Suicide is one of the leading causes of death worldwide [1]. With a phenomenology comprising a wide range of thoughts and behaviors, suicide risk is often conceptualized along a continuum of increasing degrees of severity [2]. While the global estimates indicate that more than 9% of individuals experience suicidal ideation (SI) during their lifetime, only 29% of them enact a suicide attempt (SA) [3]. For this reason, recent models often refer to an ideation-to-action framework, studying the contributors to the progression from suicidal thoughts to their enactment, in order to improve screening, assessment, and prevention of suicide risk [4]. Substantial evidence suggests that pain, physical and psychological, is a key element in suicide risk [5,6,7,8,9,10,11,12,13,14,15,16,17]. Ideation-to-action theories all identify blunted pain perception as a primary factor in the transition from SI to SA, especially for lethal or near-lethal SA [18,19,20]. Pain-related aspects are some of the most debated topics in recent suicide literature. Although abundant, research on the connection between pain and suicide has at times reached contrasting conclusions. In particular, the role of pain sensitivity in facilitating the transition from SI to SA still warrants further investigation. This work aims to highlight key evidence on the connection between pain and suicide while proposing a new conceptual model.
Pain and Suicide
A lot has been written about the link between pain and suicide. Only on PubMed, no less than 14 systematic-reviews and meta-analyses have been published over the course of the last 10 years containing the keywords ‘pain’ and ‘suicide’ in their title, whose findings will be detailed in the following paragraphs. Most of them revolve around two main aspects that have been hypothesized to pose a higher suicide risk, namely physical pain [5,6,7,8,9,10,11,12] and psychological pain [13,14,15,16,17]. Only one record [21] focuses on physical pain sensitivity among people with a history of SA.
The records concerning physical pain indicate that individuals living with any kind of physical pain report higher rates of death wishes, SI, suicidal planning, SA and death by suicide, as well as non-suicidal self-injury (NSSI) [5,6,7,8,9,10,11,12]. Such relationships are not limited to the adult population but were also found in adolescent clinical and community samples [6, 8, 12]. Among the factors related to higher rates of suicidal behavior in chronic pain patients, comorbid psychiatric conditions were often mentioned, especially depressive disorders [6, 9,10,11] but also anxiety disorders [10], post-traumatic stress disorder (PTSD) and borderline personality disorder (BPD) [9].
According to Shneidman’s model of suicide [22], psychache, or psychological pain, which arises when vital psychological needs are unmet, is considered the main psychological risk factor for suicide vulnerability, when deemed unbearable by the subject. The records focusing on this kind of pain highlighted that higher levels of psychological pain were associated with higher rates of SI and SA in mood disorder patients, other psychiatric patients and nonclinical samples [13, 14, 17]. The association remained significant even when controlling for depression [17] and psychological pain seemed to be a stronger predictor of SI than depression [13]. A systematic review of magnetic resonance imaging (MRI) studies found alterations among adolescents with SI and SA histories in an emotional pain circuit, composed of cerebellum, amygdala and hippocampus. However, alterations in what they defined as a ‘social disconnect’ circuit, composed of lateral orbitofrontal cortex, temporal gyrus and their connections, were specific to those with a history of SA [15]. Moreover, hypofunctioning of cannabinoid receptors connected to the modulation of neuropathic pain, which might also play a role in modulating mental pain, distinguished patients with SA history from those without [16].
One meta-analysis [21] examining physical pain thresholds and tolerance in people with a history of SA challenged the ideation-to-action frameworks’ hypothesis that increased pain tolerance heightened the risk of transitioning from suicidal thoughts to SA [18,19,20]. Indeed, while pain tolerance was higher among people with a history of SA, as compared to nonclinical controls, neither pain threshold nor tolerance reliably differentiated people attempting suicide from other psychiatric patients. Altered pain perception seemed to characterize overall psychiatric vulnerability.
Pain Hypersensitivity and Neuroinflammation
Since both physical and psychological pain appear to play a pivotal role in suicide-related thoughts and behavior, it is worth introducing a concept consistently linked to both: neuroinflammation. Inflammation is relayed to the brain by the immune system through interoceptive visceral afferent pathways, as well as humoral and cellular interoceptive pathways. Inflammatory processes are also mediated by top-down projections from the brain that modulate autonomic sympathetic and parasympathetic responses [23, 24]. Acute inflammation is an adaptive response to physical or emotional stress that serves to reprioritize physiological responses to address potential threats. However, chronic inflammation causes long-lasting biochemical changes that contribute to the development and maintenance of chronic pain conditions [25,26,27,28,29] and psychiatric disorders, particularly depressive disorders [23, 26, 30].
