
Remember me
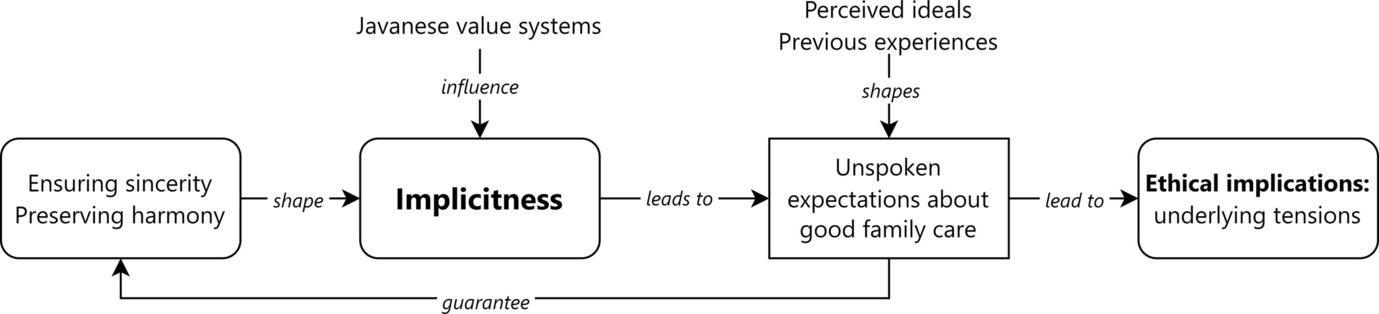
From the ethnographic data we found that implicitness influences expectations of how to provide good palliative care. Patients, family members, and health professionals had their own ideas of how a family should be involved in care. They had pre-existing ideas or conceptualizations of what constitutes good care and who provides or should provide that care. These ideas and concepts were also acknowledged by health professionals. In our findings, most of the expectations indeed remained unspoken, preventing them from becoming a request or demand.
There were variations in the degree or extent of explicit or implicit communication styles among family members, depending on each family’s communication style and cohesiveness, which we found was partly related to socio-economic status. For instance, one middle-income family in our sample that had previously lived in Jakarta and now resided near the center of Banyumas had more explicit communication between family members. Meanwhile, other families living in rural areas with lower incomes tended to have more implicit and unspoken communication. Despite differences in communication styles between families, we argue that to some extent there is always an element of implicitness in family exchanges.
We found two common unspoken expectations among families of palliative patients: that family members should be sincerely involved in daily caring activities and take the initiative in providing financial support.
Being Sincerely Involved in Daily Caring ActivitiesFamilies felt it was ideal when there was a daily, constant presence of a family member who could care for the patient, either at home or during appointments in health care facilities. The primary family caregivers are ‘on duty’ for almost 24 h since they are living together with the patients. The duties range from caring for the patient’s hygiene, nutrition, medication, and wounds. In a previous article (Wicaksono et al. 2024b) we provide more analysis of how patients’ family caregivers in Banyumas organize care at home for the patient, such as making an in-bed urine pipe installation and using traditional medicine.
Suyono, the husband of an elderly woman with chronic diabetes and a foot ulcer told us that caregiving is considered an “obligation”:
Interviewer: How do you provide hygiene care for your wife?
Suyono: I wipe her body twice a day, in the morning and in the afternoon here on the bed. I also change her clothes. Yes, I could not go anywhere, I have to be with her. (laughing). This is an obligation.
Interviewer: What kind of obligation is that, sir?
Suyono: It is an obligation for the husband, when the wife is sick, then he has to take care of her, in every single way. (FP03)
Here, the husband emphasized that it is an obligation for the spouse to provide care for the ill patient and be there for the patient. His wife never asked him to provide care and to be there for her, but he did it on his own initiative. This initiative-taking is a component of the notion of sincerity that we encountered in the fieldwork. Since providing care is physically and mentally demanding for the primary family caregiver, other family members are also expected to provide direct support, to take over the caregiving duty, even if temporarily. For instance, Suyono's daughter helped with washing the patient's hair and cooking food for the family. The sincerity here extends from being physically present to whole-heartedly catering to the patient and primary family caregiver’s physical and emotional needs, without expecting a return.
