In this study, the final diagnosis was reached in 85.0% of the TBLC and 63.1% of TBLB. Contrast with TBLC, the comparatively small biopsy specimen is the main restriction of TBLB in the histopathologic diagnosis of suspected ILD. According to the published expert statement, TBLC procedure which needed flexible bronchoscopy and an endobronchial balloon was performed under general anesthesia [12]. In the current study, there were no severe procedure-associated complications requiring further aggressive measures, with rates of bleeding (none or mild bleeding 86.6%, moderate bleeding 13.4%, severe bleeding 0%) and pneumothorax (14.4%), which was similar to previous reports [13,14,15].
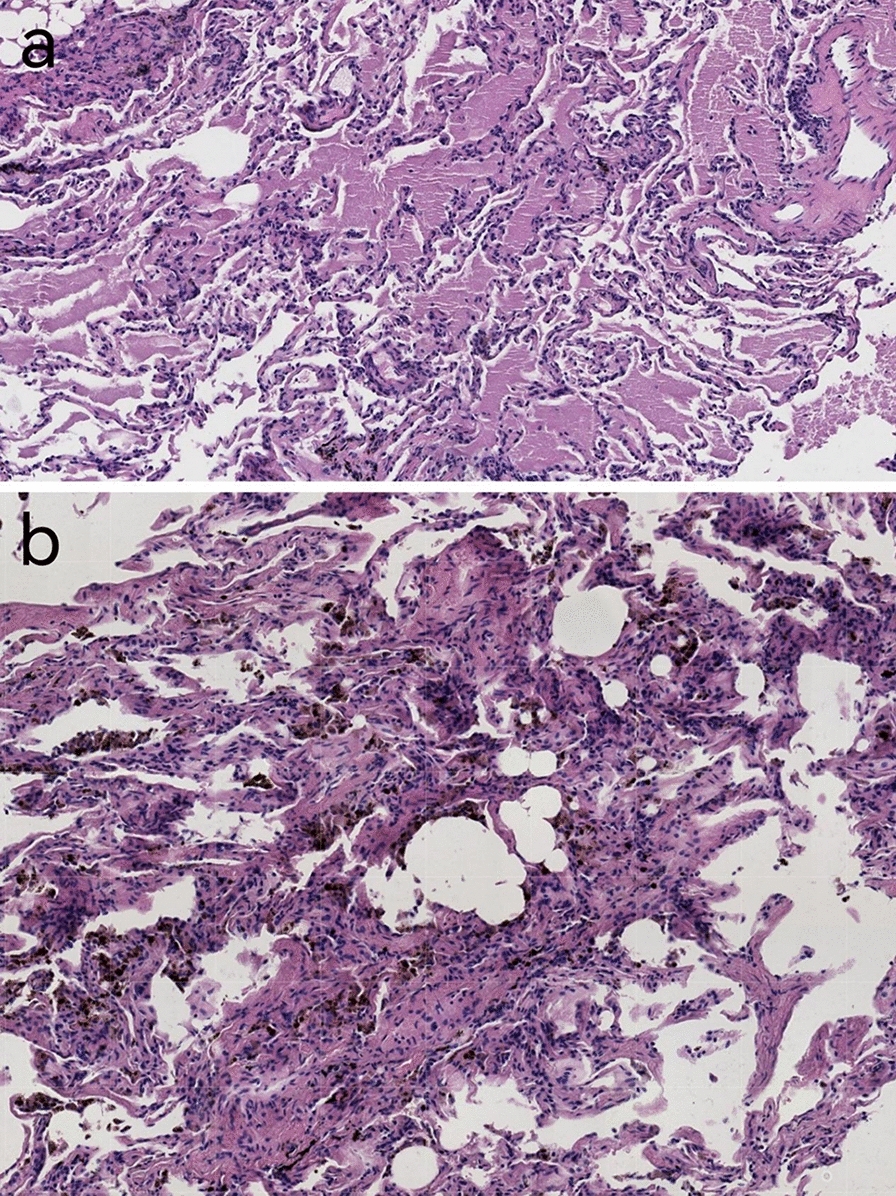
Histopathologic specimens were critical in the diagnosis of ILD. Although international guidelines propose that SLB is still the standard method to obtain biopsy tissue if the compounding of the clinical features and HRCT patterns cannot determine a specific diagnosis [10], clinicians still chose the clinical use of TBLC, with the advantages of lower invasiveness than SLB, shorter hospitalisation stay, less mortality, and lower cost. TBLC is a novel technique which could obtain suitable biopsy specimen for ILD diagnosis [16]. Although pathological diagnostic yield is one measure of biopsy efficacy, more direct measures should be considered when compared between different biopsy techniques, including accessing biopsy specimen adequacy and biopsy specimen with a definite histological pattern. TBLC can obtain biopsy specimens with the size of almost 10–30 mm2 that is enough large to recognize the pattern of lung lobules [17]. In a study by Ravaglia et al., TBLC has been reported to have a diagnostic yield of 87.8% among 699 patients from a high-volume and experienced center [18]. In this study, a pathological diagnosis was reached in 85.0% consistent with the literature report. Moreover, it is noteworthy that the most common final diagnoses were hypersensitivity pneumonitis (HP) and welder’s pneumoconiosis in this study. Previous studies had noted that TBLC provided larger biopsy specimens than TBLB and, therefore, might improve the diagnostic yield of pathological diagnosis of HP [19, 20]. However, the ATS/JRS/ALAT clinical practice guideline for HP suggests that pathology findings should refer to biopsy specimens obtaining from SLB, but do not consider whether this is equally applicable to TBLC [21].
