The present study demonstrated that a ML algorithm trained with CMR left ventricular, left atrial, and right ventricular quantified strain and general cardiac functions could distinguish patients with ICM accurately from those with patients with NICM.
The major advantage of this novel ML approach is obviating the need for contrast media administration thus enhancing patient tolerability and shortening scan time at a lower cost.
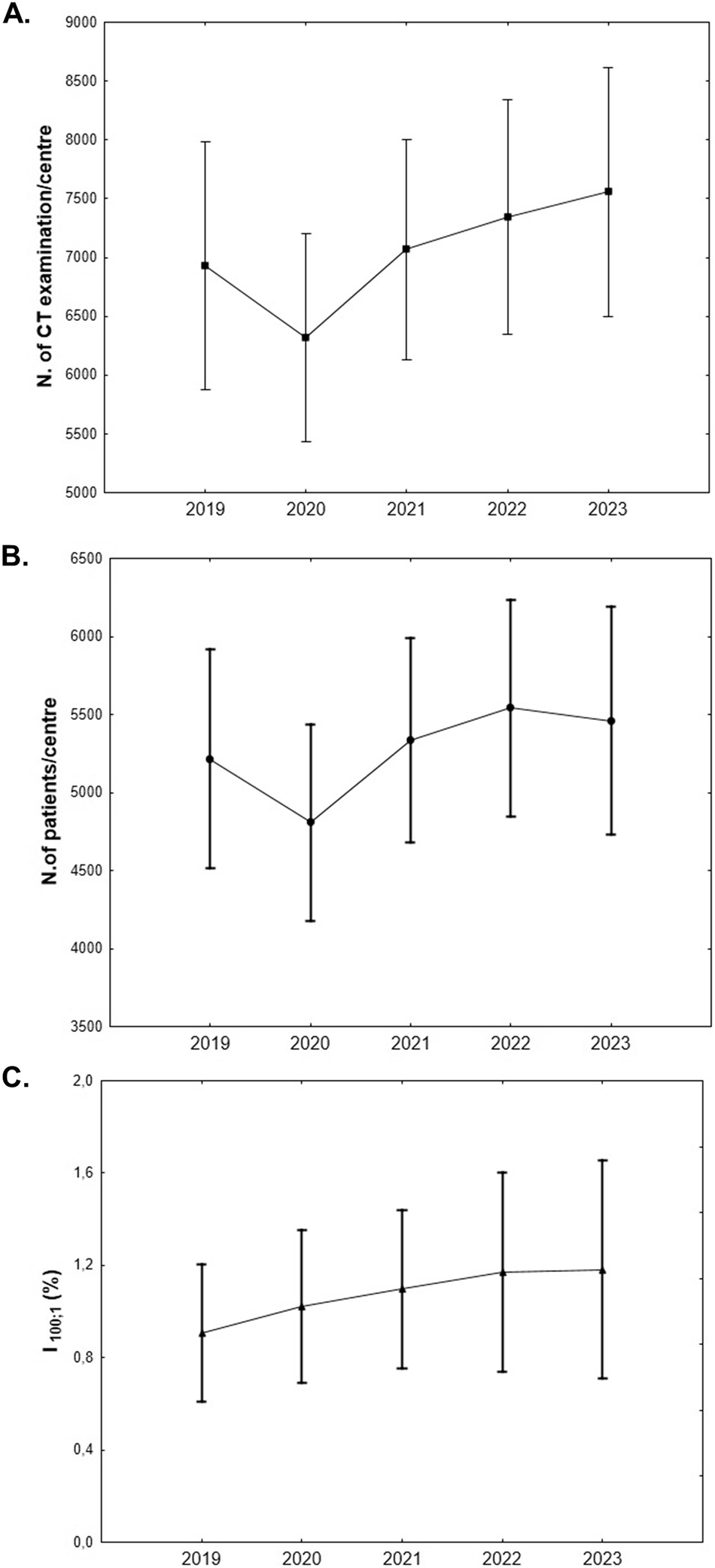
In clinical practice, the exponential increase in CMR examinations may necessitate the optimization of clinical workflows with faster and more cost-effective CMR protocols. Furthermore, individuals who are ineligible for contrast media administration and have a limited tolerance for CMR examinations may find shorter, non-contrast CMR examinations advantageous. Non-contrast CMR imaging improves the applicability of CMR examinations and offers greater patient comfort and can lower costs [12].
Several authors have explored the diagnostic capability of non-contrast cine-CMR images using ML-based models as an alternative to LGE images [11, 13, 21,22,23]. Avard et al explored a ML algorithm and radiomics features to differentiate myocardial infarction and normal cases on non-contrast cine-CMR images showing that the AI-based model yielded optimal results with an AUC of 0.93 [10]. Similarly, Larroza et al utilized a support vector machine classifier to explore the potential of texture analysis with cine-CMR images in distinguishing between infarcted nonviable, viable, and remote segments. The results showed that texture analysis could effectively detect non-viable segments on non-contrast cine-CMR images, achieving an impressive AUC of 0.849 and a sensitivity of 92% [11]. Conversely, Zhang et al evaluated virtual native enhancement combining cine-CMR images and native T1 mapping to produce LGE-like images. This approach used a deep learning model achieving a strong correlation with LGE in quantifying scar size and transmurality with an accuracy, specificity, and sensitivity of 84%, 100%, and 77%, respectively [12].
