Dry needling is creating meaningful developments in sports medicine and physiotherapy practices, expanding its scope beyond traditional clinical settings to enhance athlete recovery and pain management. This systematic review identifies various methodological approaches to dry needling in sports performance and recovery. A multitude of studies investigating these approaches has been observed, with case reports and randomized experimental studies being the most prevalent.
Pain perception emerged as one of the most extensively researched outcomes, regardless of whether the focus was on postexercise recovery or injury rehabilitation. Regarding athletic performance, a wide range of outcomes has been observed, encompassing improvements in range of motion, muscular strength, and physiological responses. Concerning different applications of dry needling, there is a notable emphasis on targeting the lower limbs or shoulders, with relatively few studies concentrating on other regions of the body. The findings exhibit diversity, indicating that, while dry needling shows an important effect on reducing pain, its impact on enhancing athletic performance parameters appears to be less pronounced.
4.1 Methodological Characteristics and Coverage of Dry Needling Studies in Sports
The discussion on the methodological characteristics of dry needling in sports focuses on the populations studied (e.g., sports represented, competitive level, and sex), as well as the specific study designs and outcomes and the context.
4.1.1 Populations Included in Dry Needling Studies in Sports
This systematic review has revealed that the majority of studies involving sports athletes focus on talent development and highly trained national-level athletes, highlighting a lack of research on highly competitive athletes at the elite or international/world-class level [47]. Furthermore, Paralympic athletes were only included in two studies, namely those conducted by Aidar et al. [40] and Dos Santos et al. [39]. The larger sample size and less congested competition schedules faced by athletes at smaller competitive levels probably make it easier to conduct experiments. However, the underrepresentation of specific competitive levels (such as elite or world-class) or Paralympic athletes may make it difficult to generalize evidence and ensure the suitability of interventions for these populations, who are subject to high levels of strain and require more comprehensive recovery strategies [48].
Regarding sex representation, most studies included both men and women. Interestingly, among those focusing solely on one sex, there was a notable balance between studies concentrating on men and women. This reflects the importance of achieving a more equitable representation of women as research subjects in sports. One possible explanation for this balance could be the greater equilibrium in the sex of the authors of studies, which appears to influence the ultimate research focus [49]. However, in different contexts, women remain underrepresented, resulting in imbalances in the understanding of interventions concerning the specificities of biological characteristics [50].
4.1.2 Study Designs and Outcomes Analyzed in Dry Needling Research in Sports
Among the various study designs, randomized experimental studies were the most prevalent, underscoring a commitment to rigorous scientific analysis within the field. Case reports also maintained a significant presence, likely contributing valuable anecdotal evidence and insights into individual cases. However, notably absent were cohort studies, which could offer deeper insights into the long-term effects and broader applicability of dry needling in athletic contexts. This deviation from common research practices in sports is intriguing, as observational studies typically dominate, whereas experimental studies are often less prevalent [51]. While experimental studies provide internal validity, nonexperimental studies, such as cohort studies, may offer information about longer exposure periods to dry needling [52], facilitating a better understanding of its efficacy and potential limitations as a long-term therapeutic practice in sports medicine. This, in turn, could guide more informed decision-making within the athletic community.
The reviewed studies on dry needling exhibited considerable variability in protocols, including differences in needle insertion duration (ranging from 5 to 15 min), number of insertions (from 3 to 12 needles), techniques used (e.g., “fast in, fast out” versus pistoning), and the incorporation of electrical stimulation or ultrasound guidance. These differences highlight a lack of standardization in dry needling dosages, with inadequate reporting of critical parameters such as insertion depth, total treatment time, and specific pain tolerance thresholds. To improve future research, it is recommended that protocols standardize these variables, clearly define dosage parameters, and incorporate consistent reporting guidelines to enhance reproducibility and clinical relevance.
