
Remember me





This study was designed as a single-center parallel randomized controlled open-label trial. The ethical approval for the study protocol was obtained from the Ethics Committee of Damascus University (date: 9/5/2022/no: 2609). The study was registered at the International Standard Randomized Controlled Trial, registration number: ISRCTN11661014.
(https://www.isrctn.com/ISRCTN11661014). Informed consent for participating in the study was obtained from every patient.
Participants were randomly allocated into two groups using a simple randomization method, where each participant drew sealed, opaque envelopes from a box (n: 10; n: 10); each envelope contains a numbered paper (1 or 2). Twenty patients were randomized; the same patients were analyzed. No changes were made to methods after trial commencement.
Consent for publicationA prospective study was undertaken; the sample size calculation was performed using G*Power version 3.1.9.4, to detect different amounts of gingival display between groups [12], assuming a large effect size (Cohen’s d = 0.8), a significance level (α) of 0.05, and a desired power of ≥ 0.80. Based on these parameters, the minimum required sample size was determined to be 16 participants (8 per group). To enhance the statistical robustness of the study and account for potential dropouts or variability, the sample size was increased to 20 participants (10 per group). The predicted sample size was 16, 8 patients in each group. Based on these results, we have selected a sample size of 20, 10 in each group; all of them were presented to our department at the university or referred from other departments between 2022 and 2024, with a chief complaint of an unpleasing smile, to 2 times more than the natural distance, which is 6–8 mm.
Following a discussion of the procedure, its pros and cons, and potential postsurgical expectations, patients received an initial consultation on eligibility and ensured that their condition met the inclusion criteria. This involved analyzing smile dimensions to exclude dentoalveolar origin, measuring clinical crown lengths of the teeth to rule out short clinical crowns as a factor. This was done by placing a periodontal probe at the midpoint of the buccal surface of each tooth, parallel to its longitudinal axis, and recording the distance in millimeters between the gingival margin and the incisal edge. Dividing the face into three equal parts checks for imbalance. Standardized photographs and cephalometric images were also taken to rule out skeletal causes and to ensure the EGD case was of soft-tissue nature. Key anatomical landmarks, such as maxillary height and the SNA angle, were analyzed. The SNA angle, which normally measures around 82°, is formed by 3 points in which (S) is the center of the sella turcica, (N) is the most anterior point of the nasofrontal suture, and (A) is the most posterior point on the anterior maxillary surface. Upper lip hypermobility was assessed by measuring lip movements from the rest to the maximal smile positions. Lip elevator muscles were considered hyperactive when their elevation was between 6 and 8 mm from the rest position. All patients chose lip repositioning surgery.
Participant selectionInclusion criteria 1.Adult patients aged between 18 and 38 years
2.Good periodontal health based on clinical examination (no periodontal pockets, no bleeding, healthy gingival appearance)
3.Systemically healthy individuals, classified as ASA physical status I or II (i.e., patients without systemic disease or with mild, well-controlled systemic conditions)
4.Excessive gingival display ranging between 4 and 6 mm caused by a short or hyperactive upper lip.
Exclusion criteria 1.Smokers.
2.Pregnant or lactating women.
3.Vertical maxillary excess of more than 6 mm.
4.Systemic disease or cases that forbid local anesthesia.
The sample of 20 patients was randomly assigned to one of two groups; each patient was asked to choose a piece of paper numbered 1 or 2, for which the first one referred to Group no. 1: 10 patients with EGD, treated with lip repositioning surgery by removing a partial thickness flap utilizing the conventional scalpel. Number 2 referred to Group no. 2: 10 patients with EGD, treated with lip repositioning surgery by removing a partial thickness flap utilizing the CO2 laser (CO2 laser; E301, Beijing, China, wavelength 10.600 nm).