The notion and practice of sincerity was illustrated through the presence of the patient's spouse or the primary family caregiver's spouse. Their presence is important not only to help with physical caregiving activities, but also to give sincere support. They could understand each other’s capacity to do physical caring activities, even without a clear guideline on who will do what. This intuitive understanding came from long-term interactions between spouses or other family members, often requiring tinkering with caregiving roles and activities. In return, the patient would feel grateful and then pray to God for the goodness and well-being of the family members. This is shown in Mawar’s story, a patient with breast cancer:
Mawar: My husband washes my hair and body every day, with warm water. He is very determined. He may look ugly and old, but Alhamdulillah (praise Allah), early in the morning he cooks rice and food and asks me what I want to eat. He washes our clothes and works in the rice field. [...] I pray, “Dear Allah, give me health and long life; give mercy to my husband.” I feel sorry for my husband, he must be tired, and no one helped him. (P10-1)
This quote shows Mawar’s gratefulness for her husband’s sincere caregiving. He took care of her in every detail. Her husband did not refrain from showing his affection by crying and worrying about her condition. This led to a growing cohesion within Mawar’s family.
Not only are family caregivers expected by patients and health professionals to care for patients at home, they are also expected to accompany the patient for appointments at public health centers (Puskesmas) or hospitals. Health professionals expect families to accompany the patient during hospitalization. Some family caregivers showed their sincerity and full attention by accompanying patients to routine medical check-ups or appointments. However, there were other family caregivers who were not able to do so due to busyness at work, or who did not realize the importance of family involvement in these appointments. This meant that in some instances, patients were not able to attend routine check-ups because there was no one to escort them to the Puskesmas. At other times, family members just dropped the patient in front of the building and waited outside. Health professionals felt sorry for the patients, as the patients needed more guidance to follow the procedures inside the building, and because health professionals expected family caregivers to be there by the patient's side so as to also listen and subsequently better care for them.
Patients’ expectations that certain family members should be present could sometimes not be expressed explicitly, due to their fear of being a burden (membebani) or possibly creating discomfort (tidak enak, sungkan, rikuh). Health professionals might notice this implicit wish, for instance, if the patient is in hospital and their appetite changes. One of the doctors in our study, for instance, said that sometimes the patient eats better when a specific family member is present during hospitalization. Therefore, presence of family members in daily caring activities is an important expectation that sometimes remains implicit.
Taking the Initiative in Providing Financial SupportProviding financial support was an expectation that should be fulfilled, particularly by family members who are not directly caring for the patient. Providing financial support can therefore be seen as a form of partial substitution for a physical presence in caring. Since asking for financial support is considered sensitive and might be inappropriate to discuss openly, it mostly remained an implicit expectation. Family members are, therefore, expected to take the initiative to provide financial support without being asked.
Discomfort may come from expressing personal or private individual needs, such as the need for diapers. By taking the initiative to provide diapers for instance, family members could reduce the discomfort in explicitly discussing personal needs. Sri, a daughter of a bedridden patient with unoperated hip dislocation, told us about the support her family received from other family members:
Sri: Her grandchild took the initiative to buy diapers for her. We do this together. Her children living in other towns and other countries also help, sending some money. Everybody thinks together (regarding how to care for her). (FP06).
The ethnographer also observed a portable toilet device in the patient’s bedroom, which has been purchased by the patient’s daughter living overseas, possibly earning a higher income than Sri.
Mawar, the patient with breast cancer referred to above, spoke about the difference between her daughter and her son. Her daughter took the initiative to offer financial support when she needed to travel to the hospital by asking, “Mom, do you have some money to buy gas? Here is some pocket money for you, to buy gas or snacks.” Her son never showed this kind of initiative, which made Mawar sad.
Sugeng, a patient who had had a stroke and with a diabetic ulcer, had a more explicit approach, as he did not refrain from asking for money from his family members, neighbors, and colleagues. He said, jokingly, “aku njaluk duite” (a Javanese sentence meaning “I ask for your money”) to his old school friends. Sugeng admitted that he was not shy anymore in asking for help and openly admitted that he received donations and support. Sometimes, Sugeng also used social media to show his needs, such as for internet bundles, which were then followed by his friends sending him some money or buying him some food. The example of Sugeng’s explicit communication shows a deviation from the usual norm of implicit expectation. This financial support, explicitly requested, was an important form of assistance. However, because it was more explicitly requested, it could not be ensured that it comes from a sincere attention to care for the patient.
