Burnout among healthcare workers can impair clinical decision-making, hinder effective communication with patients and colleagues, and reduce their capacity to manage work-related stress [15]. This study aimed to assess the prevalence of burnout among Sudanese healthcare workers and explore the coping strategies they use amid the ongoing conflict.
The ongoing Sudanese military conflict has severely impacted healthcare services due to infrastructure destruction and a critical shortage of health workers [16]. The WHO has verified 88 attacks on healthcare resulting in 55 deaths and 104 injuries [17]. Incidents of killing, kidnapping, and assault have worsened the shortage of healthcare staff [3]. This is further exacerbated by shortage of medications and equipment [18, 19] and outbreaks of diseases like cholera and dengue [20, 21]. These factors likely contribute to the high levels of burnout among healthcare workers in Sudan. It has been suggested that there is an interaction between burnout and secondary traumatic stress in the Middle East [22].
Depersonalization was the most affected in our study, followed by emotional exhaustion and, finally, personal accomplishment, with only 4.4% reporting low levels of personal accomplishment. This aligns with findings from other countries [23, 24]. Notably, the proportion of participants experiencing depersonalization in our study was higher than that reported among healthcare workers in Gaza during their war [25]. These findings suggest that physicians in conflict-affected settings have a strong sense of self accomplishment, however factors like the workload, staff shortage, and working environment cause emotional exhaustion and depersonalization leading to high levels of burnout. Depersonalization and emotional exhaustion are considered the core components of burnout, whereas reduced personal accomplishment may act as either a precursor or an outcome of the syndrome [26]. The particularly high levels of depersonalization observed may indicate a psychological coping mechanism, whereby healthcare workers detach emotionally from their patients as a way to shield themselves from chronic stress [26]. In settings like Sudan, where prolonged trauma exposure and critical resource limitations are common, this emotional distancing can serve as a necessary—though potentially harmful—adaptation to survive in a highly strained and unsupportive healthcare environment.
Nearly two-thirds of the participants in this study were internally displaced. Sudan has the largest displacement crisis, more than 11 million internally displaced people [27]. There was no significant association between displacement status and burnout domains in this study. Less than one-fifth of participants had more than five years of experience, which may reflect the characteristics of healthcare practitioners remaining in Sudan during the war. Senior physicians are more likely to find jobs abroad to support their families, while younger physicians, who lack training, are more likely to stay. This pattern may also reflect differences in social media use and availability, as younger physicians are more likely to complete online questionnaires. These plausible explanations require further investigations to obtain robust evidence. Burnout levels varied by years of experience, with early-career professionals (1–5 years) showing significantly higher emotional exhaustion and depersonalization. This finding is consistent with previous studies that have reported greater burnout among those with fewer years of experience [28, 29].
Nurses were more likely to report depersonalization compared to physicians; however, this difference was not statistically significant. A study conducted among healthcare workers during the COVID-19 pandemic found that Sudanese physicians were more likely to report burnout compared to nurses. A plausible explanation for this finding is the heavier workload and frontline role of physicians during COVID-19. This contrasts with findings from other studies that report higher levels of burnout among nurses [30, 31]. Some studies, however, report no significant difference between the two groups [32]. Technicians were significantly less likely to experience emotional exhaustion compared to physicians, a difference that may also be attributed to workload.
Less than a quarter of participants reported having fully sufficient access to basic necessities. This is consistent with the general situation in war-torn Sudan, where one in every three people is at risk of food insecurity [33]. Insufficient but manageable access to basic necessities was significantly associated with high levels of emotional exhaustion and depersonalization. A probable explanation is that the affected access domain is financial, which can be managed by working longer hours in multiple hospitals. This year, food prices have increased by more than 120% [34].
More than two-thirds of participants reported a lack of access to psychological support. The expertise of mental health and psychological support groups is fragmented, and there is no shared platform to coordinate priority actions or strengthen responses to mental health needs [35].
Participants with extreme conflict exposure showed significantly higher levels of emotional exhaustion and depersonalization. Similarly, a study conducted among academic staff in Ukraine found that prolonged stress related to the ongoing war led to notable increases in depersonalization [36]. Despite the severe impact of the war, many conflict-related variables in our study were not significantly associated with burnout in our adjusted models. One possible explanation is that the conflict affected nearly all healthcare workers in some way, creating a uniformly high baseline of stress and reducing detectable differences across exposure levels. Additionally, the effects of the war may have manifested more through indirect stressors, such as economic hardship, longer working hours, and lack of basic resources, which were better captured by other variables like access to necessities and living arrangements.
