Acute aortic dissection is an extremely severe cardiovascular disease [1]. Its exact pathogenesis is not yet fully understood. Studies have suggest that hypoxia and inflammation play crucial roles in the formation and progression of aortic dissection [4, 5]. Studies reported that hypoxic environments or HIF-1α not only significantly increase the concentration of macrophages expressing IL-6 around blood vessels, but also induce macrophage proliferation and migration, promote the survival of inflammatory cells, and enhance the inflammatory response, with evidence suggesting that HIF-1α is associated with the IL-6/STAT3 pathway [11,12,13].
Macrophages can undergo metabolic reprogramming via the HIF-1α-ADAM17 pathway, facilitating vascular inflammation, extracellular matrix degradation, and elastic lamina rupture, thereby exacerbating the development of aortic dissection [14]. The onset of aortic dissection is accompanied by a marked rise in both the quantity and proportion of synthetic smooth muscle cells, leading to diminished aortic elasticity and subsequent vessel wall rupture [15,16,17]. Research suggests that hypoxia-induced HIF-1α may mediate smooth muscle cell phenotype switching via the PI3K/AKT pathway, suppressing proliferation and migration capacities through downregulation of AEG-1 expression [18]. In murine models of aortic dissection, elevated HIF-1α levels are observed in aortic smooth muscle tissues. HIF-1α is implicated in regulating macrophage autophagy in type A aortic dissections and fostering hypoxia-driven proliferation and migration of vascular smooth muscle cells (VSMCs). Under hypoxic conditions, the deletion of HIF-1α has been shown to diminish VSMC proliferation and migration capabilities [19].
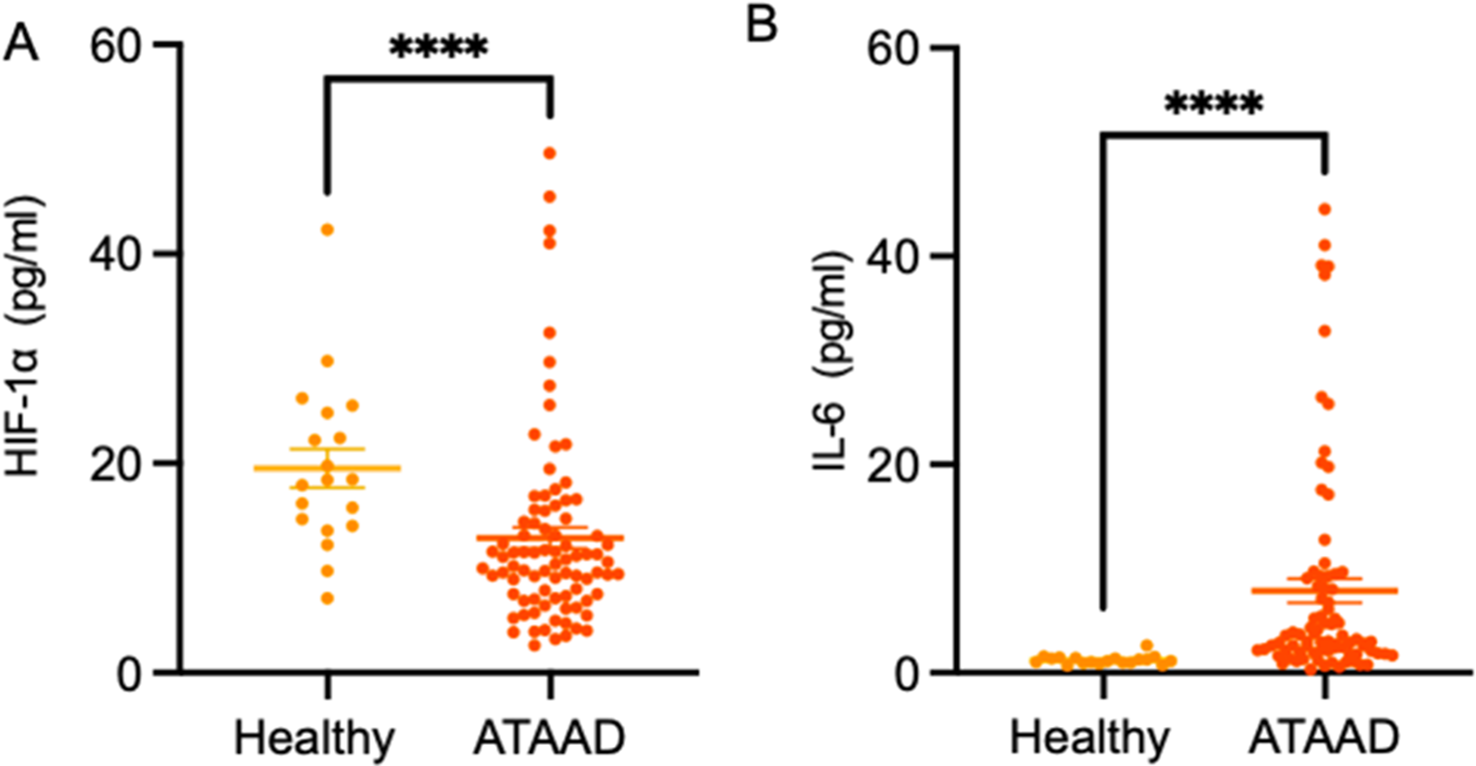
In this study, Spearman ’s correlation analysis showed a positive correlation between HIF-1α and IL-6 serum levels, suggesting a correlation or interaction between these two factors. This is inconsistent with previous cellular pathway and histological studies. During hypoxia, HIF-1α increases and affects gene expression related to hypoxia adaptation and IL-6 expression. Both are associated with inflammatory response and vascular endothelial function [20, 21]. The positive correlation between HIF-1α and IL-6 in acute aortic dissection suggests that they may jointly promote disease progression. This provides new clues for future directions and treatment strategies.
