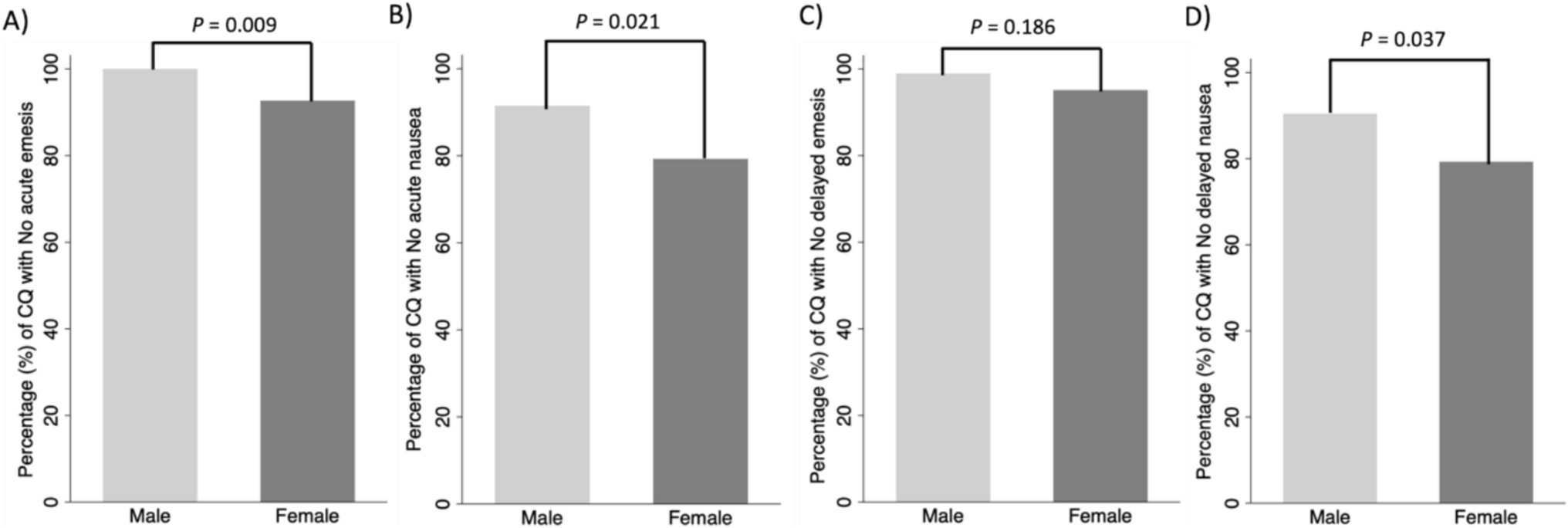
To our knowledge, this is the first prospective study specifically designed to assess the incidence of CINV among both sexes. We showed that females have a higher incidence of CINV, especially acute emesis and acute and delayed nausea. These differences were especially notable in the high emetic potential regimens, probably influenced by the larger sample size and because CINV symptomatology is most aggravated in this subgroup in females. Female sex and young age were shown to be clear predictors of non-CR, while habitual smoking and moderate emetic risk schemes may reduce the frequency of CINV. In males, no predictors of non-CR were identified, whereas in females, young age and pregnancy-related nausea and vomiting contributed to it. A high percentage of patients reported adverse effects, constipation being the most common one, especially in females.
It is well-known that the incidence of CINV differs based on sex, as has been proven in different studies [16, 19, 24,25,26,27,28,29]. Sekine et al. and Hilarius et al. demonstrated a higher incidence of CINV in females, both in the acute and delayed phases, as well as a relationship between the number of risk factors and the occurrence of CINV [5, 16]. Binder et al. confirmed that CINV rates were higher in young females than in males [28]. Zhao et al. evaluated the incidence of CINV in highly emetic chemotherapy, proving that females with no history of alcohol intake and a larger body surface area undergoing high doses (≥ 70 mg/m2) of cisplatin were more vulnerable to chemotherapy-induced nausea [29]. Uchida et al. found female sex, age < 60 years, no habitual alcohol intake, and ECOG score of 1 to be significant risk factors associated with non-CR [25]. Tsuji et al. in patients treated with highly emetic chemotherapy, revealed that sex and age, among other factors, were significant and independent factors affecting CINV in the overall phase [26]. The systematic review and meta-analysis conducted by Mosa et al. analyzed the influence of sex in 32 studies, and of those, 18 studies confirmed that female patients are at higher risk of CINV than male patients (p < 0.05), showing a summary odds ratio of 2.79 (95%CI 2.26–3.44) [24]. In our study, the OR in the overall cohort was even higher, 3.70 (95%CI 1.70–8.08) in the univariate analysis and 4.45 (95%CI 1.58–12.55) in the multivariate analysis, confirming the results of the meta-analysis and previous studies.
Young females are at high risk of suffering CINV, especially those who suffer from emesis and nausea during pregnancy. It may be due to nausea and vomiting, usually caused by conditioned stimuli. Patients with a prior history of this effect are at higher risk of suffering it again when they are exposed to the same stimuli [14]. In addition, aging in women seems to be a factor that decreases the incidence of CINV. Menopause has been shown to influence the severity of nausea; probably, changes in FSH and E2 due to menopause may affect the severity of nausea [30]. In our study, this hormonal status was not collected. However, according to the mean age of the female patients, it is expected that most of them were post-menopausal. It is possible that the differences between groups would be even greater if the female patients were younger, since young age was one of the main determinants of CINV.