What makes implicitness a value?Expectations, wishes, or desires could not usually be simply made explicit due to the importance of the value of implicitness in family care. Implicitness is a value because it creates a way to ensure sincerity and maintain harmony. When a family member fails to act upon this value, they may be perceived by the patient, other family members, or health professionals as bad caregivers.
Ensuring SincerityThe value of implicitness aims to ensure sincerity by providing a way for people to take initiative in providing care, without being asked. We learned that keeping expectations implicit and not transforming them into requests or demands could be a test of sincerity. When family members accept an explicit request for help, it is difficult to know whether the help comes sincerely or not. There is a possibility that family members do it to avoid the discomfort of declining the request and to remain socially acceptable. On the contrary, if family members do something and contribute to care without explicit request, it is considered that their help truly comes from the heart. By not explicitly saying ‘what I need’ and ‘what to do’, the action taken by family members is felt to be genuine and sincere. When an act of care is done sincerely in this way, the care receiver will feel less like a burden. The importance of sincere affection is represented in Desi’s story, in which she emphasized the concept of gemati (a Javanese word meaning loving and caring sincerely (Supriyadi 2024). Desi is an elderly woman who took care of her adult bedridden son, who had suffered a severe stroke. The patient’s son, a young adult of around 20 years old, needed to be instructed by Desi to care for the patient:
Desi: I told him (the patient's son/Desi's grandson), “Whether you want to wash him or not, it's up to you! If I don't tell you, he won't get washed. How is this possible?”. I feel a little upset with him, why isn't he gemati at all?
Interviewer: What is gemati?
Desi: Love. He does not truly love his father, maybe only a glimpse of it. (F05)
She argued that when a person is gemati, he or she should not need any nudging or instruction to take care of loved ones. Desi told us that her grandson was not quick enough to understand the needs of his father, because he lacked sincerity. She preferred not to ask explicitly, because it would invalidate the sincerity of the action.
Maintaining HarmonyImplicitness also aims to maintain harmony by preventing arguments or conflicts and discomfort that can arise from discussing expectations explicitly. From previous cases, such as the quote from Sri, we learned that implicit expectations, such as expecting family members to buy diapers or to send money for the primary family caregivers without being asked, could avoid possible discomfort related to being vulnerable. The absence of discomfort may be considered to be a part of a state of harmony. Meanwhile, Dahlia’s case below provides an example of how explicit communication can lead to conflict and confrontation. Dahlia took care of her divorced father, who now had daughters from his new wife:
When Dahlia’s father was hospitalized in another city, she told her half-siblings that she and her husband had to go back and forth, perhaps almost 1600 km over the course of ten days of hospitalization. Her half-siblings openly accused her of making things up. “Is father really sick? Is this your agenda to ask for our money?” (FW16)
Although this is an extreme example, Dahlia’s case points out that explicitness may trigger conflict and uneasiness among family members. Dahlia and her husband were offended when they heard her half-siblings’ reaction. They hoped for some empathetic response such as “Thank you for accompanying our father”. The financial support, although it is also expected, was something they did not ask for. For Dahlia and her husband, it would have been better for Dahlia’s half-siblings to stay silent rather than to accuse them of making up stories.
Another example of implicitness being used to sustain harmony was shown by Nardi, a patient with paraplegia and a pressure ulcer, who refused assistance from the social worker to help solve family financial problems. He told us, “I did not want to make a fuss in the family.”
The above cases reveal the strong ideals and norms of sustaining harmony within the family, and avoiding arguments or conflict; maintaining harmony through keeping certain issues implicit is better appreciated, even if it sometimes means bad care for the patients.
The Ethical Implications of Being Implicit about ExpectationsIt is clear from our findings that implicitness plays a significant role in everyday palliative care situations within families. Implicitness as a value comes with good intentions and is seen or used as a form of care; however, it does not always result in positive outcomes. Implicitness by itself has the potential to lead to underlying tensions that are not addressed properly. These challenges could arise in the daily practices of family care.
