The findings of the present study confirm the feasibility of the mini-open approach with the MIPO technique for treating displaced midclavicular fractures. The important finding was that mini-opening with the MIPO technique could significantly reduce the incidence of complications, such as numbness, overall surgical satisfaction, surgical length, blood loss, and scarring, compared with conventional ORIF.
The overall outcomes of shoulder joint function, DASH score, and CMS were favorable in both groups. No statistical or clinical differences were observed in the final follow-up period. Attributed to the fact that, blood loss, incisional length, and 1st and 3rd postoperative VAS scores were significantly reduced by restoring the anatomical relationship of clavicle by mini opening of skin compared with ORIF. The VAS score was eventually lower in the ORIF group on the 5th day, which was comparable to that of the MIPO with mini-open technical group, as the healing recovery process was initiated. Therefore, orthopedic trauma surgeons should consider taking advantage of modern surgical practices to effectively manage the pain in patients with multiple traumas.
Except for one important variable, the mean operative time was greater in the MIPO group than in the ORIF group. Although the timing was not statistically significant between the two groups, it was longer in the MIPO group. This can be attributed to the relatively higher fluoroscopy time required for precise reduction and fixation. In contrast, as we gained experience with the technique after several procedures, the operative time and fluoroscopy usage were significantly reduced compared with ORIF. The ORIF procedure necessitated careful dissection and verification of fixation using an image intensifier at the conclusion of the surgery.
Recent studies on displaced midshaft clavicular fractures have concluded that nonoperative management is still well tolerated and must be the first-line management for these injuries. However, many clinical and radiological criteria have been determined for surgical indication of clavicular fractures. Operative management with ORIF is the gold standard protocol, with the advantages of early functional recovery, better functional outcome, and decreased rate of nonunion and malunion in the present context [22,23,24].
Operative treatment can result in iatrogenic injury, notably to vessels and nerves, tissue stripping leading to nonunion, implant failures, and deep infections as complications. To overcome such complications, MIPO has emerged in practice, which utilizes a mini surgical incision on the peripheral safe zone, escapes the bundle of supraclavicular nerves during mini-opening around the midclavicular area, and avoids complications significantly compared with conventional ORIF.
Contemporarily, fracture management emphasizes the importance of the biological status and does not harm the surrounding soft tissue. Blood supply to the clavicle arises solely from the periosteal artery, which might explain the incidence of nonunion in midclavicle fractures [25]. At least partially, it also preserves the fracture hematoma and promotes natural healing. One thing that nature does not often facilitate is proper alignment, which is what internal fixation with MIPO provides to an end [21].
Since the introduction of MIPO, the principle of bone healing has been biological fixation by internal bridging of the fracture with preservation of soft tissue in long bone fractures [26]. In the last decade, studies have suggested that closed reduction and submuscular plating techniques through percutaneous insertion have comparable fracture healing rates and a lower percentage of non-union than ORIF [26]. We did not encounter any primary complications such as nonunion, malunion hardware irritation, implant failure, or deep infection in either group. Hence, MIPO with mini-open techniques works on the relative stability and gross restoration of length, rotation, and alignment.
The present study emphasizes the importance of the mini-open technique with MIPO evaluating risk factors for SCN injury. A study by Nathe et al. [25] reported that there is no SCN branch within 2.7 cm from the sternoclavicular joint or 1.9 cm from the acromioclavicular joint, but between the two limits, there are variations in nerve branches, which explains the lower incidence of SCN injury after MIPO compared with wide surgical access [25]. Supporting to this evidence, there were two patients (8%) who sustained the SCN neurovascular complications in the ORIF group and indisputably no patients with SCN injury in the MIPO group.
