Our study is the first to show that concomitant therapy with ticagrelor is associated with increased blood concentrations of rosuvastatin compared with prasugrel or clopidogrel, whether analyzed separately or as a group. The association remained significant after adjusting for other potential predictors of rosuvastatin concentration such as age, sex, and renal or liver function. Our results provide important information on the concomitant guideline-directed administration of statins and P2Y12 antagonists. On one hand, our findings may explain recent reports of adverse rosuvastatin-related effects in patients on concomitant ticagrelor therapy [2, 10,11,12,13,14,15,16,17,18, 20, 21]. After a focused analysis of 2464 reports of rhabdomyolysis in patients treated with statins and antiplatelet drugs, an increase in rhabdomyolysis was observed when rosuvastatin and ticagrelor were co-administered. However, no difference was found when rosuvastatin was administered alone or co-administered with aspirin, clopidogrel, or prasugrel [22], which aligns with our results. On the other hand, research into the differences in cardiovascular outcomes between different P2Y12 regimens may benefit from further focusing on co-administration of specific statin therapies.
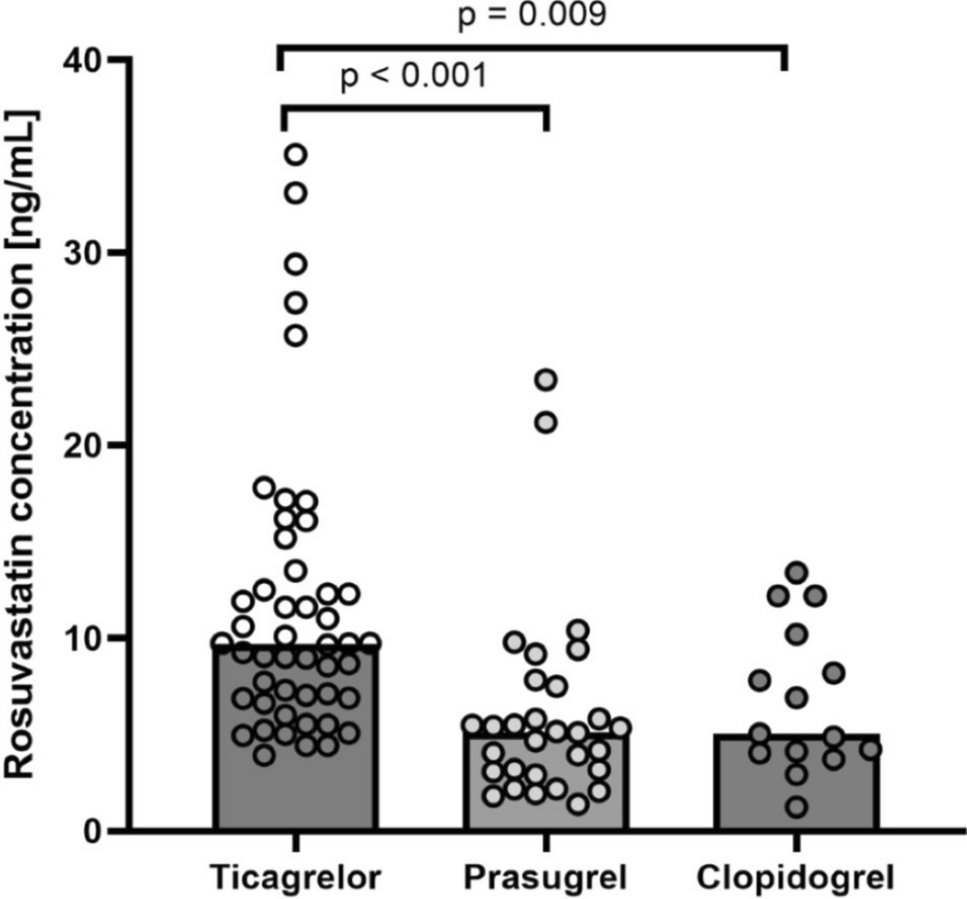
In our study, patients on ticagrelor had approximately two-fold higher trough plasma rosuvastatin concentrations than patients on either prasugrel or clopidogrel. Given the small group of patients on clopidogrel, we also performed a sensitivity analysis comparing patients on ticagrelor and those on non-ticagrelor therapy. The results remained consistent, further confirming the robustness of the results. Our results are in line with observations in healthy individuals, wherein peak rosuvastatin concentrations after a single dose of 10 mg was 2.6 times higher in participants taking ticagrelor than in those taking placebo [23]. Conversely, expected interactions with clopidogrel are smaller in magnitude (a 1.4-fold increase in the area under the plasma concentration-time curve of rosuvastatin was reported when administered concomitantly with clopidogrel 75 mg/day) [24], whereas no pharmacokinetic rosuvastatin–prasugrel interactions have been reported to date.
