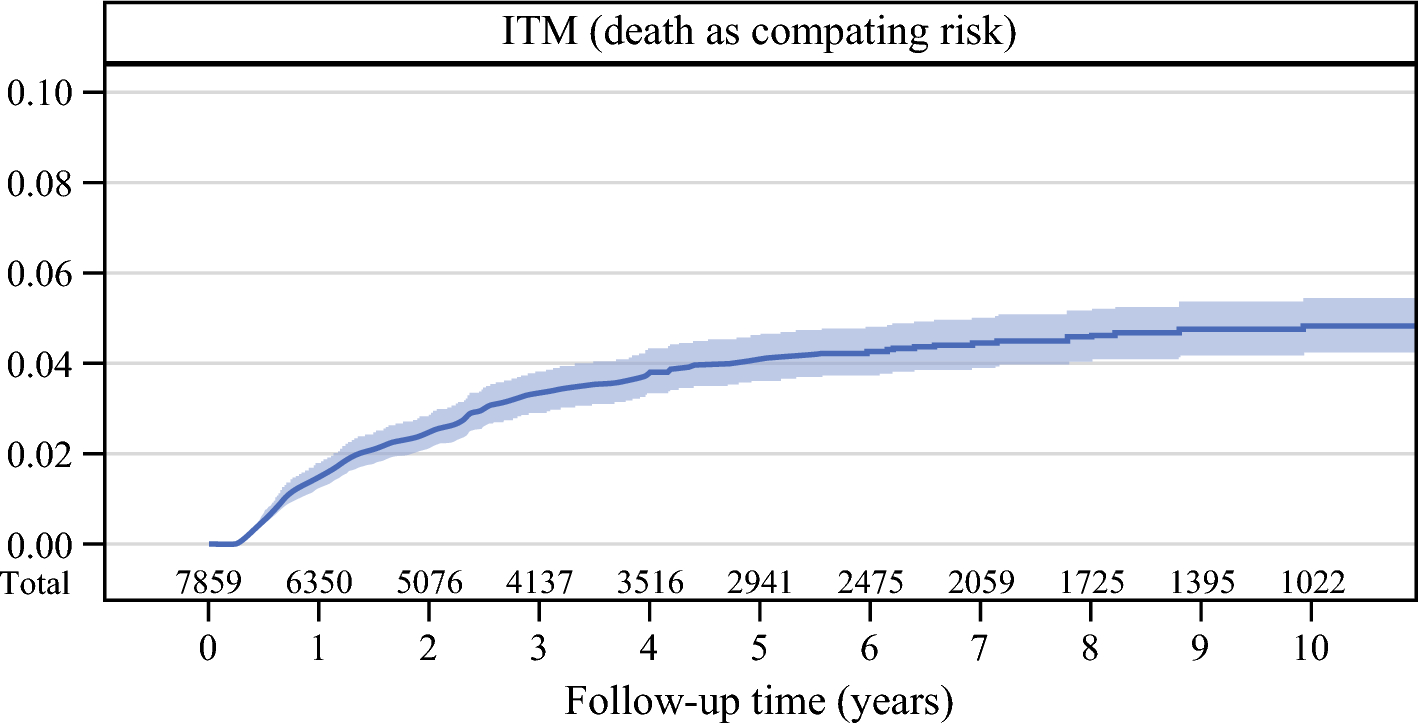
In this large multi-institutional and international retrospective registry study, we found the 5-year risk for development of an ITM as a first recurrence to be 4.12% and the 10-year risk to be 4.81%. A majority (81%) of all the patients who experienced an ITM recurrence did so within 3 years, and the risk of experiencing an ITM after 5 years was very low. Breslow thickness, lower-extremity melanoma, age, number of positive SLNs, and vascular invasion all were strongly associated with the risk of ITM recurrence. Interestingly, in contrast to de novo melanoma, the presence of a pre-existing lesion appeared to be an independent protective factor against the development of ITM.9 Ulceration was significantly associated with ITM in the univariable analysis, but was no longer statistically significant in the multivariable analysis.
