
Remember me


The study was done in accordance with the Declaration of Helsinki and approved by Research Review and Ethics committee of MAHSA University, Malaysia (RMC/AL02/2017). The Consolidated Standards of Reporting Trials (CONSORT) checklist is available as supporting information. The trial was posted on 25/07/2019 at ClinicalTrials.gov and its identifier is NCT04032548. All participants gave written informed consent, and they were informed about the details of procedure, risks, and benefits of the study.
Study designA single-centre, Latin-square cross-over, double masked (investigators and statisticians), randomized controlled clinical trial was conducted to assess the effectiveness of propolis mouthwash on chronic generalized gingivitis. In latin square cross-over design, each participant is treated as a block, which helps to control for individual differences that could impact the gingival and plaque scores of the study. The sequential order of the study protocol followed in the present study is shown in Fig. 1.
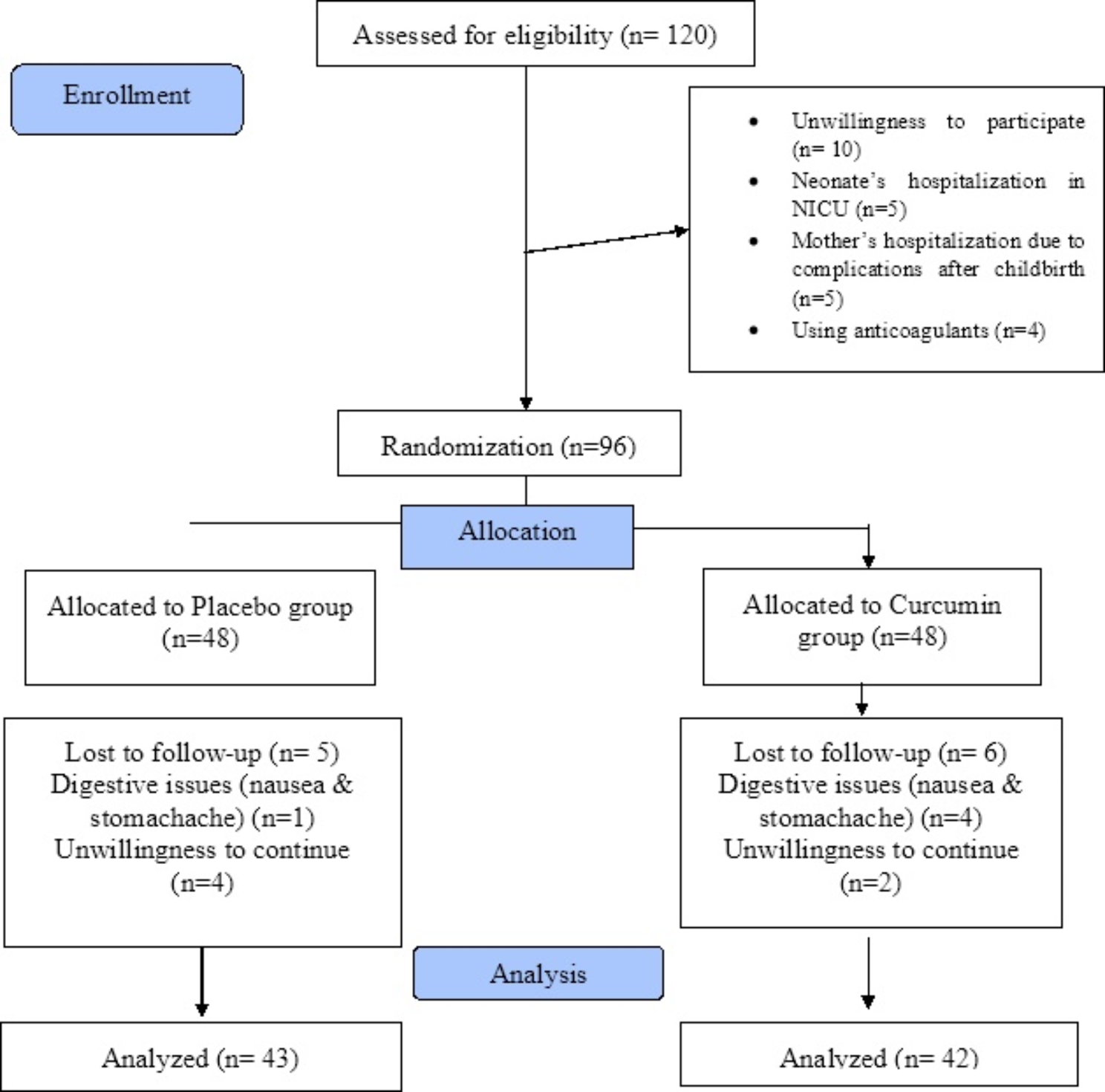
Fig. 1
Flow chart of study participants in each phase
Study population and selection criteriaSubjects were recruited between March 2019 to June 2019. The follow-up visit of the last subject was completed in December 2019. A total of 124 subjects were screened and assessed for eligibility (49 did not meet the inclusion criteria, 30 subjects declined to participate). Forty-five subjects (30 females and 15 males) who met the inclusion criteria, gave consent to participate were recruited from dental clinic of MAHSA University. Adults age range of 18–30 years were enrolled if they have the following inclusion criteria: (1) good systemic health, (2) Gingival index > 1 (3) Periodontal pocket depth ≤ 3 mm (4) Clinical attachment loss “0” (5) Provision of written informed consent. Exclusion criteria were: (1) Severe periodontal disease, as characterized by purulent exudates, generalized mobility, and/or severe recession (2) Any condition that requires antibiotic premedication for the administration of a dental prophylaxis (3) Self-reported pregnancy, intent to become pregnant during the study, or breast-feeding (4) Any diseases or condition that could be expected to interfere with the safe completion of the study (5) History of antibiotic use in the previous 3 months (6) Individuals with orthodontic appliances or prosthetic appliances that would interfere with evaluation 6) using tobacco products in any form (7) allergy to chlorhexidine or any of the components in the tested products, (8) systemic diseases (e.g., diabetes mellitus, hypertension and immunological disorders).
