
Remember me


This study (named ‘Inside study’) is a double-blind, randomised, placebo-controlled, multi-centre trial. We aim to enrol 198 children, aged between 1 and 5 years, with FC according to the Rome IV criteria (Table 1).
Study settingThis study is coordinated by Wageningen University & Research, Laboratory of Microbiology. The study is conducted in The Netherlands. Patients from the outpatient clinics in the Emma Children’s Hospital, Amsterdam, Amsterdam University Medical Centres Amsterdam (AUMC), DeKinderKliniek Almere, Spaarne Gasthuis Haarlem, Haaglanden MC Den Haag, Rijnstate ziekenhuis Arnhem and Maasstad ziekenhuis Rotterdam, will be recruited by their treating paediatric gastroenterologist. More participating centres may follow.
Eligibility criteriaParticipant screeningEligible patients will be contacted by researchers of Wageningen University & Research to answer questions the patients might have and to verify whether or not they are willing to participate, to avoid an undesirable dependency situation with the treating paediatric gastroenterologist.
Inclusion criteriaIn order to be eligible to participate in this study, a subject must meet all of the following criteria, as considered by a medical doctor:
Written informed consent obtained from parents or guardians of children meeting the eligibility criteria and those willing to comply with the requirements of the study.
Aged 1–5 years (12 to 72 months at the day of inclusion).
Children that meet/fulfil the Rome IV criteria for FC.
Exclusion criteriaAny of the following criteria will result in exclusion of a potential subject from this study:
Children who suffer from any GI complaints other than FC, known structural GI abnormalities, or previous GI surgery.
Any condition that would make it unsafe for the child to participate. This can include developmental delays associated with musculoskeletal or neurologic conditions affecting the GI tract. Children with an underlying cause of defecation disorder (for example, Hirschsprung’s disease, spina bifida occulta, cystic fibrosis, or GI malformations).
Children with clinically significant cardiac, vascular, liver, pulmonary, psychiatric disorders, severe renal insufficiency, human immunodeficiency virus, acquired immunodeficiency syndrome, hepatitis B or C or known abnormalities of haematology, urinalysis, or blood biochemistry, as checked by the inclusion questionnaire.
Children who are lactose intolerant, or who are self-perceived lactose intolerant or for whom it is expected that low doses of lactose could lead to GI symptoms.
Children who are allergic to cow’s milk or fish.
Use of antibiotics or other medicines or food supplements, and breast milk-feeding, which can influence defecation and gut microbiota 4 weeks prior to the study run-in period and during the study itself.
The use of infant formula, follow-on formula, young child formula in the previous week prior to the study run-in period and during the study itself.
Children on other supplements/medication that could affect bowel function, including e.g. fibre supplements, and pre-, pro- and synbiotics (excluding rescue medication) for the past 4 weeks and during the study itself.
Children that participate in another clinical trial.
Informed consent procedureInformed consent will be obtained by the researchers or treating paediatric gastroenterologist either at one of the outpatient clinics or at a home visit before the start of the study, see Additional file 1.