Considering the outcomes of studies on dry needling among sports athletes, there appears to be a consistent focus (75%) on analyzing and reporting outcomes related to pain perception. This emphasis on pain assessment aligns with the primary objective of investigating the effects of dry needling. Specifically, dry needling targets trigger points, which are hyperirritable spots in skeletal muscle characterized by palpable nodules or taut bands of muscle fibers [53]. These trigger points can manifest as localized or referred pain, as well as muscle tension [54]. Needles are inserted into these trigger points to alleviate pain perception by disrupting the neural pathways involved in pain signaling [55]. Consequently, it is reasonable to anticipate that research outcomes regarding pain relief could be explored more comprehensively, regardless of whether they are conducted in postexercise or injury recovery contexts.
In studies focusing on athletic performance outcomes (58.3%), muscular strength and range of motion emerged as the most prevalent areas of investigation, whereas physiological adaptations were examined in fewer studies. It is hypothesized that impairments in athletic performance (e.g., postexercise), such as muscular performance, can be mitigated by managing pain reduction [56], while limitations in range of motion can be addressed by releasing tight muscles and promoting muscle relaxation [57]. Therefore, rather than testing the effects for improvements in athletic performance, studies examining physical performance have aimed to analyze how dry needling could alleviate impairments in physical performance postexercise or during injury processes.
4.1.3 Contexts of Studies on Dry Needling in Sports
In terms of the primary focus of research, the majority of postexercise studies employed experimental designs. Conversely, a more balanced distribution was observed in case reports regarding the reporting of pain-related outcomes and variations in athletic performance. Experimental studies involving injured athletes were relatively rare, likely owing to the complexities associated with recruiting injured athletes compared with the relatively simple process involved in case reports, which require fewer participants.
Considering the body regions targeted by interventions, particularly in connection with sports, a wide array of sports was represented (e.g., soccer, volleyball, running, handball, pole vaulting, and triathlons). Among these, the lower limbs were the most frequently addressed (58.3%), with a focus on muscles such as the gastrocnemius and thigh. Conversely, in the upper region, the shoulder muscles received the most attention (20.8%).
In sports modalities involving overhead movements (e.g., volleyball, handball, and tennis), the shoulder often experiences overuse, pain, and injuries [58], making it justifiable to prioritize research in this area. Meanwhile, hamstring injuries are commonly a focal point in sports requiring significant lower limb engagement (e.g., running and soccer) [59]. However, dry needling research in sports has predominantly concentrated on the gastrocnemius, possibly owing to the prevalence of studies involving runners who frequently experience muscle soreness in this area [59], as well as the thigh. It may be prudent to increase the focus on hamstring muscles in future studies to complement potential physiotherapy interventions or alleviate pain resulting from progressive increases in load, which often occur at specific points in the season (e.g., preseason).
4.2 Dry Needling and Its Impact on Pain Alleviation in Sports Athletes
It is hypothesized that dry needling stimulates a cascade of neurophysiological events, including the release of endogenous opioids [60], such as enkephalins and endorphins [61], which act as natural pain relievers. Additionally, the insertion of needles into trigger points within the muscle tissue triggers a localized twitch response, which is believed to disrupt the dysfunctional motor endplate activity associated with chronic muscle pain [62]. Furthermore, dry needling has been shown to increase blood flow to the affected area [63], facilitating the delivery of oxygen and nutrients while aiding the removal of metabolic waste products. This enhanced circulation promotes tissue healing and reduces inflammation [64], possibly contributing to the attenuation of muscular pain symptoms.
It is justifiable to emphasize researching the pain symptoms experienced by athletes following interventions with dry needling. Some of the included studies demonstrated significant improvements in pain symptom alleviation, particularly in postexercise scenarios, as evidenced by studies such as those conducted by Benito-de-Pedro et al. [27], who reported reductions of 26.2% in pressure pain threshold, and Walsh et al. [20], who observed reductions of 4.3–10.7% in pressure pain threshold compared with control groups. However, studies such as those conducted by Cushman et al. [31], Dos Santos et al. [39], and Huguenin et al. [34] did not reveal significant effects when compared with control groups.