With precautions during ORIF, such as careful dissection, avoidance of excessive traction, and proper handling of soft tissue to minimize the risk of supraclavicular nerve injury, there were nine (36%) patients who sustained numbness over the surgical scar and anterior chest compared with only one (5%) patient in the MIPO group. In some cases, nerve injury may be unavoidable owing to anatomical variations or unforeseen complications such as excessive stretching or traction during realignment and fixation during fracture manipulation. Symptomatic numbness is believed to be due to scar tissue impingement on the supraclavicular nerve, swelling, and callus or hematoma formation during the healing phase. Correspondingly, both the mini-open with MIPO and ORIF groups had significantly decreased symptomatic numbness over the scar and anterior chest, with minor discomfort after 6 months. This result is lower than that reported in other studies. Only two patients in the ORIF group had persistent numbness below the surgical scar until the latest follow-up. However, it did not cause significant discomfort or influence functional outcomes in the shoulder, as stated by You et al. [22]. Our study also aimed to address the discrepancy between self-reported and clinically detected skin numbness as it underscores a critical aspect of postsurgical sensory evaluation and questionnaire scoring system. Self-reported numbness, which is more persistent and noticeable in daily life, likely has a greater impact on the quality of life than numbness identified only during clinical examination.
In support of our evidence, a study conducted by Ko et al. showed that only 14% of patients who underwent MIPO with minimal incisions lateral and medial to the fracture site and 27% of those who underwent ORIF developed SCN injuries [30]. Postoperative skin numbness is usually higher in patients who undergo ORIF than in those who undergo MIPO for midshaft clavicle fractures [13]. You et al. [31] observed a comparison of 70% and 30% in the ORIF and MIPO groups, respectively. In another study, ORIF for middle- and outer-third clavicle fractures was performed via a transverse incision, and 85% of the patients sustained SCN injury. In addition, 30% of patients’ symptoms persisted for an average of 2.7 years. MIPO generally has a number of benefits, including less tissue dissection, less blood loss, and perhaps less postoperative pain, which should shorten hospital stays, hasten healing, and shorten rehabilitation periods [22].
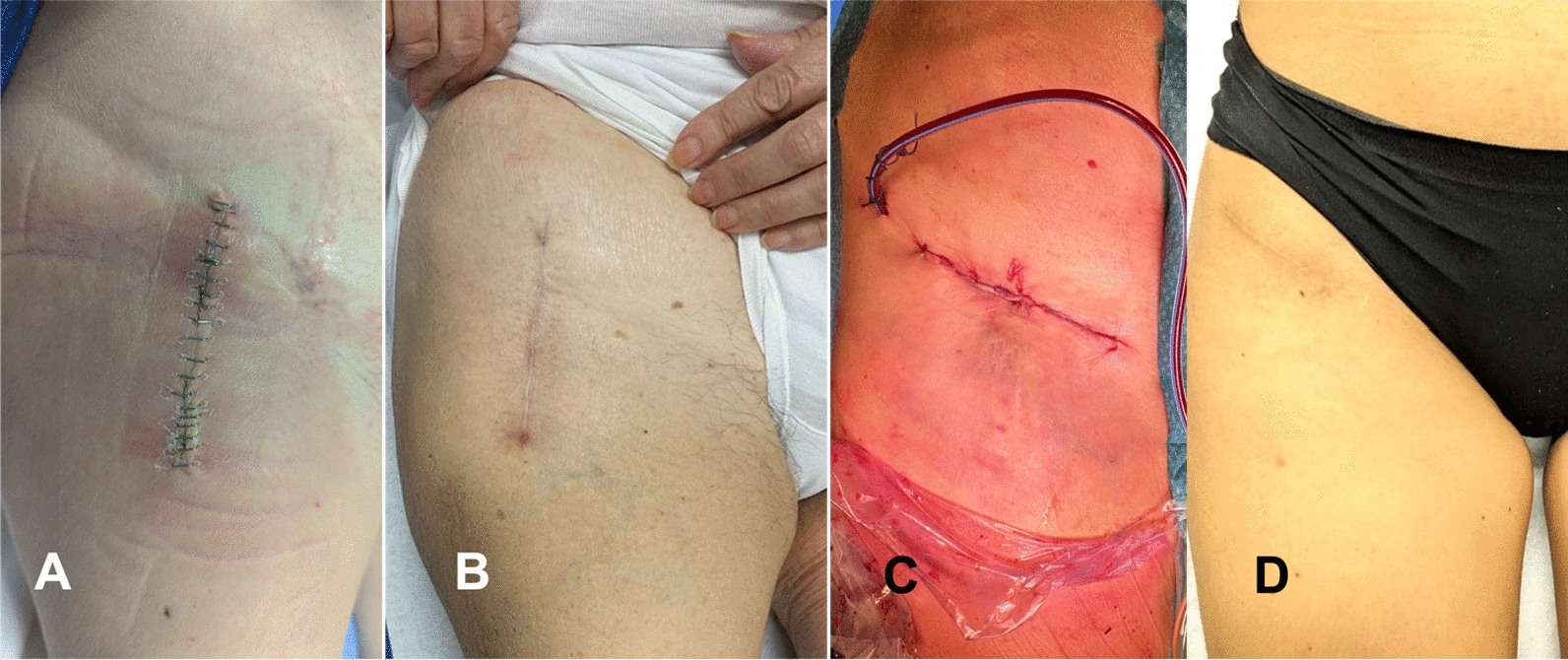
Consistent with previous reports, preoperative patients were concerned about safety, whereas postoperative concerns shifted to cosmetic outcome and satisfaction. The shift in patient demands for surgery is like a fast-food experience with an emphasis on speed, predictability, and control. We found a positive correlation between the mini-open approach and MIPO technique and better satisfaction with scar appearance, scar length, and overall satisfaction. This was confirmed clinically and statistically compared with the conventional ORIF group. However, the surgeon’s skill in wound closure techniques and understanding of patient skin type and healing characteristics contribute to cosmetic improvement in midshaft clavicle surgeries.