When expectations remain implicit, it is possible that other family members cannot instinctively grasp the needs of care recipients or family caregivers. They do love and are concerned for the patient, but they genuinely do not know how to start helping. The patient and primary family caregiver refrain from asking for help due to the idea of maintaining sincerity and preserving harmony. This reflects a problematic double-bind emotional dilemma, first described by Bateson et al. (1956), leading to unmet needs for support. While making things explicit might not be good since it spoils sincerity and harmony, remaining implicit may also not be good and could lead to inadequate support or underlying and unresolved conflict.
It is also possible, however, that family members lack the sincere and attentive characteristics needed to provide care for a patient. After several unsuccessful attempts to ask for help explicitly, the patient or their main caregiver resorts to implicit communications, refraining from further request for help and keeping their struggles to themselves. This situation frequently occurred in response to relatively young male family members’ lack of care. Mawar, the patient with breast cancer, told us that she once explicitly asked her son for help with some money to go to the hospital. Her son did not respond at all. She felt deeply saddened by the lack of support from her son, and so decided that she would not ask him for any help again so as not to be disappointed. She still hoped for her son to be more attentive, but she could not complain because it would feel like she was giving instructions:
Mawar: I feel uncomfortable if I have to give “instruction”, for me it is not appropriate if the parents say these things (how to better care) to the children. If I need anything, I will wait until I or my husband can get it ourselves (P10-2).
Another example of unresolved tension due to implicitness and resulting unmet expectations can be found in Putra and Putri’s family who were caring for their elderly, bedridden mother with severe osteoarthritis and multiple morbidities. This is a lower-middle income family living in a rural area of the hills:
Interviewer: Have you ever told your other family about your needs?
Putra: No. Our principle is “not asking (for help) from anyone unless they give it sympathetically.” Even if I ask (for help) from my wife's older sister, I forbid her. Don’t ask. We must try ourselves.
Putri: Oh God, (actually) it would be nice if my sister asked “How is mother doing? What food does she eat? This is some money to help.” If that was the case, that would be very appropriate. (F07)
The quote shows the unmet implicit expectations of how family members should provide care despite not living together, such as showing attention by asking about the patient’s condition. The tone of Putri's sentence shows resentment toward her sister. It shows unresolved tensions between family caregivers living together with the patient and other family members living elsewhere. Moreover, this case emphasized how implicitness shaped the expectation of financial support, as illustrated by Putri, who expressed her expectation of her sibling to say, “This is some money to help.”
Melati’s story reveals how unresolved tensions could also occur between close family caregivers in the home. Melati is a mother of an adult child with cerebral palsy and severe ear infection. Although her husband cooperated very well in doing physical caregiving activities, Melati also expected him to provide emotional support:
Melati: I have never been able to talk and discuss things with my husband [...] Sometimes, it feels like two foreigners living together. When I tried to share my burden, he said: “You should not complain like that, this daughter has been given to us by God Almighty for a reason.” I know that is true, but I just want to tell my story. (F08)
This quote shows a very complex interplay between the different expectations of Melati and her husband. Expectations are not static and may shift, as illustrated by Melati who wanted to talk about difficulties, while her husband wanted to not complain about their difficulties. It could also show that Melati favors less implicit communication than her husband. These differences are not resolved and lead to dissatisfaction. By asking Melati not to talk about her burdens, Melati’s husband dismissed her emotional needs and undermined her struggle. The tension between them was also rooted in wider gender norms, extending to different opinions regarding Melati’s activity with her friends, her idea to return to college, and her parenting style. However, these tensions were not sorted out, due to Melati’s perception that a wife’s responsibility includes “following husband’s every word.” Therefore, her expectations for her husband to provide more sincere affection were not explicitly discussed and not resolved.
Strategies to Resolve the Problems of ImplicitnessThe ethnographic data revealed three common strategies among participants to address the problems arising from implicitness of expectations: for families to accept difficult circumstances, for families to share their difficulties with health professionals, and for health professionals to take the initiative in exploring further and acting sensitively.
Firstly, some caregivers, like Dahlia, chose to accept the circumstances and come to terms with some of their unmet desires:
Dahlia: Actually, I am physically tired. I want someone to take over (this caregiving role), but my siblings live far away, what can I do? I felt upset with them. Because I am here alone, no siblings live here in this town, so I have to accept that I do everything by myself. (FP01)
Since Dahlia’s siblings live in other cities, she had to come to terms with this circumstance and rely on her husband and children to support her physical caregiving duties. Fortunately, her siblings still could provide financial support by regularly sending money to help with caregiving costs.
