
Remember me



Four themes were identified across the interviews: (1) current awareness of genetics, (2) consanguinity, religion and cultural influence, (3) presenting genetics information in a new digital resource and (4) dissemination, information-sharing and uptake.
Theme 1. Current awareness of geneticsWhen explaining genetics, participants identified traits that their children had inherited from one parent (e.g., being flat-footed, wearing glasses or hearing loss). When questioned regarding how to explain genetics to family members, participants suggested making models out of Play-Doh or using diagrams or analogies related to cooking, prayer beads, building and making a cup of tea.
Like making a cup of tea, the slight variation of the milk… it makes a difference.
It was emphasised that it’s not about how the information is relayed but who is presenting the information that is important, as community members are more likely to trust people they know and respect.
I think it’s a cultural issue…I think people are more likely to trust someone that they know in their own community.
Participants were reflective of how they would explain genetics to elders in the community, suggesting that they play an important role in medical decision-making. In this regard, multiple interrelated barriers to explaining genetics were identified, including language, education, and health literacy and that many words (e.g., genes) do not directly translate to Urdu nor are commonly understood.
From a Pakistani community, our elders don’t always understand the genetics condition. They just think it’s abimariandbimarijust means an illness that will go away or will be treated with a bit of paracetamol.
Theme 2. Consanguinity, religion and cultural influenceOnly one participant was aware of consanguinity as a terminology. However, everyone was aware of cousin marriages, although there were many different interpretations. These ranged from cousin marriages being directly associated with arranged marriages, being only limited to first or second cousins or any extended relative of the “same blood.”
Participants had some level of understanding about cousin marriages, but most of them had different interpretations, which were necessarily not correct.
….everybody said, oh, what rubbish she’s talking, like cousin marriage has been happening since our Prophet’s time, it’s not a valid reason to break an engagement with your uncle’s son, like it’s a family thing, you can’t do that on just a very silly assumption that this can happen.
As participants described, women are perceived to be responsible for passing down a genetic condition in their community. Therefore, it reduces women’s marriage prospects hugely. One of the participants described how:
In a community where girls are being rejected on the basis of their colour and their height, bringing this into the picture will make it more difficult, I think, where you are rejecting people on the basis of, okay, they have got this kind of disease in the family so it’s a big no.
Theme 3. Presenting genetics information in a new digital resourceParticipants had requests related to the written information, language, including engaging visuals and embedding trust (using NHS branding) and featuring patient stories (see Table 1).
Table 1 Requirements for the new app presented as sub-themes with supporting quotes (presented in italics)Theme 4. Dissemination, sharing and uptake of genetics-related informationParticipants discussed that linking the app with existing services and community groups would widen uptake, as people are unlikely to think about genetic conditions until they are affected. A participant explained that much more marketing would need to happen if the app was standalone, given that there are “millions of apps” on the app stores.
There were many suggestions for how the app may be disseminated to young people, including sharing it on Facebook groups, YouTube and Instagram, using a distinct hashtag: If you’re really trying to get the younger generation, you might start a campaign, a hashtag, and try to promote it with maybe famous bloggers, things like that.
To engage the community more broadly, participants suggested using influencers and high-profile community members to promote the app and also sharing it on community social media groups (e.g., from mosques), at bus stops and in local children’s centres and on marriage or Muslim dating websites. Healthcare workers and settings were also identified as potential avenues for dissemination. For example, via midwives, distributing leaflets at GP clinics, on the NHS website or placing posters in waiting areas of hospitals and pharmacies.
It was emphasised that in-person communication and word-of-mouth were extremely important in the community. This was also important for people who do not speak English confidently or who may not respond to leaflets. Participants suggested that community events (e.g., health seminars) or engaging people while waiting at the doctor’s surgery could be an appropriate way to engage the community and answer any questions.
I strongly believe that it has to be face-to-face communication in terms of maybe health seminars, awareness events that are going on within the local community. I don’t think it’s something that if it was posted through the door or a leaflet, that they would actually take the time to sit down and read it.
Participants also explained that despite initially using the app alone, they would share the information with their partners and family members, especially if it was serious (e.g., recommended seeing a GP). One participant explained that information-sharing in families was normal due to the fact that many people “don’t have the privacy of their own phone.” Others explained that they simply like to share relevant information.
I’d probably use it myself first. I’d get to see the information. And then I would pick my targets, which I normally do, would be my sister-in-laws, who have got children of marriageable age, and then I’d be saying, have you seen this, I’ll send you the link, why don’t you download it, have a look in your own time. Or I’d say, you know, click on that, and just see that video about that family and what happened to them and how it impacted and the things they had to go through and…we might look at it together.