4.2.1 Studies Involving Athletes Experiencing Injuries or Musculoskeletal Pain or Dysfunction
In studies involving athletes experiencing injuries or musculoskeletal pain or dysfunction (e.g., shoulder pain, tennis elbow syndrome, scapular dyskinesia), significant positive effects in pain relief were observed compared with control groups. For instance, Ceballos-Laita et al. [38] reported that pain intensity decreased by 82.5%, Etminan et al. [45] found that the pain rate dropped by 88.4%, Kheradmandi et al. [46] observed that pressure pain threshold decreased by 0.7%, and Zarei et al. [7] showed a numerical pain rating score of − 75.9%. However, one study conducted by Janowski et al. [35] on ballet dancers with calf pain reported no significant differences between the treatment and control groups.
Additionally, in athletes experiencing pain and injuries, the presence of localized pain or injuries may provide more homogeneous targets for dry needling interventions. The focused nature of the injury site and the repetitive stressors inherent in athletic activities [60] may create a more conducive environment for consistent pain reduction outcomes with dry needling. Furthermore, the underlying pathology is often more clearly delineated in this population than in the population of nonathletes, allowing for a targeted and standardized approach to dry needling application, thus contributing to the observed effectiveness in reducing pain intensity across studies.
4.2.2 Studies Focusing on Postexercise Recovery
In postexercise scenarios, the efficacy of dry needling in pain management presents a landscape marked by inconsistent findings. The variability in outcomes can be attributed to multifactorial influences, notably the divergent physiological responses following exercise. Postexercise pain dynamics involve complex mechanisms, including inflammatory processes, neural sensitization, and tissue remodeling [65], which may interact with dry needling interventions in heterogeneous ways across individuals and study designs. Additionally, factors such as the timing of interventions relative to exercise cessation (which varied in terms of implementation time and subsequent follow-up periods ranging from 24 to 48 h or more) [30], the fitness level and intensity and duration of exercise [66], and individual pain perception thresholds [67] contribute to the observed discrepancies. Therefore, the efficacy of dry needling in postexercise recovery may depend on individual factors, highlighting the need for further research to identify those who may benefit most from the intervention [68].
In studies reporting significant improvements, the duration of dry needling interventions tended to be longer compared with postexercise studies, which often involved a single session. This trend is exemplified by, for instance, studies by Etminan et al. [45], which was composed of nine sessions over 3 weeks; Zarei et al. [7], which included 20 sessions over 4 weeks; and Kheradmandi et al. [46], which involved three sessions. Therefore, the duration and frequency of dry needling interventions could be concurrent factors that influence variations. Consequently, future research should explore and compare the frequency and duration of dry needling interventions to understand whether these factors can modulate how athletes manage pain or perceive the potential benefits of dry needling. Additionally, comparing possible extents is crucial, as the immediate acute effects can vary in duration depending on the athlete. This line of inquiry may unveil individualized thresholds or identify effective minimum doses for optimal outcomes.
4.3 Dry Needling and Its Influence on Neuromuscular Function, Range of Motion, and Physiological Parameters
While the primary focus of dry needling in sports applications is pain management, their pain reduction could also enhance subsequent muscular performance or increase range of motion, thereby improving athletes’ physical capabilities during recovery. For instance, dry needling may facilitate improvements in muscle stiffness and motoneuron excitability of latent medial myofascial trigger points. However, the evidence is inconsistent and typically does not strongly support this hypothesis [56, 69, 70].
Studies tend not to show any significant effects of dry needling on muscle force production. For instance, Ceballos-Laita et al. [38] found no significant difference in internal and external rotation strength among handball players with shoulder pain compared with the control group. Additionally, Devereux et al. [33] revealed that, while maximal force and power were not significantly enhanced by dry needling compared with the control group, jump height improved 48 h after the intervention in male field sport athletes with latent myofascial trigger points in the rectus femoris and medial gastrocnemius muscles bilaterally. Furthermore, Etminan et al. [45] observed athletes with chronic tennis elbow and found no significant effects of dry needling compared with the regular physiotherapeutic approach in terms of grip strength. Similarly, Janowski et al. [35] observed no significant effects of dry needling on triceps surae torque among ballet dancers experiencing calf pain compared with the control group.