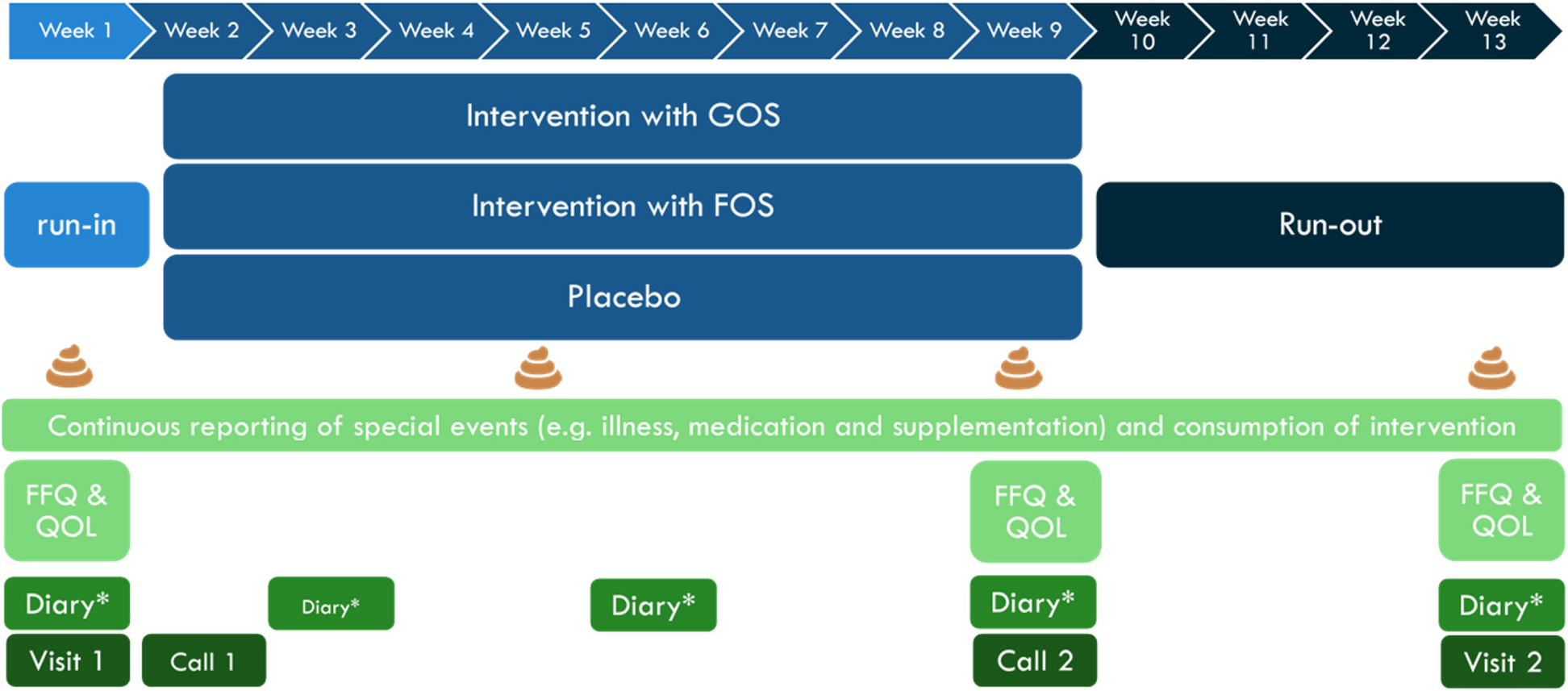
InterventionsAfter the run-in period, participants will receive either Vivinal® GOS powder (FrieslandCampina, Amersfoort, The Netherlands), Frutalose® OFP chicory oligofructose (Sensus, Roosendaal, The Netherlands) or placebo (maltodextrin) supplements in tins with scoops. The substances are approved food grade ingredients, they have been previously used in other clinical trials and are used in several food products. All supplements were similarly powders light in colour with a pleasant taste. All supplements are in identical tins with scoops and were produced according to good manufacturing practice standards. One scoop (8.5 mL size) should be consumed per day, with half a dose in the first 3 days to avoid any potential side effects such as flatulence caused by intestinal fermentation of FOS or GOS. The product should preferably be dissolved in warm or cold drinks such as milk or semi-solid products such as yoghurt. The intervention product will be consumed for 8 weeks (Fig. 1).
Fig. 1
Study protocol flow. Visit 1 is at day = 1, call 1 at day = 7, call 2 at day = 63 (end of 9 weeks), visit 2 at day = 91 (end of 14 weeks), which will be a home visit to pick up samples and leftover product. During visits 1 and 2, anthropometrics (weight, height and head circumference) will be measured. *Diary includes filling out stool consistency and frequency and compliance of taking the study product. FFQ, food frequency questionnaire; FOS, chicory fructo-oligosaccharides; GOS, galacto-oligosaccharides; QOL, quality of life questionnaire
Rescue medication should be used if the participant does not have a bowel movement for 3 consecutive days, being either microlax 5 mL, sodium picosulphate pearls (1 droplet per 5 kg body mass) or glycerine (glycerol) suppositories (1 g, 2 g or 4 g). These types of laxatives were chosen as they have a mode of action based on provoking peristalsis, and thereby are expected to have minimal effect on gut microbiota composition [31]. This is in contrast to (fermentable) osmotic laxatives such as lactulose or PEG, which were found to influence gut microbiota composition [32].
