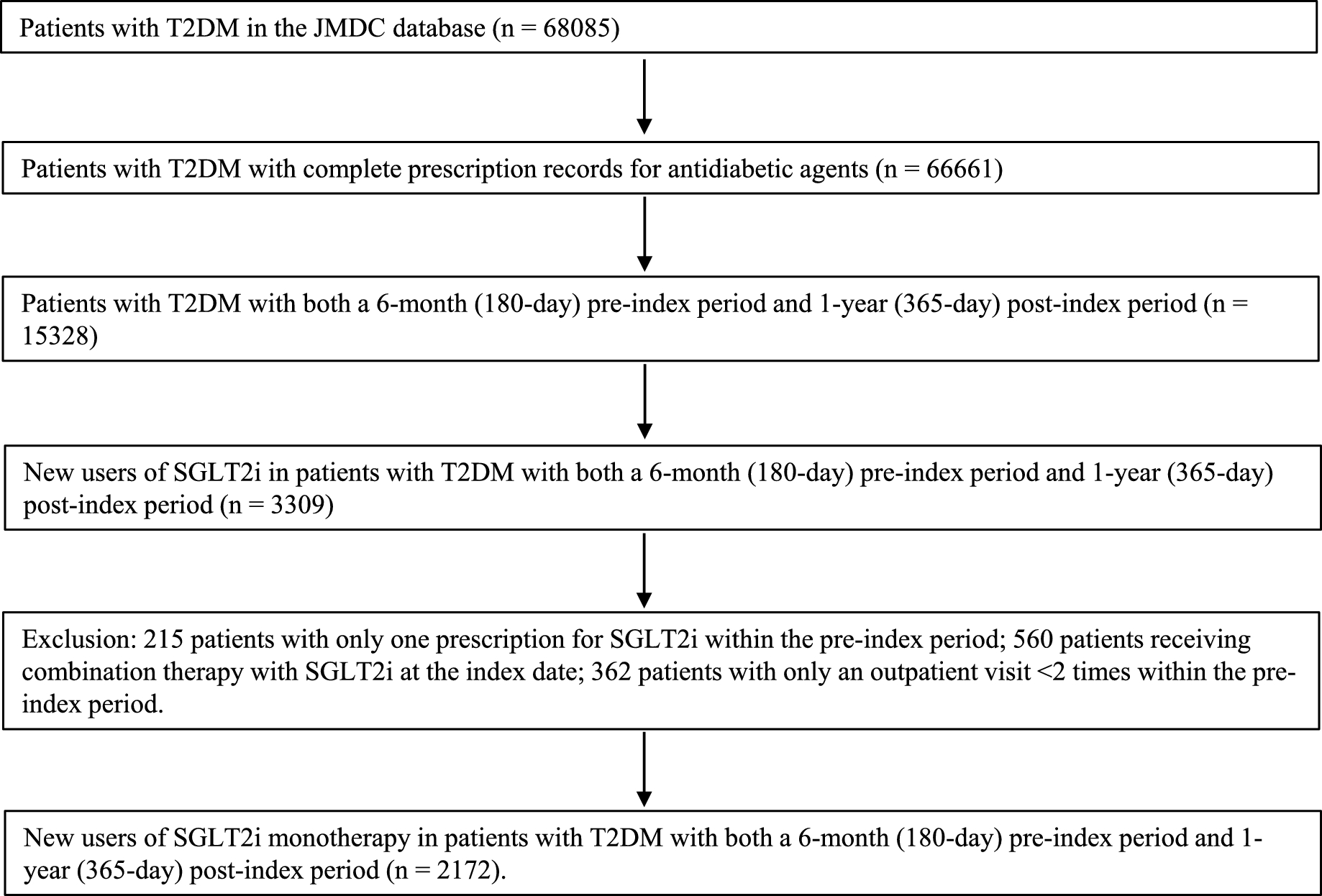
Using the JMDC database, a retrospective study on patients with T2DM was conducted to examine persistence and adherence rates to SGLT2i monotherapy and identify factor(s) affecting persistence/adherence. Persistence rates to SGLT2i without exceeding 90- and 30-day gaps at 365 days were 60.0 and 53.8%, respectively. Mean PDC at 365 days was 71.2%, and 58.3% of patients adhered to treatment.
Persistence and adherence rates in the present study were equivalent to those in a previous review [6]. An older age (shown at one-year intervals), hypertension, dyslipidemia, and hyperuricemia were factors increasing persistence and adherence to SGLT2i monotherapy.
A systematic review of 22 observational studies from eight countries (excluding Japan) revealed that the pooled persistence rate without exceeding a 90-day gap to SGLT2i therapies at 12 months was 58.9%, the pooled mean PDC at 12 months was 72.0%, and the pooled percentage of adherence at 12 months was 49.0% [6]. The present results showed that the persistence rate to SGLT2i without exceeding a 90-day gap at 12 months was 60.0%, the mean PDC at 12 months was 71.2%, and 58.3% of patients adhered to treatment. The results obtained on persistence and adherence rates in the present study, which was performed in Japan, were equivalent to those in a systematic review [6]; a study by McGovern et al., which was included in the review, reported the highest persistence rate of 69.5% at 1 year and the mean age of patients was 66.1 years [20]. Additionally, the present results were slightly worse than the findings reported by Kurtyka et al., which had the same gap period of 90 days in the JMDC database; the persistence rate to DPP4i monotherapy at 12 months was 72.2%, while the mean PDC and percentage of adherence were 76.6 and 67.2%, respectively [5]. These results support persistence and adherence rates to SGLT2i monotherapy at 12 months being slightly lower than those to DPP4i monotherapy [7]. Persistence depends on the gap periods of each study. Consistent with previous findings [21], the present results showed that the persistence rate to SGLT2i monotherapy with a 90-day gap period was higher than that with a 30-day gap period. The results obtained herein showed that even if a 30-day gap period was permissible, the persistence rate to SGLT2i monotherapy in patients with T2DM was higher than 50%.