Possible factors for diagnostic yield and complications of TBLC include number of biopsy specimens and biopsy location, probe size, freezing time, guidance of fluoroscopy, approach of anesthesia, and flexible or rigid bronchoscopy. Compared with 1.9 mm size of probe, a larger probe size of 2.4 mm could have greater diagnostic yield but a higher rate of pneumothorax (2.7% vs. 21.2%)[18]. In 2018, an expert statement recommended that a frozen time of 7 s with a 1.9 mm size of probe were suitable when performed the procedure of TBLC [12]. In our cohort, a 1.9 mm size of probe was used with a mean frozen time of 3–6 s, using carbon dioxide as the cryogen. Moreover, the cryoprobe was been inserted to a suitable placement away from the pleura with the guidance of fluoroscopy was considered to be a critical factor which minimized procedure-associated complications including pneumothorax and bleeding. Dhooria et al. reported that the occurrence of pneumothorax was significantly higher in patients who were performed the TBLC procedure without the guidance of fluoroscopy contrast with those with using fluoroscopy (20.9% and 5.9%, P = 0.01) among 128 ILD patients [22]. In addition, it has been reported the occurrence of moderate to severe bleeding was definitely higher in patients who were preformed TBLC procedure without prophylactic endobronchial balloon placement than those with prophylactic endobronchial balloon placement(35.7% and 1.8%, P < 0.001) [22]. In the present study, we used fluoroscopy and endobronchial balloon blocker in all patients based on the standardized protocol.
Bleeding and pneumothorax was the most common complication after TBLC. The occurrences of procedure-associated complications including bleeding and pneumothorax were considered acceptable (4.9% and 9.5%, comparatively) [8]. However, the range of substantial bleeding was reported to be wide, with the range of 0.3–26.6% in meta-analyses of TBLC procedures [15, 19]. The difference may be associated with the lack of a prophylactic balloon placement in a number of studies. In the present study, there were none patients who had severe hemorrhage after transbronchial cryobiopsy. We encountered moderate bleeding in 25 patients (13.4%), which required to be immediately treated by endoscopic measures. Pneumothorax was observed in 27 patients (14.4%), consistent with previous reports [23,24,25].
A previous study indicated that the rate of procedure-associated complications was modest in terms of experienced operators [6]. According to a survey which was investigate the procedure of TBLC, most of TBLC practice training (43%) was completed by self-training, other TBLC training was completed by fellowship training and practice course [26]. A standard TBLC training course which was performed by an experienced center was considered to be an important role in starting TBLC, with the advantages of convenience and ease of accessibility. With less procedure-associated complications including bleeding and pneumothorax, patients who underwent TBLC had a shorter hospital stay and better cost-effectiveness profile, making TBLC technique growing attractive in clinical procedures.
This study has several limitations. First of all, this is a retrospective and cross-sectional study conducted in a single center with a small study cohort. Second, final diagnoses were not always made within a MDD team. Further studies are needed to prove the diagnostic accuracy of TBLC by definite diagnosis with a more experienced MDD team.



Comments (0)