Despite that rescue medication may be required, the child will still remain in the study. Each use of rescue medication needs to be reported in the diary to differentiate between spontaneous bowel movements and those related to rescue medication use. To further exclude an influence of escape medication on gut microbiota outcomes, a stool sample should only be collected after a spontaneous defecation and at least 3 days after the last use of escape medication.
OutcomesPrimary objectiveThe main study parameter is the change in stool consistency, measured by the validated Dutch-modified Bristol Stool Form Scale (mBSFS) [33]. This will be the mean difference in stool consistency of GOS versus placebo and FOS versus placebo at all time points (week 1, 3, 6, 9 and 13) and from baseline to week 9.
Secondary objectivesThe secondary study parameters will be:
Changes in stool frequency between groups and over time.
Changes in stool consistency in the number of cases in a certain score of the mBSFS, as percentages.
Tertiary objectivesPainful defecation.
Meeting the Rome IV criteria at baseline, week 9 and week 13.
Quality of life of the child, measured by the TAPQOL [34].
GI symptoms, such as flatulence and bloating.
Gut microbiome:
◦ Total faecal microbiota composition, as measured by 16S ribosomal RNA (rRNA) gene sequencing
◦ Faecal abundance of specific genera/species as measured by quantitative PCR analysis.
◦ Faecal pH and faecal concentration of fermentation products such as short-chain and branched-chain fatty acids.
◦ Correlations between stool characteristics and gut microbiota composition, faecal pH or fermentation products.
Use of rescue medication.
Faecal incontinence (only for completely potty-trained children).
The amount of GOS, FOS or placebo supplement consumed, as an indication of compliance, measured in both diaries as well as weighing the tins after the trial.
Anthropometrics: weight, height and head circumference measured at baseline and the close-out visit after week 13.
Anthropometrics: weight, height and head circumference measured at baseline and the close-out visit after week 13.
Dietary intake, as measured by a food frequency questionnaire.
Participant timelineAfter randomisation, patients will enter a 1-week run-in period, after which they will either receive GOS, FOS or a placebo for 8 weeks. Lastly, a 4-week run-out period is in place to investigate whether a possible effect lasts or not. The flow of the study protocol is presented in Fig. 1.
Sample sizeA sample size calculation was performed for stool consistency on a scale from 1 to 5. We used the sample size formula n = 2 × (Zα + Zβ)2 × (SD/D)2 per group. Using a probability α = 0.05 and a power (1-ß) of 80%, the formula simplifies to n = 2 × 7.9 × (SD/D)2 per group.
The effect sizes of GOS and FOS versus placebo were estimated based on a study by Closa-Monasterolo et al. who investigated the effect of a mix of chicory inulin with FOS on stool consistency in functionally constipated children aged 2–5 years [26]. Based on these data, an effect size of 0.35 was chosen, with an SD of 0.65. This results in a group size of 54.5. The total number of children to be recruited is 198, that is, 66 per arm assuming a drop-out rate of 20%.
Assignment of interventions: allocation and blindingRandomisation is done by a computerised random-number generator in the Electronic Data Capture system Castor EDC via a variable block randomisation of block sizes of 6 and 12, not stratified per centre, to one of the three intervention arms [35]. For the study product, two codes per treatment arm, each consisting of two letters and one number were made and printed on the bottom of the cans. The list linking these codes to GOS, FOS or the placebo is only known by two people who are not involved in this study; one at Wageningen University & Research and one at FrieslandCampina. Therefore, the study can be conducted fully blinded for all parties involved. In case of an emergency, the study treatment can be unblinded after consultation with the principal investigator at Wageningen University & Research.
Comments (0)