A displaced midclavicle with simple or comminuted anatomy is a good indicator of mini-open with MIPO. In this study, we used mini-incisions at the fracture site which are often helpful for anatomical reduction. This can aid in butterfly bone fragments resting well on the parent bone without extensive soft tissue stripping, as in ORIF. This causes a smaller fracture gap and a lower nonunion rate. On failing to do so, the situation can be contrary, and the resorption of free fragments can lead to nonunion. However, in our study, we did not encounter nonunion cases owing to meticulous precautions during dissection.
In this study, both treatments were performed using a precontoured anatomic locking plate. In most patients, anatomical locking plates are designed to perfectly fit on the superior surface of the clavicle [23]. The plate used acts as a bridging fixation, even in comminuted fractures. In addition, they provide angular stability to S-shaped bone when threaded screws are added to the plate, with little effect on comminuted biocircumstances [24,25,26]. Moreover, eliminating plate contouring minimizes the risk of plate fatigue breakage and the intraoperative time. Therefore, we did not encounter symptomatic hardware irritation leading to plate removal using the MIPO technique.
In contrast, absolute anatomical reduction, direct manipulation, and fracture site assessment are often restricted in comminuted and wedge-shaped fractures. Owing to these demanding technical requirements, greater radiation exposure, and strict control over the fracture site, MIPO has some inequity. However, this new technique is reliable, has many postoperative benefits, and acts as a bridge plate for shaft fractures of the clavicle.
There were some limitations to the study design. This retrospective observational study did not include standard follow-up period between the two groups or different patients. In addition, we were not able to implement rigorous patient selection criteria during the survey. Despite this, the average follow-up intervals between the two groups were similar, providing a valid comparison. This study aimed to establish the subjective experiences of skin numbness using objective functional scores. We could not conduct quantitative sensory testing through nerve conduction studies for precise results as it may require comprehensive examination, equipment, and cost of the study. This study relied on the memory of prior events and experiences for the questionnaire scoring system, which can be biased. Prospective studies should be conducted in the future to improve the clinical research quality. This study adds to the growing literature on displaced clavicular fractures and provides a reference for MIPO.






Comments (0)