Continued identification of risk factors for SSI following instrumentation of degenerative lumbar spinal diseases is crucial from a clinical perspective, as it as helps develop a more comprehensive understanding of this specific patient population. The study findings revealed that higher ASA class (III or IV compared to I or II), surgeries involving the sacral vertebrae, open surgery instead of minimally invasive surgery, longer surgical duration, and lower hemoglobin levels were identified as independent factors significantly associated with SSI.
The wide range of reported surgical site infection (SSI) rates, from 0.5% to 18.0%, can be primarily attributed to a variety of factors, including patient population characteristics, the methods used for defining and diagnosing SSIs, study methodology, and surgeon or hospital-related factors (Janssen et al. 2019; Ogihara et al. 2021; Luo, et al. 2022; Park et al. 2018; Veeravagu, et al. 1976). In the current study, we observed a moderate SSI incidence rate of 3.5%, however, some points should be noted. Firstly, the target population consisted of individuals with degenerative lumbar spinal diseases, excluding patients with trauma, tumors, or deformities, which themselves are known risk factors for SSIs (Gadot et al. 2022; Kumar et al. 2015; Baroun-Agob et al. 2021). Secondly, the study only included patients who underwent decompression and instrumentation, which represents the typical treatment approach for the majority of individuals with degenerative lumbar spinal diseases. Furthermore, we excluded patients who had previously undergone lumbar spinal surgeries or were undergoing revision surgery during the index hospitalization, regardless of the underlying reasons, as these individuals possess unique characteristics that could potentially confound the study results.
The association between a higher American Society of Anesthesiologists (ASA) score and an increased risk of surgical site infection (SSI) has been well-documented across various orthopedic subspecialties (Le et al. 2020; Ridgeway et al. 2005), and can be elucidated from multiple perspectives. First, a higher ASA score often indicates a greater burden of comorbidities and overall poor health status, which can impair the immune system's ability to effectively combat infections. Secondly, individuals with a higher ASA score may experience compromised tissue perfusion and impaired wound healing due to systemic factors such as decreased cardiac output or peripheral vascular disease (Bhat et al. 2024). Additionally, a higher ASA score may also be indicative of a higher prevalence of risk factors associated with SSI, such as obesity or diabetes, which can negatively impact wound healing and increase the susceptibility to infection.
Three surgery-related factors were identified as being associated with an increased risk of SSI, including involvement of the sacral vertebrae, open surgical approach, and longer operative duration. The involvement of the sacral vertebrae may increase SSI risk due to the proximity of the surgical site to the rectal and perineal regions, where a higher concentration of potentially infectious bacteria resides (Abdul-Jabbar, et al. 1976). Additionally, the need for a larger incision and more extensive tissue dissection to optimize surgical access for nerve decompression, fusion, and instrumentation can lead to heightened tissue trauma and blood loss, consequently augmenting susceptibility to infection. This finding aligns with the observed higher SSI risk for open surgeries compared to minimally invasive procedures. Similarly, prolonged surgical duration may reflect the complexity of condition or the surgical procedure itself, such as cases involving multiple spinal levels, obesity, or severe spinal stenosis surgery (Lee et al. 2016; Sponseller et al. 2010). These factors can expose patients to a higher bacterial load and provide more opportunities for bacterial colonization at the surgical site. To mitigate the increased risk of infection associated with these surgical factors, it is crucial to handle tissues carefully and, whenever possible, utilize minimally invasive surgical approaches.
The finding that preoperative lower hemoglobin concentration was associated with an increased risk of postoperative SSI aligns with several prior studies of surgically treated patients. Birhanu et al. (2022) identified a hemoglobin cut-off value of 70 g/L as risk factor for SSI. Similarly, an earlier study on patients undergoing spinal tumor surgery reported an increased risk of composite adverse events, with OR of 2.7 for a hemoglobin level < 90 g/L compared to ≥ 110 g/L (Wang, et al. 2023). Furthermore, another study focusing on spinal surgeries, particularly for degenerative spinal diseases, found that postoperative hemoglobin level was more likely an indicator for increased SSI; specifically, the risk of SSI increased by 6 times for a hemoglobin level of < 80 compared to ≥ 100/L (Woods et al. 2013). These findings underline the importance of closely monitoring and addressing preoperative anemia, significant intraoperative bleeding, and substantial postoperative decreases in hemoglobin levels. Particular attention should be given to patients presenting with these characteristics.