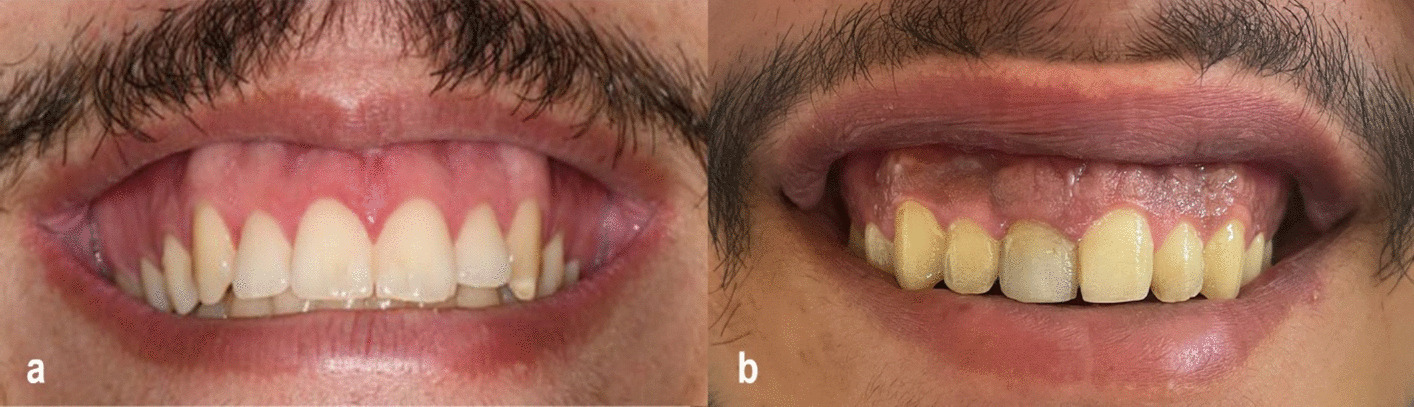
An informed consent was obtained from each patient, irrespective of which group. Prior to surgery, intra- and extraoral photographs were taken using a 7500D Nikon camera (Nikon, Tokyo, Japan), and all measurements were recorded (Fig. 1a, b).
Fig. 1
a Preoperative photograph of a patient from the CO₂ laser group demonstrating excessive gingival display (4–6 mm) during maximal smile prior to lip repositioning surgery. b Preoperative photograph of a patient from the conventional scalpel group showing excessive gingival display (4–6 mm) during maximal smile before undergoing lip repositioning surgery
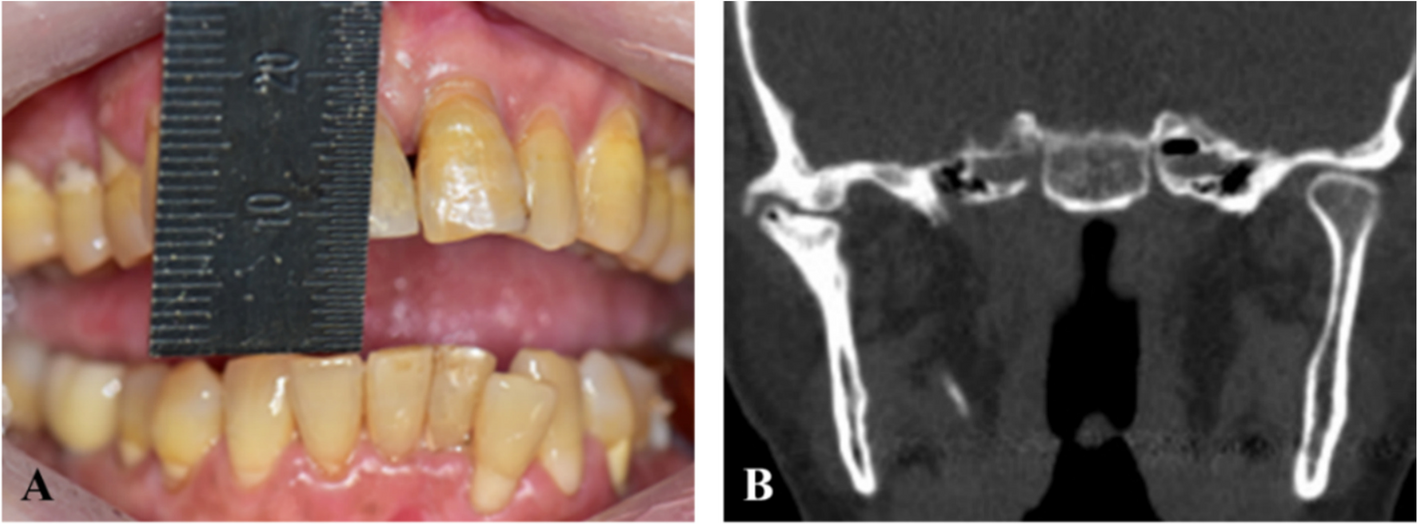
The amount of exposed gingiva was recorded using a gingival probe. Following several previous studies, measurements were taken from the inferior border of the upper lip to the zenith point on the gingival margin, starting at the central incisors and ending at the second premolars on each side. Assessments were performed before surgery and at 1, 3, and 6 months postoperatively [13]. A custom-made appliance with a hollow midpoint and horizontal extraoral arm was fabricated after taking an impression of the maxillary teeth for each patient. A sterile millimetric graduated ruler was inserted vertically into the hollow part of the appliance to ensure consistent measurements; this technique was developed to guarantee measuring the upper lip length from the same position before surgery. In all the recall appointments, patients were instructed to bite in normal occlusion. The external upper lip length was recorded both at rest and maximal smile, preoperatively, and at 1-, 3-, and 6-month post-operation (Fig. 2a, b).