However, our research found that the expression of HIF-1α in human blood samples from patients with type A aortic dissections is lower than that in healthy individuals. This may due to several possibilities as list below:
1.
Acute hypoxia strongly induces the expression of HIF-1α. In the study of hypoxia adaptation in injured epithelia, exposure to chronic hypoxia environments similar to wound microenvironments leads to a decrease in the level of mTOR (mammalian target of rapamycin), which in turn leads to a decrease in HIF-1α levels [22]. The occurrence of acute aortic dissection may also be related to chronic hypoxia. In clinical work, we also find that some AD patients are obesity, they are suffering from obstructive sleep apnea syndrome (OSAS) and are in a state of hypoxia for a long time. This also indicates that they are in a statement of chronic hypoxia. We know that HIF-1α is an easy degradation factor under non-hypoxic environment. All of the AD patients are given oxygen therapy as soon as they are on the way to the hospital when they are in the ambulance. Even if some patients are not sent by ambulance, they are also given oxygen therapy as soon as admission. The hypoxic environment will be changed and the HIF-1α is degradated. In this case, the serum level of HIF-1α may be down-regulated [23,24,25].
2.
It has been reported that high levels of HIF-1α expression were observed in tissue samples of acute aortic dissection, while we observed low levels of HIF-1α in serum [26]. This difference may be due to the different distribution and mechanism of action of HIF-1α inside and outside the cell. Because HIF-1α mainly functions as a transcription factor in the nucleus, when aortic dissection occurs, HIF-1α needs to enter the nucleus to bind to the HRE (hypoxia response element) in DNA to regulate the expression of downstream genes. Therefore, the release of HIF-1α outside the cell will be correspondingly reduced.
3.
In aortic dissection, there may be other biological molecules that inhibit HIF-1α. These molecules can reduce its level through signal transduction pathways or directly interact with HIF-1α. The expression of HIF-1α is affected by multiple factors, including but not limited to IL-6. Even if the level of IL-6 increases, other regulatory factors may also lead to a decrease in HIF-1α expression. That can explain our result: although HIF-1α and IL-6 level in ATAAD patients were positively correlated, the serum IL-6 level were significantly increased while the serum HIF-1αlevel were significantly reduced.
4.
In ATAAD patients, HIF-1α expression levels exhibit distinct patterns across different stages of the disease, implicating stage-specific variations. Given the dynamic nature and progression of aortic dissection, HIF-1α expression is likely subject to temporal fluctuations throughout the course of the illness. Moreover, the observed discrepancies in serum HIF-1α levels can be attributed to interindividual variability and sample heterogeneity. The patient response to IL-6 and HIF-1α in the context of aortic dissection shows cell-type and tissue-dependent variability, introducing further complexity. This cellular heterogeneity may result in divergent expressions of HIF-1α within specific cell populations compared to the overall serum concentrations, highlighting the need for nuanced interpretations of HIF-1α’s role in the pathophysiology of aortic dissection.
Although animal models can provide useful preliminary data in many cases, there are significant species differences between the physiological systems of humans and rodent. Therefore, there are certain limitations in applying animal experimental results to humans due to species differences in the observed increase in HIF-1α levels in rodent models, and further clinical research is needed.
Due to the limitation of sample collection, the sample size of the measurement is small, and the research results of the experiment have certain limitations. We can increase the sample size in one step to reduce the relevant impact of the offset value. In our study, we only use ELISA to detect the levels of HIF-1α and IL-6 in serum, and can further verify the expression levels of both through retesting using immunofluorescence, Western blot analysis, and other methods.



Comments (0)