Secondly, some families chose to share their problems with health professionals. Health professionals often become a venting outlet for patients or the primary family caregivers. As an external party, health professionals are sometimes considered a safe space to express more explicitly their expectations and concerns. When communicating among family members themselves, patients and families may fear adding more burdens or creating conflict. Health professionals, however, could have or hear conversations about these expectations, especially during prolonged exposure to the patient, such as during home care visits. For instance, family caregivers told Fony, their primary care physician, that they often felt unappreciated for their caregiving, while the patient only wanted to see other family members who are not there on a daily basis:
Fony: The primary family caregivers who are tired from taking care of the patient from A to Z, they are always blamed for everything. Meanwhile, the patient waits for visits from other family members, other children, who live far away. The primary family caregivers are more tired than those distant family members who only send money. I don’t know what to say. (FGD 2)
Nurses, particularly those who are involved in homecare services, can delve deeper into family conditions, observe family dynamics, and listen to the whole story. Yusuf, a homecare nurse, shared his experience of hearing different family members express dissatisfaction with each other's caregiving roles:
Yusuf: We never limit the duration of our homecare visits, to ensure care needs are fulfilled. For example, a female patient and her son (A) talk about another son (B) not providing enough money. The next visit, it's the other way around, with son (B) telling stories about his brother (A) not helping with hospital appointments. This happens frequently. (FGD 1)
Third, some health professionals tried to explore the situation further when noticing a lack of family presence and involvement in patient care. Some patients, due to the feeling of discomfort and the fear of becoming a burden, cannot explicitly express their wish to have their family members by their side and use “cryptic language codes” that require sensitivity from health professionals to fully understand what they mean. Dahlia and her husband told us they feel it might be inappropriate to share family problems with health professionals but would appreciate it if health professionals took a proactive approach in exploring these issues first.
Mala, a palliative care physician, shared her communication techniques with other health professionals, noting the importance of validating the concerns of family caregivers and offering to help facilitate communication:
Mala: When we hear patients’ and families’ stories, perhaps we feel confused and sad, but we can try to validate the feelings: “I understand what you feel right now, it must be difficult for you and the family. Let’s try to find the solution together. What do you expect from other family members? If you can’t say it directly, please feel free to tell it to us, perhaps we can be a bridge to communicate this with other family members”. (FGD 1)
Mala expressed that she herself is still learning how to communicate effectively, since every word choice she uses will influence the psychological well-being of the patient and family. To improve her communication skills and provide more holistic care, she emphasized the need to practice more frequently. One good example is Astrid, a Puskesmas nurse, who visited a patient’s home to uncover the patient's true wishes and the real challenge within her family.
Astrid: There was one patient who did not attend her medical appointments. She told us she was busy selling snacks at the local market every morning. When we visited her home, she looked so happy and excited. It turned out she wasn't selling snacks at the market but was actually staying at home. She had an adult son who was also at home and pretended to sleep when we arrived. We realized that she wanted to come to the Puskesmas, but she couldn't ask her son to take her there, so she came up with the “market” excuse. (FGD 2)
Astrid’s visit turned out to be an important moment for the family. Although she did not directly communicate with the son about caregiving, she explained and emphasized to the patient the importance of routine check-ups in a way that meant the son could also hear this too. Her visit eventually inspired the patient’s son to improve as a caregiver. In the next home visit, Astrid learned that the patient was routinely attending the hospital appointments accompanied by her son. Another patient asked the Puskesmas doctor to emphasize to her, when her son was sitting next to her in the consultation, that “You must come routinely for medical check-ups”, hoping that the doctor's advice would motivate the son to help more without directly telling him what to do.
Health professionals also often felt less able to help after exploring patients’ and families’ difficulties, particularly when problems were related to the patient’s economic circumstances. One homecare nurse said, “Of course I am confused. If the conflict is finance-related, what can we do anyway?”. The head of a Puskesmas expressed, “It is our duty to care, but if we have to think about their economic condition, we give up, this is the scope of someone else.” One possibility to solve this problem according to the focus group discussion in our study would be to connect the patient and the family caregivers with available resources, such as institutional and regional social funds, or external philanthropy organizations.
Comments (0)