4.3.1 Studies Involving Athletes Experiencing Injuries or Musculoskeletal Pain or Dysfunction
In athletes with unilateral shoulder pain, Ceballos-Laita et al. [38] found that individuals exposed to dry needling exhibited more significant changes than the control group in internal rotation range of motion, external rotation, glenohumeral internal rotation deficit, external rotation gain, and extensibility. Conversely, Janowski et al. [35], who studied the effects on ballet dancers, found no statistical difference in lunge range of motion measurements between the dry needling and sham groups. Variations in study methodologies, such as the timing of effects analysis, which may have influenced the observed effects such as duration, along with differences in participant characteristics (e.g., shoulder pain and calf pain) and treatment durations, may have contributed to such discrepancies.
Concerning the balance of athletes dealing with pain and injuries, López-González et al. [36] found that basketball players with chronic ankle instability who underwent dry needling demonstrated statistically significant improvements in static postural control measures. These improvements were evidenced by decreased sway variability and center of pressure displacement among those who received dry needling compared with those who did not.
Additionally, Zarei et al. [7] reported that incorporating dry needling into regular physiotherapy interventions revealed clinically significant improvements in functional performance only in the dry needling group during dynamic balance testing. One possible explanation is that dry needling can enhance proprioception and sensory feedback necessary for maintaining balance [71]. However, regarding postexercise recovery, Benito-de-Pedro et al. [29] found no significant effects of dry needling on static plantar pressure compared with the ischemic compression group. Thus, further research is necessary to comprehend the mechanisms underlying the reported evidence. Comparative analyses are also needed to identify the influence of dry needling on the health of both injured and uninjured athletes.
Regarding physiological responses, Janowski et al. observed significant differences in mean temperature when investigating ballet dancers experiencing calf pain and comparing dry needling versus sham dry needling [35]. Specifically, both the right and left calves in the sham group, as well as the right calf in the dry needling group, exhibited noteworthy differences in temperature [35]. One potential explanation for the decrease in muscle temperature in dry needling is the activation of the descending pain inhibitory pathways, triggered by the insertion of the needle into the muscle tissue [72]. This activation can lead to the release of endogenous opioids and neurotransmitters such as serotonin and norepinephrine [60], which may induce local vasodilation and increase blood flow [63], consequently reducing muscle temperature.
4.3.2 Studies Focusing on Postexercise Recovery
Regarding postexercise recovery, a single session of dry needling was less effective than cold water immersion in restoring maximal force in Paralympic powerlifters according to Dos Santos et al. [39]. Conversely, Haser et al. [22] reported that soccer players exposed to dry needling experienced significant benefits in muscular endurance and hip flexion range of motion compared with the placebo group.
Considering range of motion, it has been hypothesized that dry needling can reduce muscle tone and tension by eliciting a local twitch response within trigger points, thus relaxing the affected musculature [73]. This reduction in muscle tension may allow for increased flexibility and range of motion in the targeted muscles [74]. In a postexercise context, Benito-de-Pedro et al. [29] revealed no significant differences in the dorsiflexion range of motion at the tibiofibular–talar joint or in static and dynamic plantar pressure alterations before and immediately after the intervention.
Regarding physiological responses, Aidar et al. [40] investigated dry needling’s impact on postexercise recovery in Paralympic powerlifters. Their findings revealed a decrease in systolic blood pressure immediately following dry needling treatment. However, a contrasting pattern emerged at 50- and 60-min post-recovery. The passive recovery method resulted in a significantly higher heart rate and doubled product values compared with both cold-water immersion and dry needling. Similarly, Dos Santos et al. [39] observed members of the same cohort and demonstrated that dry needling was the only intervention associated with increased interleukin (IL)-2 levels at various time points. Muscle thickness did not increase following dry needling; conversely, cold water application led to greater muscle thickness at 15 min and 2 h post-treatment. These results suggest that cold water immersion facilitates effective recovery up to 24 and 48 h postexercise, while dry needling appears to be a favorable option within the initial 24-h recovery window.
