals rather than mastery goals. In other words, students attribute less importance to acquiring specific expertise which could be gained while researching for and creating summaries and instead concentrate on studying the material to pass exams. This hypothesis of a higher prevalence of performance goals is also supported by the low means for the learning strategy critical review, because critically engaging with the study contents might be more important for mastery goals than for performance goals. Nonetheless, critical review is an important aspect in the study process, especially for developing a scientific understanding which is important for any practitioner. Ratte et al. [24] showed that German medical students evaluated scientific competencies like critically reviewing relevant literature as important for themselves. Since our study demonstrated rather lower mean values on the scale critical review, we assume a discrepancy between students’ self-perception and actual use of scientific competencies.
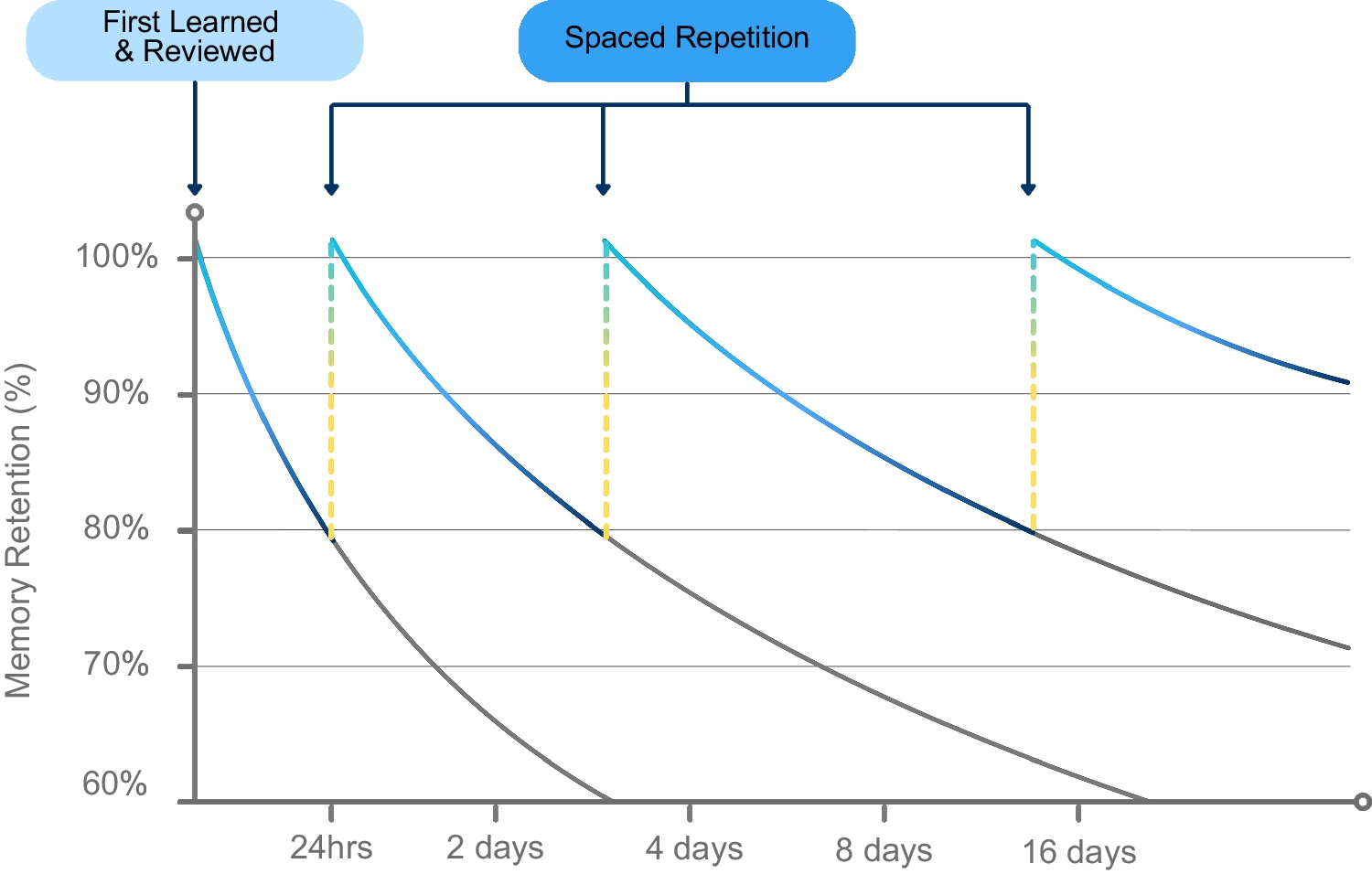
Furthermore, the results show a strong integration of previous local exam questions into the study process. Possible functions of using previous exam questions can be to check one’s level of knowledge, to identify knowledge gaps or to familiarise with the format of exam questions. However, applying this strategy comes with risks such as cueing effects (i.e. learning wrong answers as correct by reading them repeatedly) or limiting the study process on memorising answer options (as many questions are being used multiple times). Keeping the achievement goal theory in mind, the preferred use of previous exam questions could again implicate underlying performance goals. It also suggests assessment-oriented learning since the examination format is explicitly integrated into the study process. Testing oneself regularly can positively affect the retention of information, a phenomenon which is called the testing effect and increasingly examined in the context of medical education [25, 26]. In addition to the testing effect, other benefits of integrating frequent tests into medical education are discussed elsewhere (e.g. [27]).