Fig. 2
a Measurement of external upper lip length during smile using a custom-designed ruler to ensure consistent positioning in a CO₂ laser group patient. b Measurement of external upper lip length during smile using the same custom-designed ruler in a conventional scalpel group patient
The internal upper lip length (vestibular depth) was also recorded clinically using a specially designed graduated ruler with a hollow midpoint, which allowed exclusion of the upper labial frenum and ensured consistent positioning for measuring [14].
InterventionOperative procedurePrior to surgery, both external and internal oral tissues were disinfected with 2.0% chlorhexidine solution and 0.12% chlorhexidine rinse for 1 min. Local anesthesia was administered by infraorbital infiltration injection in both sides using 2% lidocaine with 1:80,000 epinephrine.
The surgical procedure involved marking the incision lines on the dry mucosa in each patient using a sterile surgical marking pen (Fig. 3a, b).
Fig. 3
a Intraoperative marking of the surgical flap in a CO₂ laser group patient. The inferior incision is made 1 mm apical to the mucogingival junction; the superior incision is 10–12 mm above and parallel to the first. b Intraoperative marking of the surgical flap in a conventional scalpel group patient. The inferior incision is made 1 mm apical to the mucogingival junction; the superior incision is 10–12 mm above and parallel to the first
A horizontal partial-thickness incision, extending from the mesial line of the right maxillary second premolar to the left maxillary second premolar, was made 1 mm coronal to the mucogingival junction (MGJ); a V-shaped incision was made in the upper lip frenum area to facilitate guaranteeing labial midline position with punctual lip symmetry and accurate closure.
A second horizontal incision was then made in the labial mucosa, positioned approximately 10 to 12 mm apical to the first incision. Finally, the two incisions were connected at the mesial line angles of the right maxillary first molar in an oval shape (Fig. 4a, b), and.
Fig. 4
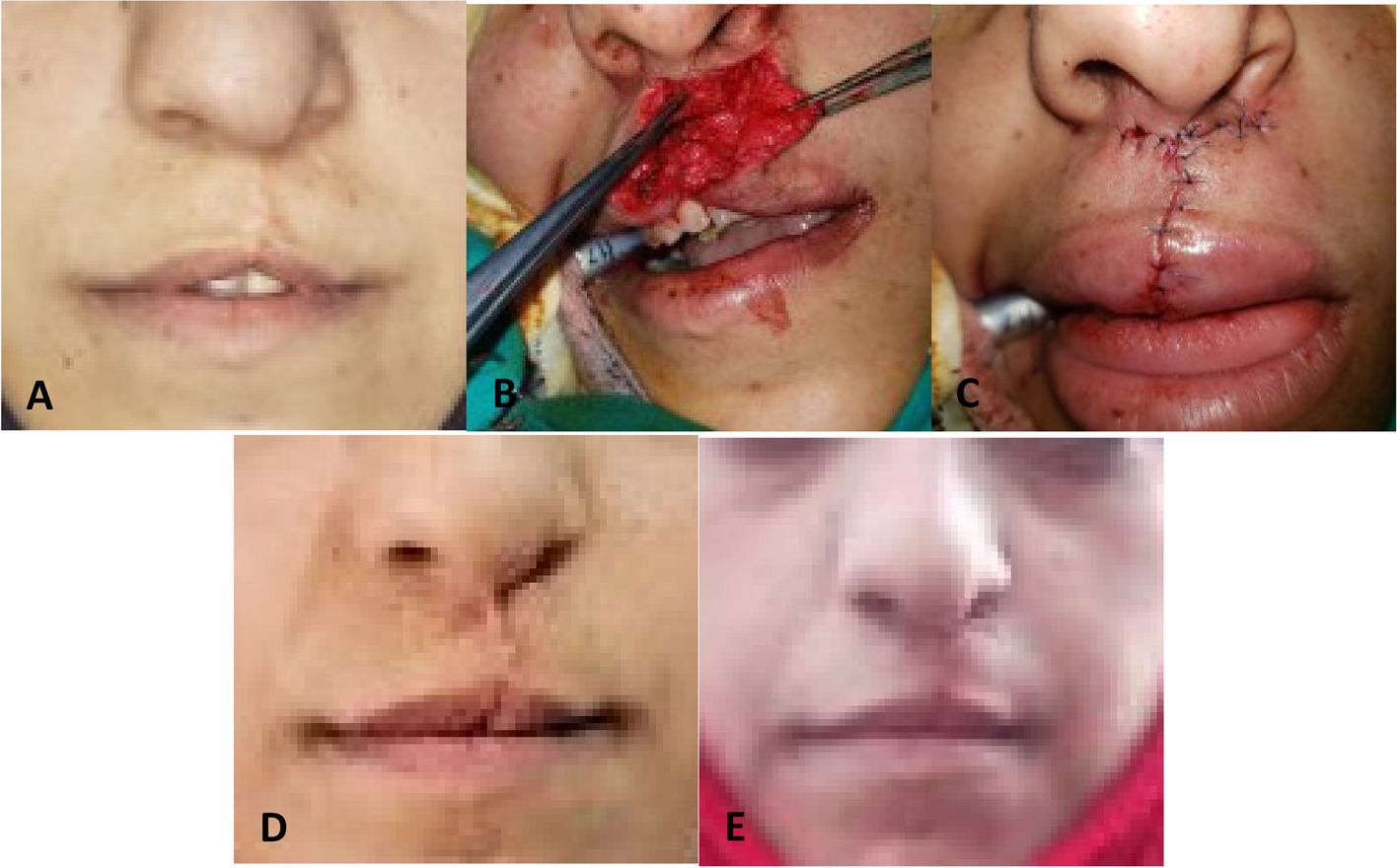