For example, prolonged neuroinflammation may lead to persistent central sensitization, a phenomenon in which maladaptive neuroplasticity induces lasting hyperexcitability of central pain pathways, resulting in amplified pain processing and pain hypersensitivity [31,32,33]. Central and peripheral inflammation play a role in the pathogenesis of chronic pain [34] and patients with chronic pain conditions often possess hypersensitivity to physical pain, expressed by lower pain thresholds compared to healthy controls [35]. Indeed, neuroinflammatory processes lead to heightened processing of aversive interoceptive stimuli and increased interoceptive hypervigilance, reflected by abnormal activation in the posterior insula, dorsolateral prefrontal cortex (PFC), anterior cingulate cortex (ACC) and somatosensory cortex [32, 36]. Moreover, neuroinflammation tends to inhibit fear extinction processes, thus strengthening the neural signature of interoceptive fear memory traces [32, 36, 37]. Interoception, defined as the sensing of the physiological condition of the body [38,39,40], intertwines with many metacognitive dimensions, such as cognitive appraisal and interpretation, affective evaluation, as well as the degree of trust and attention given to interoceptive sensations [41]. Sustained neuroinflammation also affects these components facilitating stress-sensitization processes and thus altering emotional processing and affect regulation [42]. Consistently, interoceptive signaling of inflammation appears to be involved in the etiology of mood disorders [30] and metacognitive components of interoception are thought to be implicated in the pathogenesis of some anxiety disorders, such as panic disorder [43]. Additionally, a possible adverse consequence of inflammation-induced interoceptive hypervigilance is pain catastrophizing, one of the most important correlates of pain chronicity and disability [44]. During resting-state fMRI, patients living with chronic low-back pain displayed abnormal connectivity between the amygdala and the ‘central executive network’, which may be associated with increased pain catastrophizing and rumination [45]. Finally, since the neural networks involved in physical and psychological pain processing partially overlap [46,47,48,49], neuroinflammation could also induce hypersensitivity to psychological pain [30, 50].
Not surprisingly, consistent evidence also suggests an involvement of peripheral and neuroinflammatory processes in suicidal behavior [50,51,52,53]. Increased pain sensitivity has indeed been observed among older adults with SI and SA histories, who also recurred more frequently to opioid analgesics and reported a greater impact of pain on their quality of life [54, 55]. Moreover, interoceptive dysfunctions, especially in cognitive and emotional appraisal of bodily sensations, were associated with suicide-related outcomes [56, 57]. More specifically, lower trust in bodily sensations was connected to both SI and SA among the general population, while those with a history of SI seemed to be particularly characterized by lower capacity to regulate worry about unpleasant bodily sensations [58]. However, results were different using different interoceptive measures [59].
Such findings align with the work of Elman and colleagues [60], who highlighted the role of altered anti-reward brain networks in chronic pain conditions and suicidal behavior, similarly to what was observed in addictive behaviors. Prolonged pain or stress may indeed produce desensitization of reward and sensitization of anti-reward networks, alongside pain-stress cross-sensitization. This translates into aberrant learning processes, increasing incentive salience attribution to pain-related stimuli and enhancing responsivity to stress and negative emotional states. Similarly, a suicide-stress cross-sensitization is also theorized based on evidence of strong links between life adversities and suicide-related behaviors. Consistently, increased frequency and lethality of SA observed in some patients could in part be explained by aberrant salience attributed to suicide-related content. Similarly to addictive behaviors, pain-stress and suicide-stress cross-sensitization may narrow the behavioral repertoire and facilitate habit-based, pseudo-compulsive self-injurious and suicidal behaviors.