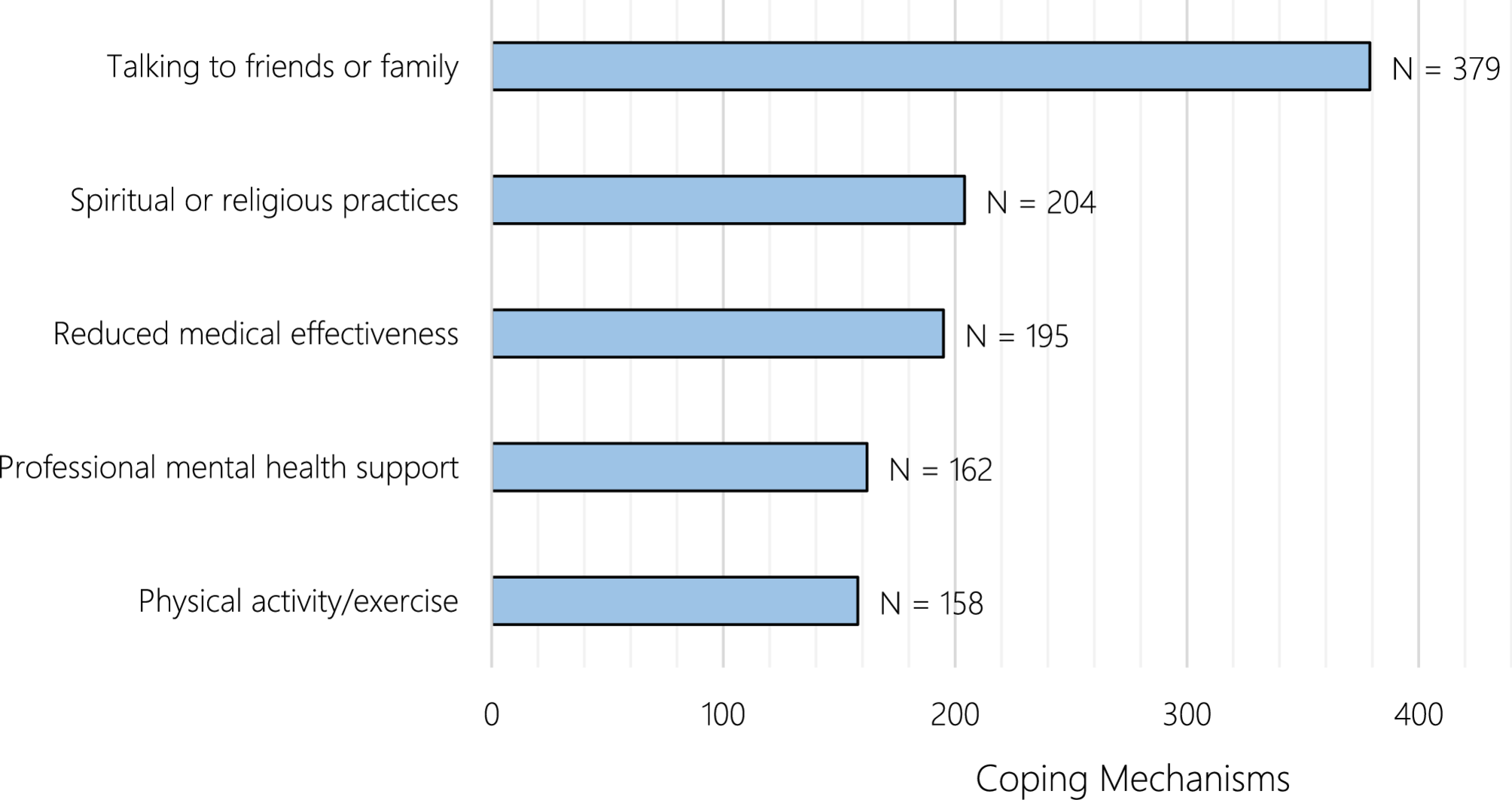
The most commonly reported coping mechanisms were talking to friends and families as well as spiritual or religious practices. Previous studies have found that social relationships may help in managing the effects of burnout [37, 38]. Additionally, religious practices are regarded as protective and beneficial in managing burnout [39, 40]. A previous study conducted among displaced individuals in shelters in Port Sudan highlighted the significant role of religious and spiritual practices—such as prayer, reading the Quran, and trusting in God—in coping with distress. The study also emphasized the importance of social and emotional support, noting that individuals often leaned on family ties and built supportive social relationships to manage their circumstances [41]. These coping strategies may reflect the strong communal and religious values embedded in Sudanese culture, where individuals often rely on close-knit family networks and faith during times of crisis. In the context of limited access to formal mental health services during the conflict, these culturally rooted mechanisms may serve as essential substitutes, helping individuals manage stress and emotional exhaustion.
This study offers valuable insights into burnout among healthcare providers in a conflict-affected country. A notable strength is the inclusion of participants from various professional roles within the healthcare system. However, the interpretation of the findings should consider several limitations. The cross-sectional design restricts the ability to draw causal inferences. Moreover, the use of a non-probability sampling technique may limit the generalizability of the results. Participants’ responses may have been influenced by recall bias and the tendency to provide socially desirable answers. Additionally, the disproportionate distribution of participants across healthcare roles—with physicians comprising approximately two-thirds of the sample—may affect the representativeness and limit the generalizability of the findings to the broader population of healthcare workers.



Comments (0)