a Post-flap removal view in a CO₂ laser group case showing a clean surgical field with minimal bleeding due to laser-induced hemostasis. b Post-flap removal view in a conventional scalpel group case demonstrates noticeable bleeding due to the high vascularity of the upper lip region
then a strip of mucosa was fully removed (Fig. 5a, b).
Fig. 5
a A strip of mucosa removed using a CO₂ laser as part of the partial-thickness flap technique. b A strip of mucosa removed using a conventional scalpel in the corresponding group
In Group 1, all previous surgical steps were performed using a Bard-Parker no. 15 stainless steel scalpel blade.
The same surgical technique was performed in Group no. 2 utilizing the CO2 laser. All the clinical staff were aware of laser safety measures (controlled area, wavelength-specific eyewear) and the wearing of high-filtration face masks to address the laser surgical plume. A laser test fire was performed to determine beam patency.
Laser operating parameters were as follows:
Wavelength
10,600 nm
Application
Non-contact
Emission mode
Super pulsed
Pulse width
300 µs
Pulse interval
500 µs
Frequency
1250 Hz
Beam spot size
0.5 mm (sq. cm)
Average power
2.2 W
Peak power
6 W
CO₂ laser emission modeIn some laser systems, the super pulsed mode refers to the emission of very short, high-frequency pulses generated by modulating the electrical pumping mechanism. Unlike gated or chopped modes, often inaccurately referred to as “pulsed” true super pulsed lasers can achieve high peak power and power density while maintaining low average power. This enables deeper energy penetration into tissues with minimal thermal buildup, making super pulsed lasers particularly suitable for precise and controlled surgical applications. Some devices also allow the emission of grouped pulses, known as pulse trains, further enhancing energy delivery efficiency [11]. The surgical procedure involved applying the laser beam at the outlined borders of the proposed flap in order to reduce the tension and make the mucosal strip dissection smoother; the laser beam was then advanced along the oval-shaped line from the first side, adopting a 45° angled handpiece and with normal hand speed in order not to cut the strip or deepen the flap.