Previous ML-based cine-CMR research focused on the application of radiomics analysis, which requires time-consuming quantitative post-processing image analysis or the acquisition of additional CMR sequences, leading to longer CMR examinations.
To the best of our knowledge, this is the first work focused on a ML-based model that includes cine-CMR parameters to discriminate between ICM and NICM. Previous work investigating myocardial strain-derived parameters to determine the etiology of heart failure have focused on the analysis of a single cardiac chamber or on radiomics analysis [10, 13, 23,24,25]. The present study has a retrospective study design and a single-center data collection approach. The retrospective analysis enables to harness a substantial dataset of CMR cases, encompassing a significant timeframe, which is essential for training and validating a robust ML model. Additionally, the decision to focus on a single center offered a dataset characterized by consistency and homogeneity in relation to imaging protocols and CMR scanner which contributes to reducing potential variability and confounding factors.
The current study simultaneously analyzed multiple cardiac chambers using an ML algorithm. The physiological “communication” between cardiac chambers may be too complex to be captured using the traditional regression models. A ML-based model for assessing the relationship between cardiac chambers interaction can overcome some limitations of common regression techniques.
In the features importance analysis, ventricular and left atrial strain parameters presented the most discriminative value in discriminating between ICM and NICM.
In fact, NICM tends to show global myocardial fiber dysfunction involving both ventricles in comparison with ICM that shows a more regional dysfunction [26]. The contribution of circumferential and radial strain parameters in discriminating ICM from NICM seen in the current study is explained by the different effects on subepicardial and transmural fiber by myocyte injuries.
Indeed, the myocardium is composed of three layers of fibers, namely (1) subendocardial fibers acting on longitudinal shortening, (2) subepicardial fibers acting on circumferential shortening, and (3) transmural fibers acting on radial shortening [27, 28].
The pathophysiology of myocardial infarction is characterized by a waveform appearance from the subendocardium to the epicardial layer. Therefore, the subendocardial fibers are the earliest myocardium layers involved in ischemia [28, 29]. In addition, it has been suggested that impairment in the contraction of longitudinal fiber in ICM is compensated by the augmentation of the other layers [29, 30]. Similarly, the RV strain parameters’ impact in discriminating between ICM and NICM demonstrated in the present study may relate to the ventricular interaction through the interventricular septum [31]. Indeed, the RV shares oblique fibers with the LV in the interventricular septum. In the RV contraction, the oblique septal fibers are more efficient than the free wall transverse fibers and consequently, LV remodeling leads to septal fibers dysfunction impairing RV contraction [32].
Another hypothesis suggested is an intrinsic injury of the RV myocardium in NICM patient [33]. Due to the anatomical connection of the ventricle and atrium, their contribution to differentiate ICM and NICM is expected in this model. The LA strain parameters more relevant in the proposed model are reservoir and conduit strain rate parameters reflecting LA expansibility and stiffness.
In patients with LV dysfunction, LA contraction rises to maintain optimal LV filling. Consequently, early in ventricular dysfunction LA pump function is increased but LA stiffness augmented, and work mismatch occurs. Subsequently, LA pump function decreases as a result of the progression of LV dysfunction due to the increased afterload imposed on the LA [7, 34]. In addition, some authors suggested a direct myopathic involvement of the LA myocardium in various NICM [22, 35, 36].
Practical advantages
The aim of the current study was to investigate the capability of an ML algorithm using cardiac function, volumes, and atrial and ventricular strain features from cine-CMR in discriminating ischemic from non-ischemic etiologies. Using cine-CMR features could potentially avoid the contrast media administration and increase the clinical availability of CMR examinations allowing increased accessibility to CMR examinations achieved through reduced costs and faster imaging acquisition.
Limitations
The following study limitations should be acknowledged and addressed in future research before the presented method can be employed in clinical practice. First, the relatively small sample size was evaluated with a single CMR scanner and the retrospective single-center observational design of the study with no external validation dataset. Although we have taken precautions to mitigate the challenges posed by the limited dataset, the sample size and single-center study design could potentially impact the generalizability to more diverse populations, encompassing variations in race, medications, and other factors. To confirm the robustness of the present findings, future multi-center studies are prompted to facilitate the incorporation of larger, more varied datasets, bolstering the reliability and broader applicability of the proposed approach. Even though the purpose of the study was to evaluate an AI model to discriminate between ICM and NICM, and thus required a heterogenous NICM cohort, the composition of the evaluated population might be influenced by statistical variations as may the subsequent results.
Second, although we have taken precautions when training models and estimating generalization performance, this model may still suffer from overfitting. To guard against overfitting, we employed cross-validation to select features with diagnostic value, train algorithms, calibrate predicted probabilities, and evaluate performance on the same cohort, by considering non-overlapping subsets of the data and thus reducing the bias in performance estimation.
Finally, in the current study, the predictive value of strain and parametric mapping parameters for adverse cardiovascular events was not assessed at follow-up. The promising results could prompt further prospective trials including a larger number of patients to confirm the present findings. However, implementing non-contrast AI models into real-world clinical practices poses considerable challenges, including the lack of transparency and interpretability of AI models, the needed of a large amount of annotated data from different centers, as well as ethical and legal issue. The derivation of an effective non-contrast ML model that can be applied to the real-world clinical practice would require a considerably larger training group across different centers and patient groups and its validation would require an independent validation cohort. Furthermore, the development of a privacy protection algorithm is essential, which should integrate encryption and AI techniques to achieve secure and generalizable non-contrast AI models.




Comments (0)