In the latest version of the ESMO guidelines [31], the recommendations for CINV prevention due to high emetic chemotherapy based on anthracycline-cyclophosphamide (AC), were differentiated according to gender. In women treated with AC-based chemotherapy, a four-drug regimen including single doses of 5-HT3-RA, dexamethasone, NK1-RA, and olanzapine before chemotherapy is recommended to prevent acute CINV, and the addition of olanzapine to a triple antiemetic association on days 2–4 is suggested to prevent delayed nausea and vomiting. Similarly, for the prevention of acute CINV following oxaliplatin-based moderate chemotherapy, the addition of an NK1-RA before chemotherapy is suggested for women aged < 50 years old against a two-drug regimen (5-HT3-RA and DEX), recommended for the rest of patients receiving oxaliplatin [31]. These changes in treatment guidelines from international organizations such as ESMO highlight the increasing gender differences in CINV and the need for individualized approaches. In patients, especially women, with poor CINV control, different strategies can be employed, such as the addition of olanzapine, which has been shown to significantly improve CR rates as well as CINV prevention in chemotherapy-naive patients [32]. Other less-studied strategies have been using oral cannabinoids such as dronabinol and nabilone, which may have a role in controlling emesis from a neurophysiological perspective. Those drugs appear to offer a useful additional option, but further studies are still required to evaluate their efficacy and safety in the case of difficult-to-control CINV [33].
Other factors like habitual alcohol intake and habitual smoking have been described in previous studies to reduce the incidence of CINV [16, 24, 27, 34, 35]. In our study, only habitual smoking seemed to contribute to reducing CINV in the overall population, but only in the univariate analysis, like the study of Sekine et al. [16]. Another well-described factor is a history of pregnancy-related nausea and vomiting. In females, this factor has been associated with an increased risk of vomiting [35]. In our study, this factor was also found to increase the risk of CINV, although only in the univariate analysis.
Personal predisposing factors such as sex, age, habitual smoking, and history of pregnancy-related nausea and vomiting seem to be the main contributors to CINV in our study. The emetic potential of chemotherapy seems not to play such an important role, unlike what has been reported in previous studies and current antiemetic guidelines [8, 11, 13]. In fact, in our study, as the emetic potential of the chemotherapy regimen increased, the risk of CINV lowered; OR moderate emetic risk 0.15 (0.04–0.57), OR high emetic risk 0.46 (0.21–1.01). These data suggest that it is possible to predict in advance that patients are at high risk of CINV to adjust their antiemetic prophylaxis and that patients with a low emetic risk chemotherapy are not well protected against CINV. In addition, it was observed that approximately half of the patients who experienced CINV did so in more than one cycle, which further highlights the importance of personal predisposing factors in CINV. It is therefore important that the antiemetic regimen considers predisposing risk factors beyond the emetic risk of the chemotherapy scheme [6, 7, 16, 24, 28]. This might help to select high-risk patients for whom more potent antiemetic regimens should be prescribed and the selection of low-risk patients for whom expensive antiemetics are unlikely to be helpful and can cause them some adverse effects [35]. Different scores have been developed to accurately identify patients at high risk for CINV [36,37,38].
Our study recorded the incidence of the adverse effects most described in the prescribing information of the antiemetics used for chemotherapy prophylaxis. Constipation was the most reported adverse effect in both groups, being significantly the incidence being higher in females (52.4%) than in males (37.2%). Other common adverse effects reported by patients were tiredness, generalized pain, malaise, and diarrhea. Nevertheless, it remains uncertain whether these adverse effects stem solely from the administration of antiemetic agents or if they are influenced by the concurrent effects of chemotherapy. It is plausible that the interplay between chemotherapy and the patient’s psychological state of anxiety contributes to the exacerbation of adverse effects attributed to antiemetic drugs.
Our research provides valuable information on how to manage CINV according to sex, allowing early identification of patients at higher risk and individualizing antiemetic prophylaxis according to patient characteristics to reduce the incidence of antiemetic adverse effects. Nevertheless, several limitations must be acknowledged when interpreting these results. First, the data came from a single center. Hence, the findings might not apply to other settings owing to the center effect. Second, the study was non-randomized. Patients were divided into groups according to sex. The groups were balanced, although the male group was slightly larger than the female group. Third, numerous potential risk factors have been identified in the literature, some of which have been difficult to quantify for this study. Some of these factors may play a role in the observed outcomes. Biomarkers for CINV and the genetic and molecular mechanisms were not explored. It will be worthwhile to assess those factors in the future. Fourth, our study included a small percentage of patients who had already received other lines of treatment and for whom it was not registered whether they had previously suffered CINV. A history of experiencing CINV in prior treatment lines may predispose individuals to CINV in the current course of treatment. Nevertheless, that group only represented 4.3% of males and 19.6% of females. Additional multicentric studies in larger populations are needed to confirm our results and to develop more individualized regimens based on each patient’s risk according to sex. Based on our results, it would be interesting to evaluate in future studies whether men might require less potent antiemetic prophylaxis despite taking highly emetic chemotherapy. It would also be beneficial to focus on pharmacogenetics studies to investigate the role of genetic variants in selecting appropriate genetic risk factors for tailored emetic prophylaxis in clinical practice.



Comments (0)