
Remember me
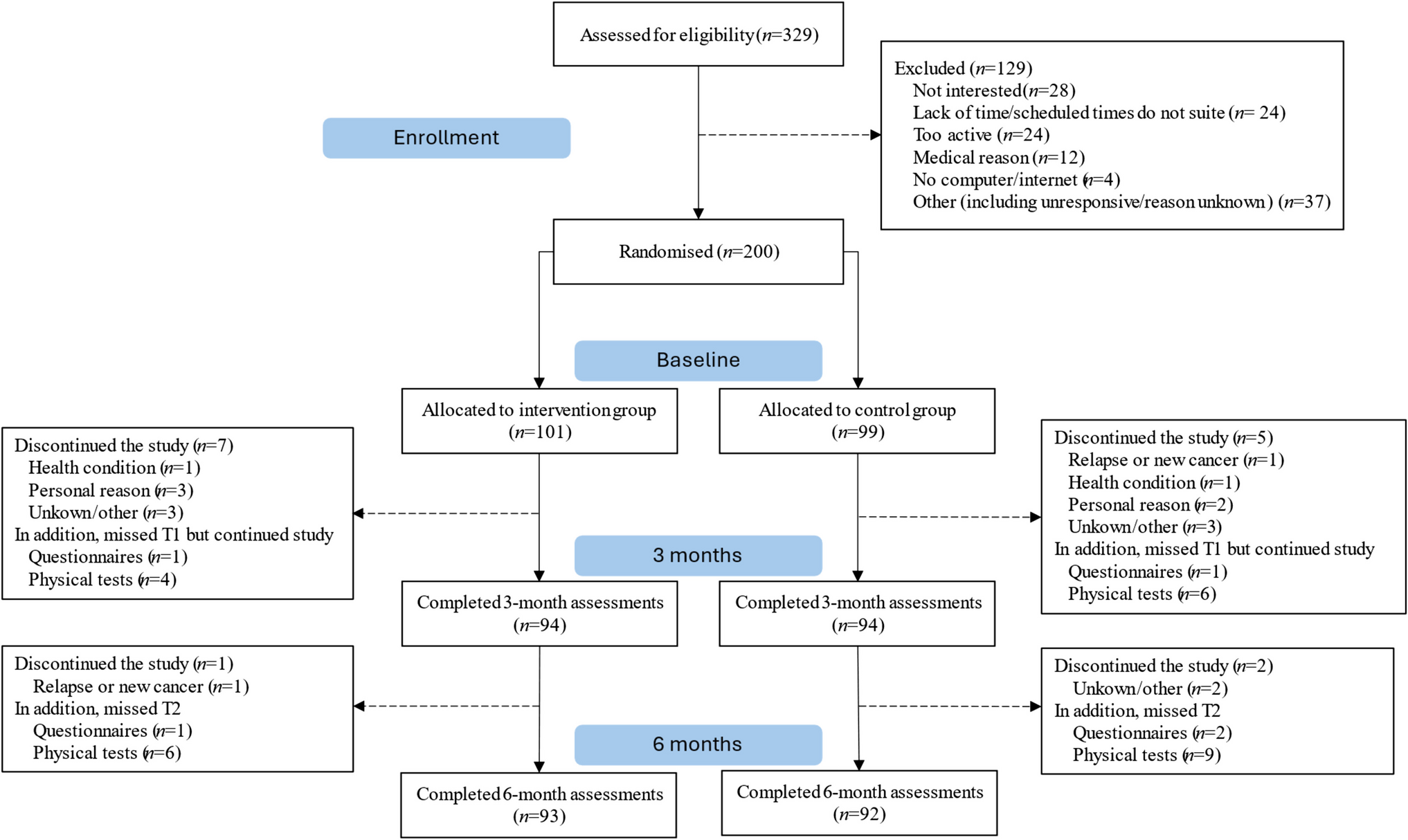



MELACARE was tested using a two-group RCT in which patients were allocated equally to the intervention or usual care (Fig. 1); this has previously been described [31]. The study was conducted at the Department of Plastic Surgery, Copenhagen University Hospital, Herlev and Gentofte, Denmark. We followed CONSORT [32] and TIDieR for reporting [33].