Possible mechanisms of rosuvastatin–ticagrelor pharmacokinetic interactions are more likely to involve transport mechanisms than metabolic enzymes [5, 25]. Rosuvastatin undergoes minimal metabolism by CYP2C9 and CYP2C19 and almost none by CYP3A4. It is primarily excreted through hepatic transporters, exhibiting high affinity to solute carrier organic anion transporter 1B1 and is also transported by adenosine triphosphate-binding cassette (ABC) transporters, such as ABCG2, ABCC2, and ABCB1, which supports its excretion via the bile. A static drug–drug interaction model predicted a 2.1-fold increase in rosuvastatin concentrations due to inhibition of ABCG2 by ticagrelor, whereas solute carrier organic anion transporter-mediated hepatic uptake of rosuvastatin should be unaffected because of the relatively low ticagrelor concentrations in the portal vein [2]. This inhibition was corroborated by similar effects observed with fostamatinib and febuxostat, where ABCG2 inhibition led to an approximately two-fold increase in rosuvastatin exposure [26, 27]. There are no pharmacokinetic studies describing how prasugrel affects rosuvastatin concentrations or ABCG2 function. Higher rosuvastatin concentrations observed in the ticagrelor group in our study could be explained by the extent of inhibition of ABCG2, as clopidogrel is expected to have a smaller effect on rosuvastatin concentrations. ABCG2 is a key transport protein involved in mediating rosuvastatin efflux in the small intestine [2]. Polymorphisms in the ABCG2 gene have been linked to increased rosuvastatin plasma concentrations [28, 29], supporting the hypothesis that ticagrelor’s inhibition of ABCG2 contributes to the elevated rosuvastatin levels observed in our study.
Other determinants of rosuvastatin concentrations were increasing age, renal function, ALT and LDH activity, and concomitant therapy with ezetimibe and/or potentially also valsartan. As expected, renal function—an important determinant of rosuvastatin clearance [30]—was an independent predictor of rosuvastatin concentration regardless of ticagrelor therapy. Although age has been identified as an important factor in the occurrence of rhabdomyolysis, particularly in patients aged ≥ 75 years [31], our exploratory analysis did not find an association between age and rosuvastatin concentrations after multivariate analysis; however, it is noteworthy that our patient population primarily comprised patients who had experienced MI at < 75 years. When comparing rosuvastatin concentrations in patients on ticagrelor aged < 65 years with those > 65 years, no statistical difference was observed, which could be due to the low number of patients (N = 10) in the group aged > 65 years. During the analysis of group comparisons, we also observed that patients receiving ticagrelor and prasugrel had slightly elevated ALT levels, an incidental finding also reported by others [32, 33]. Given a distinct effect of P2Y12 inhibitors on ALT levels and the potential interaction between liver function and rosuvastatin concentration, we adjusted our results for ALT in the multivariate model to minimize a potential confounding effect. Nonetheless, this hypothesis should be further validated in a larger cohort. Conversely, ALT and LDH were only associated with rosuvastatin concentration in the univariate model. Statin therapy increases liver enzyme activity by 0.5–2% [6], so a correlation with rosuvastatin concentration is an expected finding. Conversely, rosuvastatin concentrations were lower in patients on concomitant therapy with ezetimibe and/or valsartan but not when angiotensin II receptor blockers were analyzed as a combined group. Although the rosuvastatin–ezetimibe interaction was not significant after multivariate adjustment, valsartan emerged as a potential independent predictor of lower rosuvastatin concentrations. Previous studies have already reported non-significantly lower rosuvastatin concentrations in healthy volunteers taking valsartan [34, 35]. However, our patients were receiving higher doses of rosuvastatin, which may influence the observed effect. More importantly, given the very small number of patients on valsartan in our study, this finding should be regarded as hypothesis generating but merits further exploration in future studies.
Our study has some limitations. First, this was an observational study to compare rosuvastatin concentrations between patients taking different P2Y12 receptor antagonists, which precludes adjustment for unmeasured confounders. Second, we only performed a single sample measurement of rosuvastatin concentration, which precludes time-dependent analysis and may lead to a bias due to sampling errors or biological variability. Additionally, the number of patients was too small to draw definitive conclusions regarding the comparison of statin intolerance between the groups. Moreover, the groups were not completely homogeneous in terms of medication use, although this is unlikely to have had a significant impact on the results. The strength of our study is that it was a homogenous real-life patient population treated in accordance with the international guidelines.
Nonetheless, our study has shown that rosuvastatin concentrations are higher in patients on concomitant therapy with ticagrelor than in those receiving prasugrel or clopidogrel. The association is significant, independent of other potential determinants of rosuvastatin concentrations, and may be clinically relevant. Possible interactions between ticagrelor and rosuvastatin should be taken into account in the clinical setting, as both medications are commonly recommended together as part of guideline-directed therapy in patients after MI.

Comments (0)