Subjects were instructed to avoid systemic antibiotic therapy, local antimicrobials and use of toothpastes containing antimicrobial agents. They were also advised to avoid alcohol and tobacco during treatment. Patients received detailed information on the instructions for plaque control including tooth brushing and flossing. All the subjects received the same brand of toothpaste (Colgate® Strong Teeth toothpaste, Malaysia) and toothbrush (Colgate sensitive soft bristle toothbrush, Malaysia) during the study period.
Randomization and allocation concealmentA total of 45 patients were randomly assigned into one of the three different groups (n = 15 each) using computer generated random allocation sequence (D.P): Group 1 PR mouthwash; Group 2 included CH mouthwash; and Group 3 included PL mouthwash. The random allocation was concealed by having a person not involved in the study. The clinician who performed all measurements was blinded to the treatment arms to the patients (S.G). The randomization codes were not broken until data had been collected. As the study design was a crossover utilizing Latin square design; each group was exposed to all three interventions in a phased manner (block randomization) as shown in Fig. 2. During phase I, three mouth rinses were randomly allocated to three different groups using the lottery method. Further, in phase II and phase III, the groups follow the sequence as shown in Fig. 2 as it is Latin square design.
Fig. 2
Latin square cross-over design depicting sequence of order for all the three groups
Rinse formulationRinse formulation: Propolis rinse 5% was prepared in the College of Pharmacy, MAHSA University. The formulation included 5% propolis, mint flavour, propylene glycol, sorbitol, and water. Propolis rinse was made by using propolis from Malaysia (NHF, Malaysia). The placebo rinse was prepared like propolis mouth rinse except the active ingredient propolis. Readily available Oradex antibacterial mouthwash [(0.12% chlorhexidine gluconate w/v), Fortune Laboratories Shd Bhd, Selangor, Malaysia] was used as the positive control.
Training and calibrationPrior to the start of the study, five subjects were examined for GI and PI twice within 24-hour interval. The calibration was accepted if the measurements at baseline and the 24-hour interval were close to mean score of 0.5 at the 95% level.
Clinical measurementSupragingival plaque and gingival inflammation were assessed by full mouth Silness and Loe Plaque index (PI) [24] and Loe and Silness Gingival index (GI) [5]. Both the clinical parameters were measured at baseline and 3 weeks after intervention by one examiner who was calibrated for PI and GI by Kappa index which resulted in agreement of 0.85 and 0.87 respectively [25].
Intervention protocolThe mouth rinses namely, 0.12% Chlorhexidine mouth rinse, Placebo mouth rinse (self-prepared), and 5% Propolis mouth rinse (self-prepared) constituted three interventions.
Subjects were instructed to rinse for 21 days [26], twice daily, morning after breakfast and night before going to bed, with 10 ml (undiluted) of the assigned mouth rinse for 1 min and then expectorate the rinse. A measuring cup was provided to all the subjects to dispense 10 ml of the assigned mouth rinse. All the subjects were instructed to avoid drinking or eating for minimum of half an hour after rinsing. On day 22, subjects were instructed to rinse once in the morning after breakfast. The use of mouth rinse was followed by a washout period of 15 days during which participants were asked to stop using the assigned mouth rinse. After the washout period of 15 days the selected subjects were assigned to the next mouth rinse in a phased manner (Fig. 2). During the entire course of the study, all the participants received Colgate toothbrush and Colgate total toothpaste and they were instructed to brush twice daily, once in the morning after breakfast and once at night after dinner.
ComplianceAll the participants included in the present study received a checklist to note and record the assigned mouth rinse for 21 days, along with timings (morning and night) to monitor compliance with the use of mouth rinse. The checklist also had an additional column to record any side effects experienced during the intervention period.
Sample size calculationSample size calculation for randomized controlled trial was determined to be 15 in each group which would provide a power of 80% and level of significance at 5% with expected mean difference of 2.281 and standard deviation of 2.563. Based on the above calculation, the minimum sample of 12 is required in each group. Considering an attrition of 20%, 15 subjects in each group and a total of 45 subjects were recruited.
Statistical analysisThe data was cleaned, coded, and analyzed using Statistical Package for Social Science (SPSS) version 27 (SPSS Inc., Chicago, IL, USA). The normality of data was checked using the Shapiro Wilk test with p > 0.05, indicating fulfilment of the normality assumption. Paired-t test was performed to assess the significant difference between baseline and after intervention for both plaque index and gingival index for PR, CH, and PL groups. Analysis of variance (ANOVA) was performed to compare the significant difference in the mean plaque and gingival sore between PR, CH, and PL groups. Post-hoc test was performed using the Bonferroni method to determine statistically significant difference between the two groups. p < 0.05 was considered for statistical significance.
Comments (0)