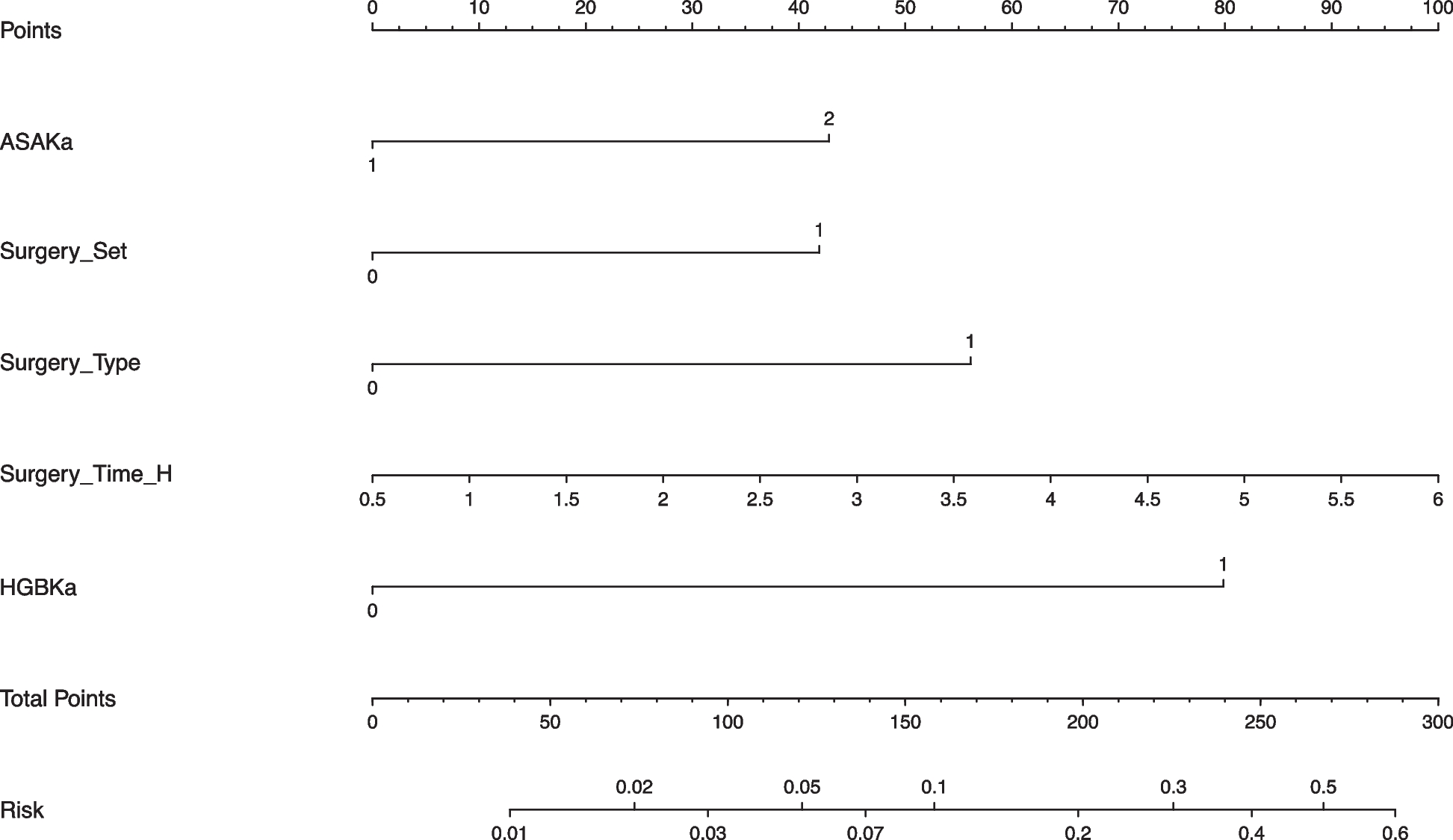
It should be noted that the predictive power of this nomogram is moderate, at only 74% (95% CI: 0.682–0.804), which is substantially below the ideal threshold of above 90% for clinical application. Nevertheless, our findings suggest that the nomogram can still provide valuable insights in risk stratification and decision-making, particularly given the complexity of the patient population and the multifactorial nature of the rare events, such as SSI in this context. We believe this nomogram can serve as a useful tool for clinicians, particularly when combined with clinical judgement (eg, operative trauma assessment, patient history) and other diagnostic information (such as lab test results and imaging studies). Future studies should aim to enhance the accuracy of the predictive model through various strategies, including expanding the sample size, incorporating additional relevant variables, or utilizing advanced modeling techniques.
Several limitations to this study should be acknowledged. First, the retrospective design inherently introduces potential biases in data precision and accuracy, particularly the documented comorbidities were self-reported by patients. Second, the patient population was drawn from a single tertiary referral hospital, which may have resulted in a selection bias, as patients treated may have more severe comorbidities and advanced diseases compared to those treated in community settings. Additionally, due to the strong imbalance between the SSI and non-SSI groups (only 53 events among 1,462 patients), our model may be at risk of overfitting despite internal validation. This limitation should be considered when interpreting the model’s predictive accuracy, and future studies with larger and more balanced samples are needed for external validation. Third, as with all multivariate regression models, there remains a risk of residual confounding due to unmeasured variables. In this study, we were unable to collect some key data, such as the extent of soft tissue damage, details of medication use, wound care practices, and postoperative rehabilitation protocols. Furthermore, we only classified surgical technique as “open” or “minimally invasive,” without recording specific intraoperative practices such as wound closure methods, drain usage, or antisepsis protocols, all of which may influence infection risk. Additionally, other important clinical factors—such as a more comprehensive evaluation of nutritional status, use of immunosuppressive agents, and wound classification—were not included in our analysis. The absence of these variables may result in residual confounding; therefore, our findings should be interpreted with this limitation in mind. Fourth, although the study conducted internal validation, it is important to emphasize that external validation is still necessary to ensure the practicality and applicability of the predictive model across diverse healthcare settings. Lastly, as our study period included the years of the COVID-19 pandemic, it is possible that perioperative protocols and patient selection were altered in response to the pandemic. Such temporal shifts could have affected both the exposures and outcomes evaluated, and may have introduced bias into our findings. This limitation should be considered when interpreting our results.
In summary, this study of surgical patients with lumbar degenerative disease observed a moderate SSI rate of 3.5% and also identified five independent risk factors as being associated with SSI: higher ASA class (III or IV compared to I or II), surgeries involving the sacral vertebrae, open surgical approach, longer surgical duration, and lower preoperative hemoglobin levels. These findings can inform preoperative patient counseling, risk assessment, and the development of personalized risk management strategies for implementation of targeted interventions to mitigate the likelihood of postoperative SSI.





Comments (0)