The present study demonstrated that an older age reduced the risk of poor persistence and adherence, which is consistent with the findings of observational studies on patients with T2DM who received OAD [5, 10, 22]. Patients with T2DM who adhere to treatment are more likely to have good glycemic control [23], while those who do not are expected to have poor clinical outcomes [1, 2]. Based on these findings, older patients with T2DM who adhere to treatment may have relatively good glycemic control: however, our database was unable to capture hemoglobin A1c.
Comorbid conditions, such as hypertension, dyslipidemia, and hyperuricemia, were associated with a lower risk of the discontinuation of SGLT2i monotherapy: the adjusted odds ratio for hypertension was 0.72 (95% CI 0.57–0.91), that for dyslipidemia was 0.74 (95% CI 0.60–0.90), and that for hyperuricemia was 0.75 (95% CI 0.60–0.95). “The healthy adherer effect”, which indicates that patients with a chronic condition(s) are more likely to adhere to their therapies [24], appears to have contributed to these results because the majority of patients in the present study had chronic conditions, and older Japanese patients with T2DM are expected to have diabetic complications [25]. Additionally, one systematic review to summarize factors associated with good adherence to urate lowering therapy showed that adherent patients with gout had a high number of comorbidities, diabetes, and hypertension [26]. These findings partially support the present results. A previous study showed that hypertensive patients with controlled blood pressure were more likely to be adherent than those with uncontrolled blood pressure [27]. Furthermore, self-monitoring blood pressure is one of the interventions that achieves good adherence to anti-hypertensive medication [28]. Patients with hypertension or dyslipidemia may visually monitor their blood pressure or blood lipid levels. Neither blood pressure nor blood lipid levels at baseline were available for analysis, which may have been because our cohort included stable patients with hypertension or dyslipidemia. The reason why the odds ratios for hypertension, dyslipidemia, and hyperuricemia were lower than that for an older age currently remains unclear: the adjusted odds ratio for an older age was 0.97 (95% CI 0.96–0.98).
The present study showed that an older age, hypertension, dyslipidemia, and hyperuricemia were associated with persistence and adherence to SGLT2i monotherapy, which was consistent with that of other OAD. Kurtyka et al. and Miwa et al. reported that a younger age and comorbidity were associated with lower adherence and higher discontinuation to DPP4i monotherapy or DPP4i regimens [5, 9]. Tunceli et al. demonstrated that a younger age and no concomitant medications increased the likelihood of non-adherence to antihyperglycemic agent monotherapy, which included more than 70% metformin [10]. Therefore, these factors may be common with adherence and persistence to OAD.
Several interventions have been reported to improve adherence in patients with diabetes, including diabetes education, increasing counselling, and keeping regimens as simple as possible [29]. Although the present study showed that the number of outpatient visits was not associated with a higher adherence rate to SGLT2i monotherapy, previous Japanese studies, such as a cross-sectional study conducted by Okuno et al., demonstrated that patients with more frequent outpatient visits had a better relationship with their doctors and higher adherence rates [30]. Regarding simple dosing, a recent study showed that the 1-year persistence rate was higher with DPP4i than with α-glucosidase inhibitors [7]. Patients with chronic diseases who receive their first prescription are more likely to discontinue treatment at an earlier stage [31]. Negative perceptions of long-term medication, such as adverse event(s), may affect the adherence of a new user to chronic medication despite the benefits of treatment [32].
The strengths of the present study were the use of a large healthcare claims database and the majority of data being obtained from clinics. Japanese patients with T2DM generally visit a clinic [33]. Therefore, the results obtained herein may be generalized to patients with T2DM who visit clinics. However, there are several limitations that need to be addressed. The present results may not be generalized to all patients with T2DM because there may have been a selection bias due to the JMDC database including a small population of individuals aged 65 years or older and not those aged 75 years. This bias may have also distorted the true relationship between an older age and good adherence/persistence. Furthermore, our cohort included approximately 70% male patients. Another limitation is that although our study only targeted SGLT2i monotherapy, combination therapy with OAD is common in Japan. Unmeasured factors, such as the duration of diabetes, hemoglobin A1c, and the body mass index, may have affected the results obtained based on previous findings showing that hemoglobin A1c was associated with poor adherence [34]. Furthermore, reasons for the discontinuation of SGLT2i monotherapy were not examined in the present study. These factors and reasons for discontinuation were not identified due to the lack of relevant data in the JMDC database. Previous studies showed that the Morisky score was associated with medication adherence in patients with T2DM [4, 35]; however, we were unable to incorporate this variable due to the nature of the healthcare claims database. Since the present cohort had strict inclusion criteria assuming new users of SGLT2i, the relationship between previous experience with antidiabetic agents and adherence to SGLT2i was not investigated. Moreover, it is unclear whether patients actually took SGLT2i because the present study relied on prescription data.

Comments (0)