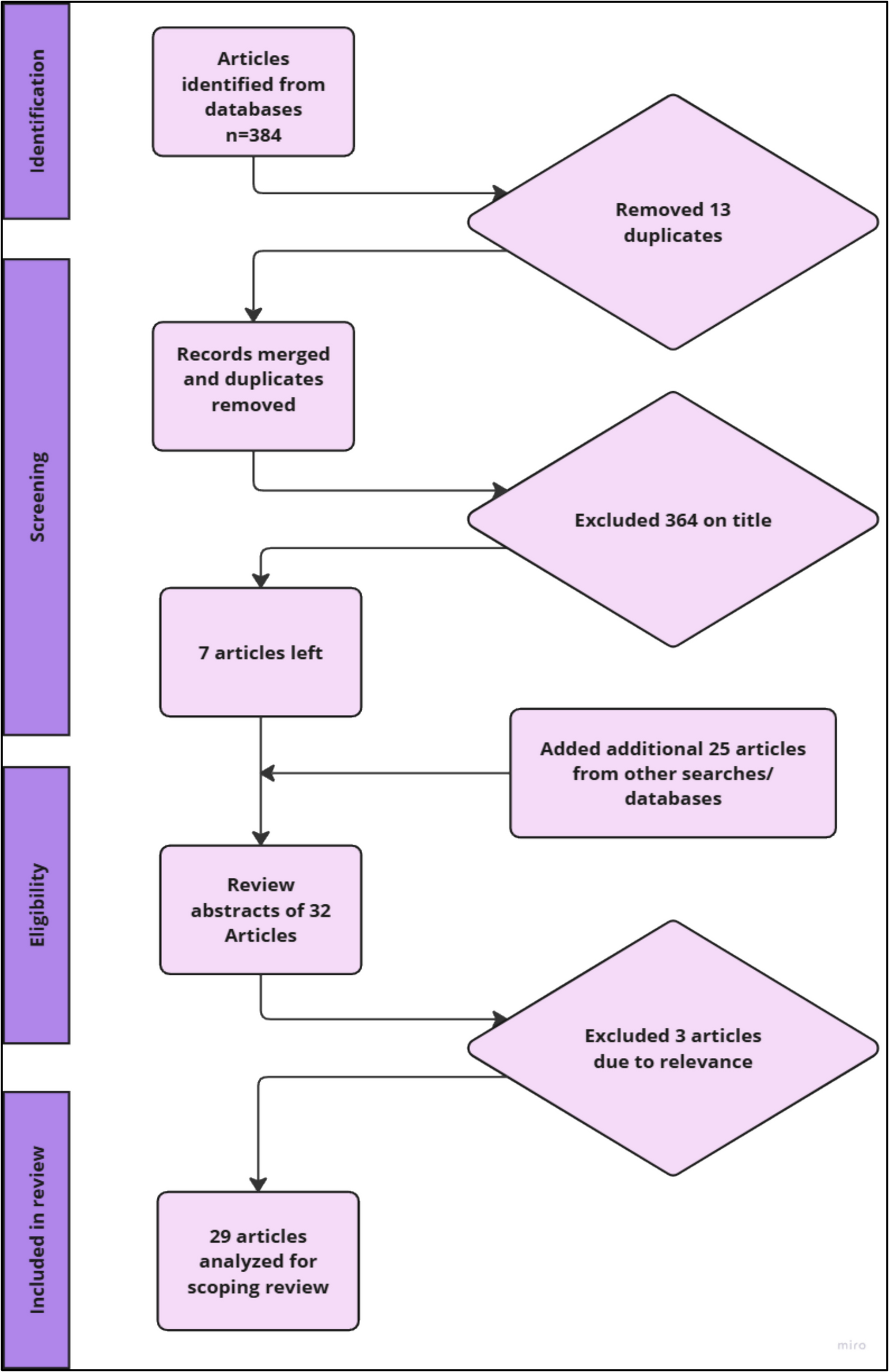
Phase 2. Scoping existing digital resourcesIn the systematic review of the content, functionality, and quality of patient-facing genetic and genomic mobile apps available in the UK we identified 22 relevant apps that were aimed at educating users [24]. There were many more apps available from the two UK app stores (n = 731), but the two stages of screening highlighted that most did not meet the eligibility criteria for myriad reasons, including those that relied on DNA sampling, not being patient-facing, not focussing on genetic conditions, or not being in English. Of the 22 apps that were reviewed, half did not meet the minimum acceptability criteria (quality), only three were affiliated with a registered charity or healthcare body, and none had been formally trialled or tested. This emphasises the need for a culturally sensitive, accessible, evidence-based app to be developed aimed at improving genetic literacy within specific communities.
In our systematic review of digital interventions for genomics and genetic education, empowerment, and service engagement, we explored existing patient-facing digital technologies [25]. Twenty-four studies were included, of which twenty-one were deemed moderate or high quality. Most (88%) were carried out in America, the majority (79%) were conducted within a clinical setting, more than half (63%) of the interventions were web-based tools, and almost all (92%) focussed on educating users. However, few of the studies were aimed at improving the empowerment of patients or were community-based, and none targeted the Pakistani community, thus highlighting the need for future work to focus on co-developing content with end users.