Fig. 1
CONSORT diagram. FCR, fear of cancer recurrence; PROM, patient-reported outcome measure. 1Not permanently living in Denmark or moved abroad
Study population and recruitmentPatients were eligible for inclusion if they had been surgically treated for melanoma stages IA–IIA within 3 months of recruitment, had no prior history of other cases of melanomas or other cancers excluding non-melanoma skin cancer, were aged 18 years or more, and had sufficient proficiency in Danish. Exclusion criteria included a high risk of a new melanoma (i.e. presence of dysplastic nevus syndrome or a first-degree relative with melanoma), comorbidity that made SSE teaching impossible (e.g. physical or mental disabilities), and no sentinel node detected in the case of lymphoscintigraphy. Patients were screened for eligibility by the principal investigator (SMH, medical doctor) and were consecutively recruited by telephone by the principal investigator, a project nurse, or a medical student between March 9, 2021, and September 28, 2023.
Random assignmentRandom assignment was computer-generated and performed using a closed site (www.melanoma.dk) in blocks of eight patients. Participants were randomised 1:1 to the intervention or control group and stratified according to clinical stage (IA vs. IB vs. IIA). Allocation was blinded to the participants until random assignment. After random assignment, blinding of the allocation to participants, the principal investigator, physicians, and project and melanoma nurses was impossible.
Control groupPatients in the control group received treatment as usual with follow-up according to their clinical stage (Fig. 2). Follow-up consists of regular physician-performed skin and lymph node exams. Patients with stage IA have one follow-up appointment at 3 months, whereafter they are discharged. Patients with stages IB–IIA have one follow-up appointment every 12 months for 5 years.
Fig. 2
Study schedule of trial activities in the intervention and control groups. Aug, August; PRO, patient-reported outcomes
InterventionThe intervention aimed to educate patients in SSE for recurrence detection and to provide psychosocial support to reduce FCR through nurse-led follow-up. The following are the components of the intervention follow-up:
1)Three to five nurse-led follow-up in-person individual sessions within the first 2 years of randomisation (Fig. 2, Online Resource 1). The main focus of the sessions was to provide information on and practice SSE, provide information on which symptoms would require the patient to contact the hospital department, and educate patients on coping with FCR using the metacognitive strategies detached mindfulness (DM) and worry postponement (WP) [31], both of which were part of previous successful intervention studies [27, 28]. Nurses delivering the intervention received a 2-day training program from a medical doctor and two psychologists (Online Resource 2). The nurse sessions were supported by:
2)The “Melanoma – Questions and Answers” booklet [34] with information on melanoma, SSE, and coping strategies.
3)Patient-reported outcome (PRO) assessment using the melanoma-specific HRQoL questionnaire “Functional Assessment of Cancer Therapy – Melanoma” (FACT-M) [35, 36]. The items were discussed at the sessions, and action was taken according to predefined guidelines (Online Resource 3) if any items exceeded predefined thresholds.
4)One scheduled appointment with a physician (plastic surgeon) was conducted to ensure the participants’ eligibility to perform SSE (Fig. 2). Hereafter, no regular appointments with a physician were scheduled, but self-requested appointments were available throughout the study period [31].
Data collectionBaseline socio-demographic data, including marital status, education, number of children, and household income, were collected electronically through a questionnaire using the Research Electronic Data Capture (Vanderbilt University, Nashville, TN). Baseline clinical data, including age, gender, and melanoma stage, were collected through the medical records. PRO data on FCR, anxiety, depression, distress, HRQoL, workability, and patient activation were collected through validated questionnaires at baseline and after 6, 12, and 24 months of follow-up. Information on SSE frequency and confidence, satisfaction with the follow-up program, and use of DM, WP, and booklet were collected through a study-specific questionnaire at 6, 12, and 24 months of follow-up (Online Resource 4). Clinical data, including recurrences, new primary melanomas, additional unplanned physician consultations, excisions, or scans, were collected through the medical records.
All in-person nurse sessions were audio recorded (with patient permission) to assess the fidelity of the intervention delivery, and two independent raters assessed whether the nurses delivered the expected intervention components to the patients at Sessions 1 and 2. Information on session duration, FACT-M completion, and actions taken due to FACT-M responses was registered by the nurse after each session.