In a study focusing on postexercise recovery in triathletes, Benito-de-Pedro et al. [27] reported no statistically significant differences in thermography measurements between two treatment modalities: dry needling and ischemic compression. This lack of significant differences was consistent across the superficial zone adjacent to latent myofascial trigger points and corresponding anatomical locations with healthy soft tissue in the contralateral limb, before and after treatment.
4.4 Adverse Effects of Dry Needling
Dry needling may pose potential risks to patients, albeit with minimal frequency and severity. For instance, in a survey involving 39 physiotherapists [15], commonly reported adverse effects included bruising, bleeding, pain during treatment, and post-treatment pain. While such mild adverse effects were frequently cited, significant adverse events were rare [15].
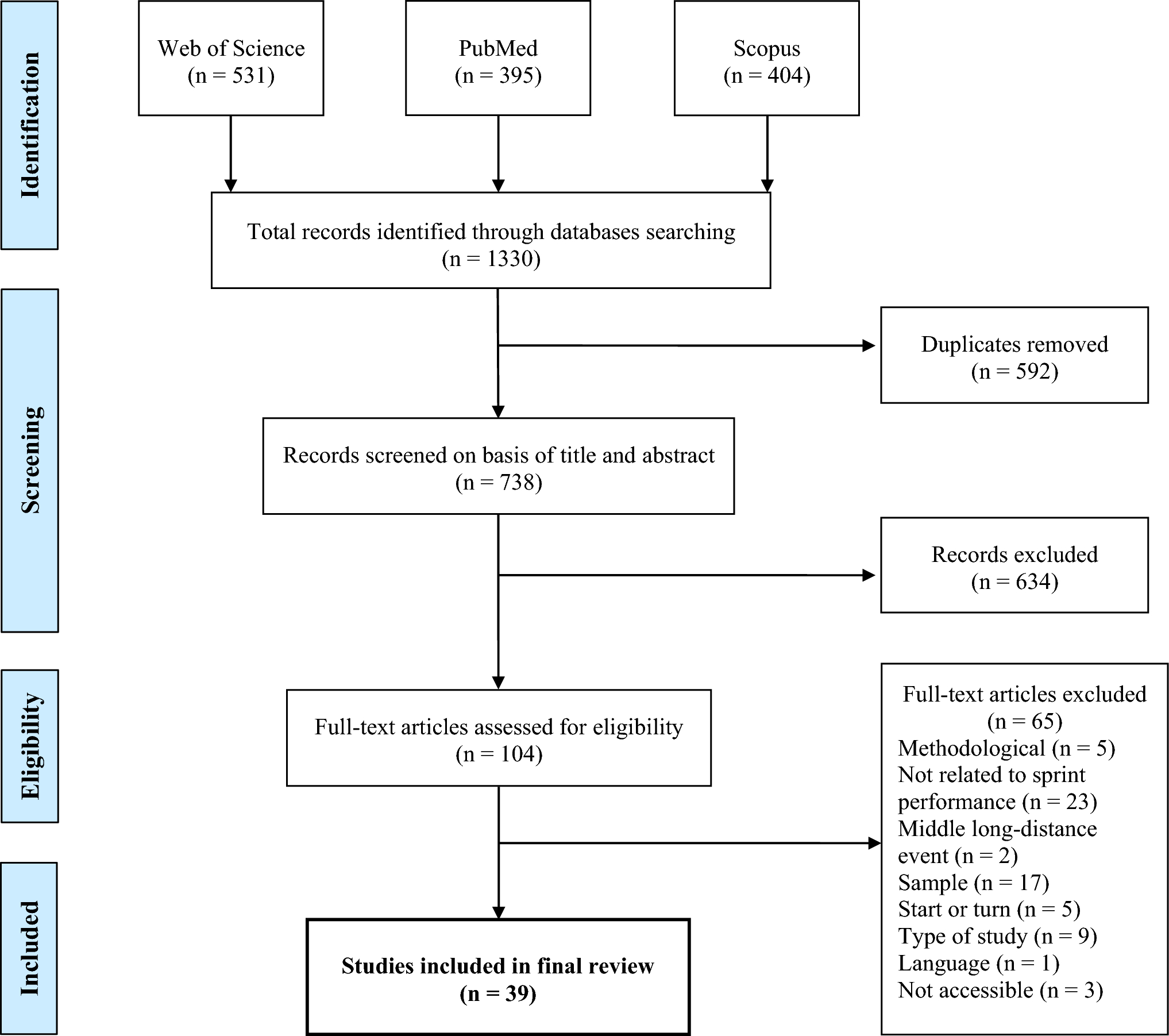
Among the 24 studies analyzed in our systematic review, only 3 explicitly documented adverse effects. Benito-de-Pedro et al.’s [29] study, which involved 17 athletes undergoing dry needling, noted two cases of local hematoma in the treatment area. Moreover, Brewster et al. [30] observed minimal and tolerable pain during needle insertion at various sites as the sole adverse reaction. Additionally, Huguenin et al. [34] noted that two subjects experienced syncopal responses to needling, but they recovered swiftly and completed the study. Meanwhile, one participant initially reported atypical chest pain, but this was resolved after a thorough medical evaluation, and the participant resumed the trial 2 days later.
Despite these isolated incidents, the majority of studies either reported no adverse effects or did not provide detailed documentation. However, there is inconsistency in reports of dry needling dosing parameters and adverse effects [75]. Without more comprehensive reporting, future studies will face significant limitations in replicating the methods of previous experiments and advancing the understanding of dry needling’s efficacy and safety profile.
4.5 Study Limitations and Future Research