Phase 3. Prototype development and testingThemes presenting the requirements for the app included features, accessibility, design, content, quality and security. These were prioritised by the app development team (Table 2).
Table 2 Prioritisation of captured requirements using MoSCoW (Must have = M, should have = S, could have = C, won’t have this time = W)Initial paper prototypes were then developed through a series of workshops with subject matter experts during the COVID-19 pandemic (Fig. 2), including a colleague with expertise in design thinking. Based on the interviews with participants, the group first established the content that the app would need to cover, including:
What are genes?
What are genetic conditions?
Why are genetic conditions more common in the Pakistani community?
What does autosomal recessive mean?
What are the risks?
How can I get more information?
When should I consider a genetic test?
What is genetic testing?
What happens when you get your results?
Fig. 2
Various paper prototypes generated during the initial design session with subject matter experts and ordered by narrative
The findings discussed by the group following the paper prototyping approach are presented in Table 3.
Table 3 Itemised content and format used in the appAnimations were designed by a professional design company (Niftyfox), following extensive storyboarding of the concepts with the project team. The storyboards were reviewed by two of the original participants during a face-to-face feedback session with the project team and the animation company. Areas that were flagged included skin colour of animated characters, clothing, analogies used and also representation of both male and female in each animation to ensure it was clear that a recessive genetic condition was inherited from both parents. Further iterations of the storyboards were made according to the feedback received during this session.
Video content was produced by the in-house media services team at The University of Manchester, scripts were written by the project team, including a genetic counsellor to ensure their authenticity. Actors were used to portray the clinicians and patients in the videos and were purposefully selected to ensure they had the right ethnicity. One of the actors could also speak Urdu, which enabled us to capture the voiceover of the videos in Urdu.
Prototypes were then further developed into a high-fidelity digital prototype in the form of an Ionic mobile app. The separately designed animations and video content were also added to the app (see Fig. 3).
Fig. 3
Screenshots of the application showing (from left to right) the home screen, main menu, animation content, glossary and videos of mock clinic consultations
Two female participants reviewed the content and proposed some changes which were discussed by the team and prioritised using the MoSCoW method (see Table 4).
Table 4 Proposed changes and issues Raised with MoSCoW prioritisationPhase 4. In-person feedback session and app refinementFive community members tested the app for usability and acceptability. We also explored their responses to the data collection methods.
UsabilityThe mean SUS score was 87 (SD: 10.95; range: 72.5–97.5), indicating excellent usability. No challenges in using the app were observed. However, three participants initially chose to watch the videos together and read the written content individually.
Participants found moving between screens easy (Mean: 4.6; SD: 0.55; range 4–5). They also found it easy to learn to use the app (Mean: 4.4; SD: 0.89; range 3–5). They explained:
It was easy to use the app. The app flowed from one section to the next. (P1)
Everyone knows how to use a device and how to use an app, as long as they know how to read the language. It was easy to navigate through the app. (P5)
AcceptabilityAcceptability data is presented in Table 5. The written information, animations, videos and content were acceptable to participants. Survey scores were lower for the items ‘the written information was comprehensive and concise’ and ‘the content could be improved’ indicating that the app could be improved. Participants suggested more use of videos, simplifying the language used (avoiding jargon and medical terms), translating the app into other languages (especially Urdu) and adding other content, like links to support groups and written testimonials from patients who have used a genetics service. Participants also wanted more information on what to do next, including charities they could link with or a ‘communication box’ where they could send a message to someone who can direct them to services or resources.
Importantly, participants tended to trust the information in the app (Mean score 4), citing reasons such as that the app is science-based. One participant responded that she was ‘unsure’ about whether the information in the app was trustworthy. She explained that she would always get a second opinion with anything health/medical related. Two others said they trusted the information as the researchers had made an effort to travel to the community and had research experience on the topic. There was discussion around the idea that they might trust the information more if it was in Urdu, as they could understand this better. Participants also said that testimonials would be helpful for building trust in genetics services.
Table 5 Acceptability of the gene appResponses to the data collection methodsIn the other phases, community members responded well to the online interviews. In Phase 4, they also tended to generally respond well to the SUS and bespoke questionnaire items, with all items responded to. However, three participants in Phase 4 sought clarification on what ‘integration’ and ‘inconsistencies’ meant (SUS items 5 and 6 Brooke 1996). Participants also tended to struggle more with the open-ended written questions, with many choosing not to answer them. Some participants accepted help in responding to the open-ended questions, opting to have a researcher transcribe some of their responses. This may have reflected language barriers, as the questions were written in English.
Comments (0)