Laser-tissue distance was maintained by the laser hand-piece spacer. Once the tissue strip had been removed, a no. 15 scalpel blade was used in gentle peeling movements; hence, a slight amount of bleeding was induced at this stage to accelerate the healing process; hitherto, surgical field visualization and hemostasis through laser use had been maintained.
In both groups, after the strip had been removed, a durable suturing was performed starting with a guiding suture in the midline area, indicated by a V-shaped index in the middle of the flap. Two further sutures were placed in the canine area on each side to assist in achieving reliable lip symmetry and ensure proper alignment of the lip midline with the teeth. Several interrupted 0000 silk sutures were used to close the rest of the wound area and to stabilize the upper lip in its new position (Fig. 6a, b).
Fig. 6
a Suturing of wound margins in a CO₂ laser group patient using 4–0 silk sutures in an interrupted technique. b Suturing of wound margins in a conventional scalpel group patient using the same interrupted technique with 4–0 silk sutures
A postoperative written prescription was given to each patient:
(i)Nonsteroidal anti-inflammatory drugs (ibuprofen 400 mg was administered four times daily for 2 days).
(ii)A total of 0.12% chlorhexidine mouthrinse (rinsing two times for 30 s per day, for 1 week).
Postoperative instructions A)Patients were instructed to apply ice packs over the upper lip intermittently for several hours post-surgery.
B)Stick to soft food for the first week and avoid any activities that could cause mechanical trauma to the surgical area.
C)Prevent wide smiling and minimize lip movement when talking for the first 2 weeks after surgery.
D)Avoid brushing around the wound for 2 weeks.
E)Take prescribed analgesics to manage any postoperative pain and, if ineffective, ask your dentist.
F)Sutures to be removed after 14 days.
Postoperative assessmentFollow-upThe intensity of postoperative pain was recorded 24 h after surgery by asking patients to choose a number from 0 to 10 on a Numeric Pain Intensity Scale which is a type of VAS (visual analog scale), where 0 refers to no pain, 1–3 mild pain, 4–6 moderate pain, and 7–10 severe pain [15]. Pain level was recorded at a single time point based on previous studies indicating that VAS is not linear and does not accurately track changes in pain intensity over time [16].
Postsurgical edema usually peaks on the third day post-operation before starting to subside by day 4 [17,18,19,20]. The occurrence of edema was assessed at its peak on the third day postoperatively and on day 7 by recording “Yes” if edema was present or “No” if absent. Edema was observed in all patients of both groups on day 3 and was absent on day 7, with visually noticeable differences between the groups. Since this is the first randomized controlled clinical trial comparing CO₂ laser and scalpel techniques in this surgery, we recommend future researchers to study these differences quantitatively or volumetrically for a more precise understanding.
The amount of exposed gingiva, the upper lip’s external and internal length, was recorded according to the same methods used in the diagnosis appointment.
Patients were followed up within 1-, 3-, and 6-month post-surgery (Fig. 7a, b), all the measurements were recorded by the same examiner (the researcher), and clinical photographs were taken at all follow-up appointments.
Fig. 7
a Six-month follow-up in a CO₂ laser group patient showing an esthetically improved gingival display during maximal smile. b Six-month follow-up in a conventional scalpel group patient demonstrating significant improvement in gingival display during maximal smile
Statistical analysisThe Statistical Package for the Social Sciences (SPSS) was used, version 25, to analyze the data as follows:
Descriptive statistics: By displaying the mean and standard deviation of the variables according to the two study groups.
Normal distribution test: Using the Shapiro–Wilk test when the sample size is smaller than 50 in order to find out the most appropriate tests for the study
Difference tests: The independent T-test and its nonparametric alternative, the Mann–Whitney test, to study the differences between the two groups in the study variables; the paired samples T-test and its nonparametric alternative, the Wilcoxon signed-ranks test, for comparisons over time within the same group; and the analysis of variance for repeated measures and its nonparametric alternative, the Friedman test, to confirm the presence of significant differences in the studied group over time.
The testing was performed at pre-set alpha of 0.05, meaning that a significant difference exists with 95% confidence.
Comments (0)