The current analysis of the identified methodological characteristics revealed a prevalent risk of bias stemming from the lack of blinding among participants and therapists, as well as insufficient detail regarding allocation concealment. These issues require significant consideration. Blinding, also known as masking, is a pivotal methodological tool that mitigates bias in research. The knowledge that participants or researchers have regarding the treatment administered can influence their behaviors and evaluations, potentially distorting the results. For example, participants who are aware that they are receiving an experimental treatment may report more favorable outcomes owing to placebo effects or subconscious biases. Likewise, if researchers are not blinded to the treatment, their expectations and interactions with participants could subtly sway the study’s outcomes.
Furthermore, allocation concealment is crucial in ensuring the impartial assignment of participants to various treatment groups. Inadequate concealment raises the risk of selection bias, by which researchers may consciously or inadvertently influence group assignments based on factors beyond randomization, thus compromising the study’s internal validity.
A review of the methodological report indicated that the significant limitations commonly found in the studies included in this systematic review pertain to the reporting of dosages, specific treatment procedures, and intervention details. This observation aligns with a previous systematic review [75] that underscored inconsistencies in reporting dry needling dosing parameters and adverse effects. The failure to accurately determine the effects of dry needling dosages on outcomes could introduce bias into decisions regarding its clinical efficacy or optimal dosage.
Future research should prioritize enhancing the quality of reporting on treatment procedures, dosages, and adverse effects, perhaps by adopting standardized reporting protocols tailored to these specific elements. Additionally, regarding the evidence gap map, it is crucial to expand the inclusion of elite and world-class athletes while also integrating more Paralympic athletes into studies. Furthermore, there is a need to incorporate a broader range of neuromuscular and physiological outcomes in experimental studies. Moreover, longitudinal cohorts are recommended to provide a comprehensive, long-term perspective on the effects of dry needling experienced by athletes.





Comments (0)