The only significant mean difference in learning strategies between the preclinical and clinical years can be found for the learning strategy repetition. Items on this scale ask about memorising content, which is a classic example of a superficial learning strategy. The associated effect size is low, so the result has to be interpreted with care, but it suggests that students use this strategy less in the clinical years. A possible reason could be that the clinical years—by definition and conceptualisation—accentuates in-depth, practical training in clinical diagnosis and treatment while preclinical years emphasises the establishment of a strong (back-)ground knowledge. More practice-oriented forms of assessment such as objective structured clinical examinations (OSCE) are found in this study section which usually examine practical and clinically relevant skills such as doctor-patient communication or examination techniques [28]. This aligns with the concept of assessment-driven learning indicating that the implementation of more practice-oriented exams indeed affects the study behaviour of medical students in a sense that less superficial strategies are used. Nevertheless, since we only found a small effect size for the difference between the preclinical and clinical years, further research is necessary. In contrast to the study of Cordovani et al. [21], there was no significant difference in effort regulation between preclinical and clinical year students. Beyond that, we observed a different trend in our study, with effort scores being higher for the preclinical years compared to the clinical years. This discrepancy may be attributed to different operationalisations of learning strategies or to differences in underlying educational systems.
Regarding preferred media and tools, there was a significantly lower use of textbooks and other literature in the clinical years (12% vs. 36% in preclinical years). This is cause for concern in a way that advanced students appear to be less interested in acquiring in-depth knowledge and reading material that may not be imminently useful for exams. The strong emphasis on resources that will help students pass exams is understandable, but as this approach limits the breadth of content students are being exposed to, it may prove detrimental for clinical medicine and in fact life-long learning.
Practical Implications for Medical Education
Some of the findings reported here may be of particular interest to our medical school but if confirmed in other samples, they hint at general challenges medical education is faced with. The following suggestions can be derived from our results:
1.
Medical educational trainings for students
Based on the lower means on the scales critical review, organisation, and time, possible topics for medical educational trainings could be how to develop and use effective time tables, how to create helpful and well-structured content or lecture summaries, and what the benefits are in comparison to using premade summaries. In addition to that, those trainings could inform about the difference between performance and mastery goals or different forms of motivations in general. With such trainings, awareness on different learning strategies and motivation can be raised. However, these trainings will only have an effect on learning behaviour if flanked by curricular changes encouraging a deep approach to learning.
2.
More open and practice-oriented assessments
The apparent focus on studying with previous exam questions could be reduced by replacing multiple-choice exams with question formats on a higher taxonomic level. Increasing the number of OSCEs may also meet students’ ambitions for a higher practical orientation of their studies. Furthermore, open formats do not require a focus on niche topics to produce new multiple-choice questions that have not been used before. For a practical implementation, Hauer et al. [29] propose specific recommendations for generating and evaluating examinations like creating exam blueprints or standardised scoring criteria. If necessary, a possible compromise between practice orientation and efficiency can be found in the key feature approach with short-answer questions or multiple-choice questions. Key feature questions are suited to efficiently assess clinical reasoning, i.e. important decisions in the process of diagnosis and therapy [30, 31].
3.
Consideration of students’ study habits in curriculum development and teaching
Finally, the students’ wish for receiving lecture material like slides to prepare or repeat lectures could serve as a possibility to influence their study and learning process. To counter the risk of focusing on memorising the bullet points on the slides, information on the slides can be reduced to increase attention and critical thinking during lectures. Lecture material should also include current research topics or scientific literature to promote scientific competencies, which according to the study mentioned earlier are valued highly by students as well [24].
Limitations and Future Directions
Strengths of this study included the high number of participants and the use of a validated questionnaire (LIST-K; [23]). Furthermore, the gender distribution in the sample is comparable to the actual gender distribution in German medical schools considering that in 2022, 64.4% of German medical students were female according to the German Federal Statistical Office [32]. In contrast to other recent studies [20], both students in the preclinical and the clinical years were included, allowing comparisons between the two groups. However, a longitudinal design would have allowed making statements about intra-individual changes and hence should be aimed for in the future. Other limitations should be considered when interpreting the results and drawing conclusions as well. For example, this study explicitly examined medical students’ study habits operationalised by their learning strategies as well as the media and tools they used. Certainly, the learning process is not limited to preparing for lectures or exams but also includes implicit learning sites during internships and practical study sections (e.g. bedside teaching, practising consultations with simulated patients), which were not specifically addressed by the questionnaire. Future studies should examine learning in a wider sense, for example by including a number of learning sites in the survey.
Moreover, an intriguing direction for future research would be to explore the relationship between study habits, students’ performance, and exam scores. Additionally, it might be interesting to repeat this study in the later future since the results of our survey might still be influenced by the shift to digital education during the covid-19 pandemic.
Another limitation of the study is the restriction to one German university, which of course cannot be seen as representative for the whole population of medical students. The study should be extended to different universities in Germany as well as beyond. Thus, an intercultural comparison of different national educational systems and a comparison of different programmes within the same educational system can be achieved.



Comments (0)