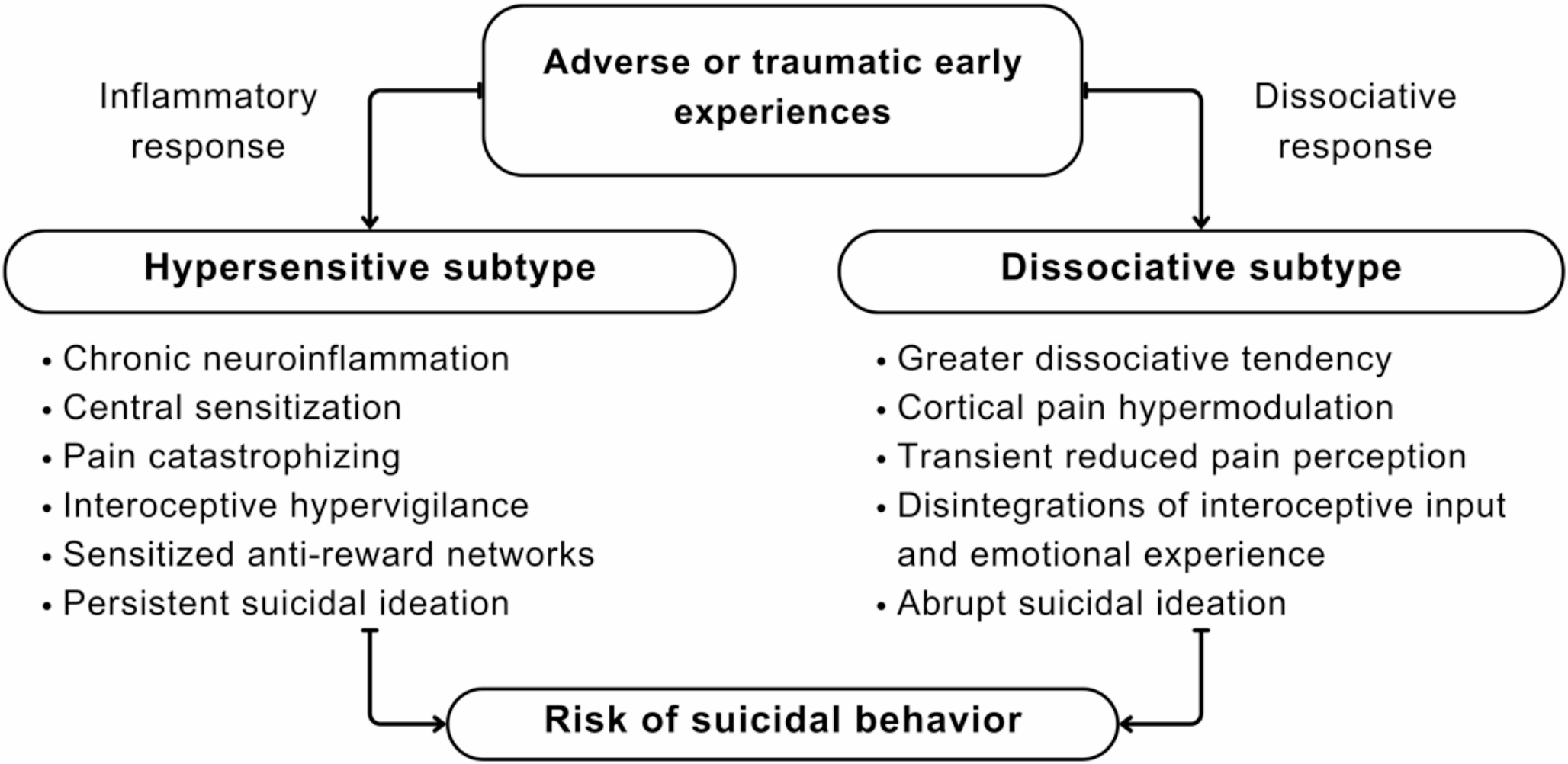
Considering all this evidence, contrary to what is hypothesized by ideation-to-action theories, at least some individuals at risk of suicide, such as those with depression and chronic pain, may possess enhanced pain sensitivity. These patients may belong to a hypersensitive subtype of individuals at risk of suicide, characterized by inflammation-induced central sensitization, impaired interoceptive pain, and fear extinction processes and sensitized anti-reward brain networks. Such individuals may struggle to shift their attention away from psychological and physical pain, as well as suicide-related content, leading to pain catastrophizing, hopelessness and potentially more persistent SI. However, while we suggest that some at-risk patients may belong to this hypersensitive subtype, not all individuals at risk of attempting suicide will necessarily exhibit this exact pattern.
Pain Hyposensitivity and Dissociation
Despite strong evidence linking suicide risk to heightened pain sensitivity, most recent theories of suicide emphasized increased pain tolerance as a risk factor in the transition from suicidal ideation to action [18,19,20]. This apparent contradiction between empirical findings and theoretical models warrants a closer examination of the origins of the increased pain tolerance hypothesis and a reconsideration of current conceptualizations.
Pain hyposensitivity as a risk factor for suicide was first proposed by Orbach and colleagues, who viewed it as part of a broader indifference toward bodily sensations, stemming from a dissociative disposition, which was thought to facilitate self-aggression [61]. Consistent with this theory, they found that individuals hospitalized after a suicide attempt exhibited higher pain thresholds and tolerance [62,63,64], lower interoceptive abilities [65] and higher levels of dissociation [66] compared to both psychiatric inpatients without a history of SAs and non-clinical controls. Later, Joiner’s Interpersonal-Psychological Theory of Suicide (IPTS) [20,



Comments (0)