OutcomesPrimary outcomeThe primary outcome was FCR, measured using the Danish version of the Concerns About Recurrence Questionnaire 4 (CARQ-4) [36, 37] at 6 months follow-up. CARQ-4 is a validated four-item scale with a total score ranging from 0 to 40; higher scores indicate greater FCR levels, and scores above 11 indicate FCR warranting clinical assessment [37]. No minimal clinically important difference (MCID) has been described for CARQ-4.
Secondary outcomesSecondary outcomes included several PROs: anxiety, depression, distress, HRQoL, workability, patient activation, number of SSEs, use of DM and WP, use of the booklet, and satisfaction with the follow-up program. Anxiety was measured using Generalised Anxiety Disorder-7 (GAD-7), which has seven items, scores ranging from 0 to 21, scores ≥ 10 indicating significant anxiety, and higher scores indicating more profound anxiety [38, 39]. The Patient Health Questionnaire-9 (PHQ-9) was used to measure symptoms of depression; it has nine items, and scores range from 0 to 27, where higher scores indicate a higher risk of having depression, and a cut-off of ≥ 10 indicates moderate to severe depression [40, 41]. Distress was assessed using the distress thermometer (DT), a single-item tool where patients rate their distress on a scale from 0 (no distress) to 10 (extreme distress), and we used the cut-off of 3 or above to identify patients with significant distress [42, 43]. We used the EuroQol 5-Dimensions 3-Levels questionnaire (EQ-5D-3L) to evaluate HRQoL [44]. It evaluates five dimensions of health, each with three severity levels, and includes a visual analogue scale for overall health rating. Raw scores are transformed into a utility score that ranges from 0 to 1, with scores closer to one indicating better health status. Workability was evaluated using the Work Ability Index (WAI), a 7-item scale ranging from 7 to 49; higher scores indicate better workability, and scores of 27 or under are considered poor workability [45, 46]. The Patient Activation Measure (PAM) was used to assess patient activation. PAM includes 13 items, and scores are converted into levels that range from low activation (Level 1) to high activation (Level 4) [47].
Secondary outcomes also included recurrences, new melanomas, additional unplanned physician consultations, excisions, and scans, as well as intervention fidelity measured as adherence to the protocol and delivery, session duration, FACT-M completion rate, and actions taken due to FACT-M responses (e.g. referral to physiotherapy).
Sample size and power calculationWe calculated the sample size a priori and expected effect size of Cohen’s d of at least 0.3 on the primary outcome, as found in a similar study at 6-month follow-up [27]. With an expected attrition rate of 10% and a power of 79% to detect a small effect size of Cohen’s d = 0.3, 340 participants were needed (170 per group).
Statistical analysesThe primary outcome was FCR after 6 months of follow-up. The intervention effect, comparing the mean outcome of FCR after 6 months under the intervention regime to the control regime, was estimated using targeted maximum likelihood estimation (TMLE) [48]. TMLE was also used to estimate the intervention effect for the secondary outcomes of distress, anxiety, depression, HRQoL (dichotomised as 1:HRQoL = 1 and 0:HRQoL < 1), patient activation, and workability. TMLE was furthermore used in the subgroup analyses assessing the effect on FCR within the subgroups of FCR at baseline (> 11 or ≤ 11), age (≥ 60 or < 60), sex, and civil status. Since HRQoL was considered a binary outcome, the effect was reported as the risk difference between the intervention and control regimes. In analyses of the other outcomes, the effect was reported as the mean difference.
TMLE was used instead of the protocol’s proposal of linear mixed models [31] to obtain a marginal intervention effect estimate, adjust for imbalance in baseline covariates, relax normality assumptions, and provide more accurate confidence intervals and p-values. Details about the TMLE analyses can be found in the appendix (Online Resource 5). Additional analyses, including those from the protocol paper, can be found in the appendix (Online Resource 6).
SSE-related outcomes; satisfaction with the follow-up program; the use of DM, WP, and the booklet; and the number of extra physician consultations, unplanned scans, and extra excisions were calculated as percentages for each group. Overall fidelity was calculated as the percentage of intervention components delivered relative to the total planned components. Interrater fidelity was measured as the proportion of agreement between the two raters.
All tests were two-sided with a significance level of 0.05. The data analyses were performed using the R package tmle [49] and R version 4.3.3.
Comments (0)