Our reported ITM risk rate of 4.81% was closely aligned with the 4.3% found in the large study by Read et al.3 from the MIA study (n = 11,614), and slightly higher than the 3.2% reported in the smaller study by Jakub et al.10 from the Mayo clinic (n = 854). The differences can likely be attributed to variations in study populations and follow-up times because our study had a longer median follow-up period of 47.1 months compared with 40.6 months in the MIA study and a duration more comparable with the 49.2 months reported in the Mayo study. These findings collectively support a consistent risk range for ITM across diverse cohorts.
In the MIA study, ITM was defined as cutaneous, intradermal, and subcutaneous metastases occurring 5 cm or further from the primary site, whereas it was defined as further than 2 cm in the Mayo study. The agreed upon definition of ITM in the National Comprehensive Cancer Network (NCCN) guidelines is a metastasis further than 2 cm beyond the primary tumor.11 The differentiation between satellite metastases and ITM in melanoma has traditionally been made on the basis of their presumed biologic behavior. However, there are compelling reasons to see them as one entity, and current guidelines suggest a combined definition that includes both ITM and satellite metastases as a locoregional recurrence.12,13
Several pathophysiologic mechanisms have been suggested for the development of in-transit recurrence, such as tumor cell dispersion through tissue fluid and implantation of tumor cells in the subcutaneous tissue after spread via the bloodstream.14,15 The hypothesis that it originates from tumor cell emboli entrapped in the dermal lymphatic vessels between the primary site and the regional lymph node basin is the most widely accepted.3 This suggests an analogous tumor mechanism and dissemination for both satellite metastasis and ITM. In clinical practice, our approach to managing locoregional recurrences, both satellite metastasis and ITM, is guided by the extent of the tumor burden, the interval since the last recurrence, individual patient characteristics, and available treatment options, but very seldom by distance from the primary tumor.
Our findings that SLN positivity was predictive for ITM further support the hypothesis of lymphatic spread as the pathophysiologic mechanism of ITM development. The association between a positive SLN and a higher incidence of ITM further supports the hypothesis of lymphatic spread, in which melanoma cells traverse lymphatic vessels to reach the SLN. Conversely, the significantly lower incidence of ITM in cases with a negative SLN indicates that melanoma cells typically remain confined to the primary site in the absence of SLN involvement. With an average size of up to 20 μm, cancer cells can easily enter lymphatic vessels, which have an average diameter of 100 μm, and travel toward the lymph nodes.16 It has been proposed that clusters of cancer cells may obstruct lymphatic vessel valves, potentially forming colonies along the vessel walls. These colonies could then invade surrounding tissues, contributing to ITM. Additionally, cancer cells may possess specific receptors enabling adhesion to the lymphatic endothelium, providing a mechanism for further growth and dissemination.17
In our study, we found that the median time to development of an ITM recurrence was 15 months after definitive resection of the primary melanoma, and that the risk for the development of an ITM after 5 years was low. Approximately 80% of all first recurrences of ITM were experienced within 3 years. Previous studies investigating the time to development of an ITM recurrence have reported similar recurrence intervals. The median time was reported to be 18 months in the aforementioned MIA study3 and 16 months in the study from the Mayo clinics.10 The low risk for the development of ITM beyond 5 years may reflect an incubation period, with ITM peaking approximately 3 years after treatment and declining thereafter. This pattern could be influenced by a dormancy phase of disseminated melanoma cells and the evolving role of the host immune system over time.
Our study identified a subset of clinicopathologic factors that were independently predictors of ITM recurrence: Breslow thickness, lower-extremity location, age, number of positive SLNs, and vascular invasion. These findings all align with the existing literature. Pawlik et al.2 reported on 91 patients who experienced ITMs in a cohort of nearly 1400 melanoma patients undergoing SLNB. Their analysis identified Breslow thickness, age older than 50, ulceration, and lower-extremity primary location as poor prognostic factors for ITM development. The current data could be used and validated in other datasets to identify a low-risk group of patients at risk for ITM.
A limitation of our study was the lack of routinely collected data on systemic treatments administered to patients with ITM, as well as data on nodal recurrence, distant metastasis-free survival, and overall survival.
In conclusion, in this large international cohort of patients with melanoma, the 5-year risk for the development of ITM as a first recurrence was 4.12%. The independent risk factors for the development of ITM were Breslow thickness, lower-extremity melanoma versus trunk melanoma, increasing age, number of positive SLNs, and presence of vascular invasion, whereas the presence of a pre-existing lesion in the primary tumor was a protective factor.





Comments (0)